
Abstract
A 43-year-old male patient with advanced colon carcinoma presented with disseminated staphylococcus aureus bacteremia and central venous catheter associated septic thrombosis of the superior vena cava. Despite appropriate antimicrobial therapy and surgical debridement of distant foci, bacteremia persisted, so an endovascular thrombectomy was performed. Contrary to the usual application, the Capturex® peri-interventional cava filter was positioned upside down, in the direction of the blood flow, in the superior vena cava to prevent septic embolism during mechanical thrombectomy. The wall-adherent septic thrombus was mechanically detached using a RAT fragmentation basket® followed by Aspirex® rotational thrombectomy. Final phlebography showed complete thrombus removal. Small thrombus fragments could be demonstrated in the filter after retrieval. The adapted technique of a reverse positioning of the Capturex® filter in the superior vena cava seems feasible and effective.
Keywords
Introduction
Septic thrombosis and septic pulmonary emboli are serious and potentially life-threatening complications of deep vein thrombosis (DVT). 1 Septic thrombosis of the superior vena cava (SVC) is usually associated with central venous catheter placement. 2 Catheter-related septic thrombosis should be suspected in patients with persistent bacteremia after 72 h of appropriate antimicrobial therapy. 3 Standard treatment consists of catheter removal and targeted antimicrobial therapy. Due to lack of comparative trials, the role of anticoagulation therapy remains unclear and is based on a case-by-case decision.3–6 If conservative management fails, alternative therapies may include percutaneous mechanical thrombectomy or thrombolytic therapy as an alternative to invasive surgical thrombectomy. 7 The application of a peri-interventional cava filter Capturex® (Straub Medical AG, Wangs, SG, Switzerland) as protection device during thrombectomy in the inferior vena cava was performed in the past.8–10 We describe an upside-down positioning of the peri-interventional cava filter Capturex® during percutaneous mechanical thrombectomy of a septic thrombosis of the SVC.
Case report
A 43-year-old male patient with advanced colon carcinoma presented with a staphylococcus aureus bacteremia of unknown origin. A computed tomography (CT) scan revealed a septic coxitis on the left side as well as thrombus around the shaft of a central venous catheter in the SVC. The catheter was removed and an appropriate antimicrobial therapy as well as anticoagulation were initiated. After the surgical removal of the port-a-cath, the initial intravenous heparin therapy was switched to enoxaparin. Despite surgical debridement of the septic coxitis, bacteremia and sepsis persisted. Moreover, follow-up CT scan showed considerable clot progression adherent to the wall of the in the SVC (Figure 1). Based on this finding, septic thrombosis was suspected as focus of persistent bacteremia and the decision for an endovascular thrombectomy was made. To limit risk of a septic clot embolization during the procedure, a peri-interventional cava filter was used. A right transjugular venous access using a 10 French Avanti® sheath (Cordis, Hialeah, FL, USA) and a transfemoral access using a 60 cm 10 French sheath from the Capturex® filter were established. A transjugular phlebography was performed identifying the clot in the SVC (Figure 2(b)). Transfemorally, the peri-interventional filter was positioned in the SVC (Figure 2(a)), which was later slightly retracted to avoid interference between the filter and the RAT fragmentation basket. Via transjugular access, a mechanical shaving of a wall-adherent, organized thrombus was achieved using a RAT fragmentation basket® (Bard, Covington, GA, USA) (Figure 2(c)), which showed incomplete therapeutic success. Finally, via transjugular access a 10 French rotational mechanical thrombectomy device Aspirex® (Straub Medical AG, Wangs, SG, Switzerland) was used. After consecutive thrombectomy runs, successful clot removal was demonstrated (Figure 2(d)). After retrieving the peri-interventional cava filter, residual clots captured inside the filter were visible (Figure 3). The thrombectomy was tolerated well; vital signs and respiratory parameters remained stable during and post procedure. Gram staining of the retrieved blood clot revealed leucocytes but no bacteria and bacterial culture remained without growth. This might have been caused by sampling error or long-term antibiotic therapy. No histopathological analysis of the clot was performed. Blood cultures showed no bacterial growth after the procedure, and antimicrobial treatment was continued for 6 weeks. Continuation of therapeutic anticoagulation with enoxaparin (Clexane®, Sanofi-Aventis, Vernier, GE, Switzerland) was recommended for a total of 3 months. This multi-morbid patient could be transferred to a regional hospital for further treatment in good general condition.
