
Abstract
This case report presents a rare instance of facial vein thrombophlebitis, a potentially serious complication, following a facial skin infection. A 33-year-old man known to have cerebral palsy, epilepsy on ventriculoparietal shunt, and kyphoscoliosis presented to the emergency department complaining of small facial wound and swelling for 1 week. The wound failed topical management and fever started to develop. His medications included quetiapine and levetiracetam. Investigations, including computed tomography, were carried out to rule out an extension to deep tissue. Management in the emergency department involved initial resuscitation with 500 mL of 0.9% normal saline and 1 L of lactated ringers, antibiotic coverage with piperacillin/tazobactam and vancomycin was given, and analgesia for pain control. This case highlights the potential for facial vein thrombophlebitis as a complication of facial skin infections. Early diagnosis and prompt initiation of appropriate management are crucial to prevent potentially fatal consequences.
Introduction
Septic thrombophlebitis (STP) is defined as the presence of a vascular thrombus in the setting of an infection. Its clinical presentation varies. It can present as a localized inflammation or with severe systemic manifestations which could be associated with septic shock. Majority of the cases are incited by an initial break in the skin either from a traumatic event or due to medical interventions such as intravenous catheters. Another subset of cases is caused by invasive infections from adjacent structures. A classic example is Lemierre’s syndrome which is thrombophlebitis of the internal jugular vein caused by oropharyngeal infections most commonly pharyngitis, 1 which is potentially a life-threatening disease with a reported mortality of up to 17%. 2
STP can occur in any vascular structure superficial or deep without preceding interventions. STP usually is clinical diagnosis and considered to be benign and commonly related to varicose veins which are treated conservatively. Some are related to deep vein thrombosis which is treated with anticoagulants and thrombectomy. 3 Risk factors include extremes of age, active malignancy, and immunosuppression, burn victims, and patients receiving total parenteral nutrition.4,5 STP of the deep venous system is less common; however, it is commonly associated with central venous catheters.6,7
The facial vein is part of the superficial venous system of the face and provides its primary drainage. It starts at the medial angle of the eye where it communicates with the superior ophthalmic vein and terminates into the internal jugular vein near the level of hyoid bone. 8 It is rarely involved in STP.
We performed a literature review of reported cases using the MEDLINE database and Google Scholar. The search was performed in English using the terms: facial vein, facial vein thrombosis, facial vein STP, and Lemierre’s syndrome. A systematic review by Paker et al. of cases till 2018 found only 11 reported cases. The primary source was an ear, nose, and throat infection. All cases presented with fever and neck swelling. Microbiological analysis revealed four positive cases of Staphylococcus aureus, one case of Streptococcus constellatus, and one case of Fusobacterium necrophorum. The rest of the cases were either not done or negative cultures. Eight patients were anticoagulated, while five were not. No mortality was documented in both groups. 9
Until now, only a few cases of facial vein thrombosis are reported in the literature with controversies in its diagnosis and management. Here, we present a case of periorbital cellulitis complicated with facial vein thrombosis that was successfully managed with conservative treatment, including anticoagulation and antibiotic therapy.
Case
A 33-year-old man with a history of cerebral palsy, epilepsy on ventriculoparietal shunt, and kyphoscoliosis presented to the emergency department (ED) complaining of left facial swelling for 1 week. His family initially noted a small wound around the left eye with no clear cause, which they tried to treat with topical antibiotic ointment. However, the wound did not improve, and swelling developed around the wound, extending to the left half of his face. He also started to develop fever. He denied having dyspnea, vomiting, diarrhea, or any recent dental procedure. His medications included quetiapine and levetiracetam. The patient is not known to have any allergies.
On examination, vital signs were blood pressure 112/89 mm/Hg, heart rate 168 beats/min, respiratory rate 30, oxygen saturation 91%, and temperature 38.2 °C. His airway was intact without any intraoral or tongue swelling. He had left-sided perioral swelling, which was warm to the touch with erythema and honey crust exterior. The swelling extended to the left side of the face (Figure 1). The submandibular area was soft, without swelling or tenderness.

Left-sided facial swelling with signs of cellulitis.
Ophthalmological examination showed intact visual acuity. Extraocular movements were intact with no associated pain. Pupils were equal in size and reactive bilaterally. There was no conjunctival injection or photophobia. Periorbital skin was swollen and erythematous. During the patient’s stay in the ED, the initial impression was impetigo/cellulitis in addition to periorbital cellulitis.
In the initial resuscitation period, a chest X-ray showed a left-sided pleural effusion and the development of patchy bilateral opacities (Figure 2). Electrocardiography (ECG) and venous blood gas (VBG) tests were also performed. The ECG showed sinus tachycardia, and the VBG results revealed pH 7.48, pCO2 36.4, HCO3 26.7.
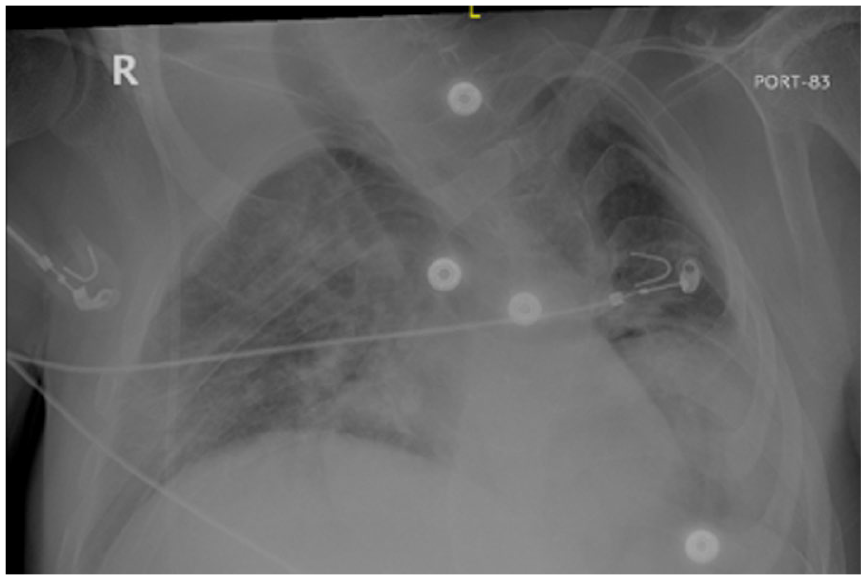
Supine chest X-ray Anteroposterior (AP) view showing left-sided pleural effusion, development of patchy bilateral opacities.
Initial laboratory tests included a complete blood count (CBC), basic metabolic panel, coagulation profile, lactic acid, erythrocyte sedimentation rate (ESR), procalcitonin (PCT), blood culture, urinalysis, and urine culture. Relevant results include leukocytosis of 17.6, lactic acid 3.35 mmol/L, PCT 12.88 ng/mL, ESR 53 mm/h.
Given the severity of his initial presentation, computed tomography (CT) of the brain and face was obtained to rule out deep tissue extension. The enhanced CT scan of face and brain showed marked facial swelling and enhancement more on the left side with subcutaneous fat stranding and edema extending to the left periorbital/pre-septal region and medial canthus. There was no evidence of central nervous system extension. There were multiple enlarged cervical and submandibular lymph nodes. The left facial, periorbital, and upper lip swelling was likely indicative of cellulitis with left facial vein thrombosis, with the internal jugular vein being spared (Figure 3).