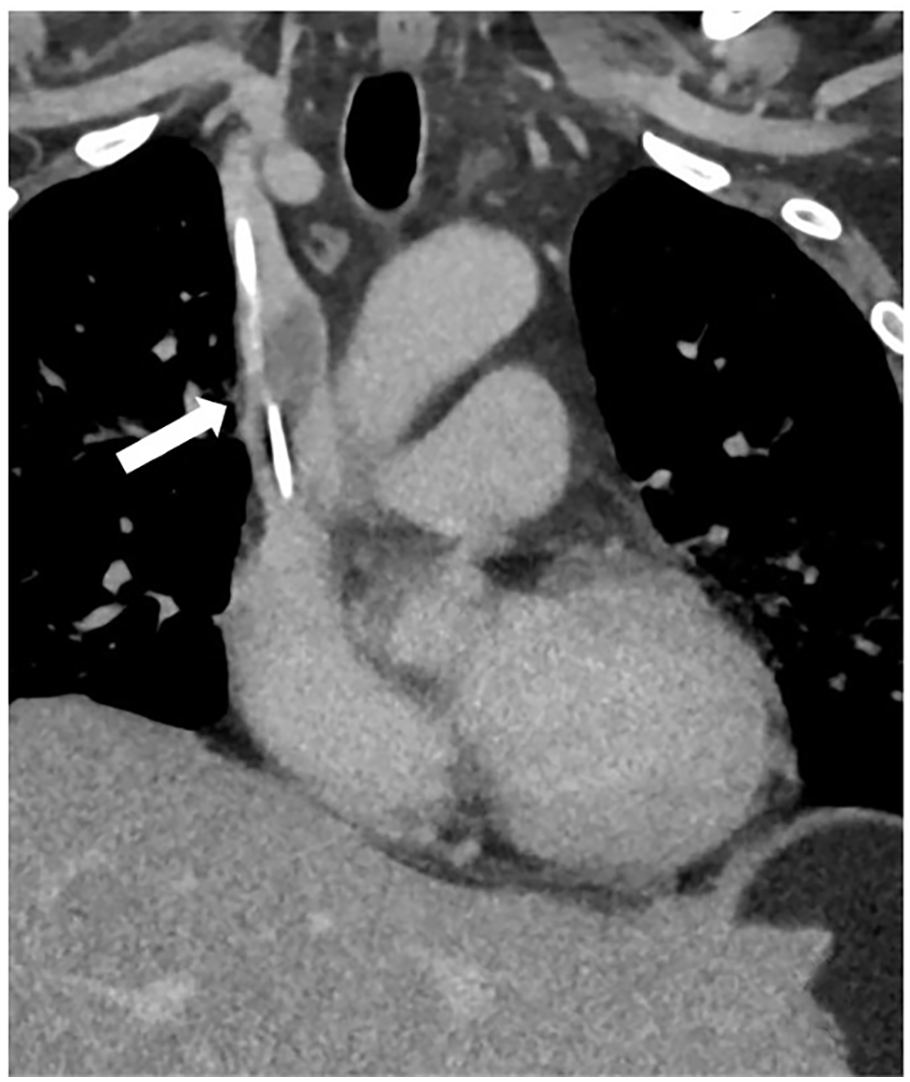
Computed tomography showing a central venous catheter in the superior vena cava with associated thrombus (arrow).

(a) Fluoroscopy showing the Capturex® filter placed in the superior vena cava (arrow). (b) Phlebography of the superior vena cava showing thrombus (arrow). (c) Fluoroscopy showing the fragmentation basket (arrow) used to detach wall-adherent thrombus followed by rotational thrombectomy using the Aspirex® device (not shown). (d) Phlebography demonstrating thrombus removal and venous patency.

After retrieving of the peri-interventional cava filter Capturex® clots caught in the filter were visualized.
Discussion
Septic thrombosis bares risk of embolization, peripheral abscess formation, pulmonary embolism, and endocarditis; therefore, consequent and aggressive management is required. 11 When conservative management fails, therapeutic options include surgical and endovascular thrombus removal. Endovascular options of thrombolysis and mechanical thrombectomy have been proven effective in the past.12,13 In general, the risk of peri-interventional embolization during endovascular thrombectomy is known, but rarely has clinical consequences. However, embolization remains a concern with risk of septic pulmonary embolism and endocarditis in fragile patients. To reduce risk of periprocedural embolization, the use of a peri-interventional vena cava protection filter that remains attached to a delivery catheter can be considered.8,9 Conventional temporary cava filter have been used in the SVC before, but need a second intervention for retrieval.14–16 As solely, a peri-interventional embolization protection was necessary in this setting, we preferred using the peri-interventional filter over a conventional removable cava filter. Use of the Capturex® cava filter in an inverse upside-down position in the SVC has not been described before and offers the advantage of an easy and quick filter removal in the same session.
Conclusion
Upside-down positioning of the Capturex® filter in the SVC was feasible, safe, and effective. This procedure can be useful and indicated in specific high-risk patients when, first, thrombectomy of the SVC or the veins of the upper extremities is required and, second, the risk of periprocedural embolization has to be minimized. Among these high-risk patients are patients with a relevant patent foramen ovale and patients with septic thrombosis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.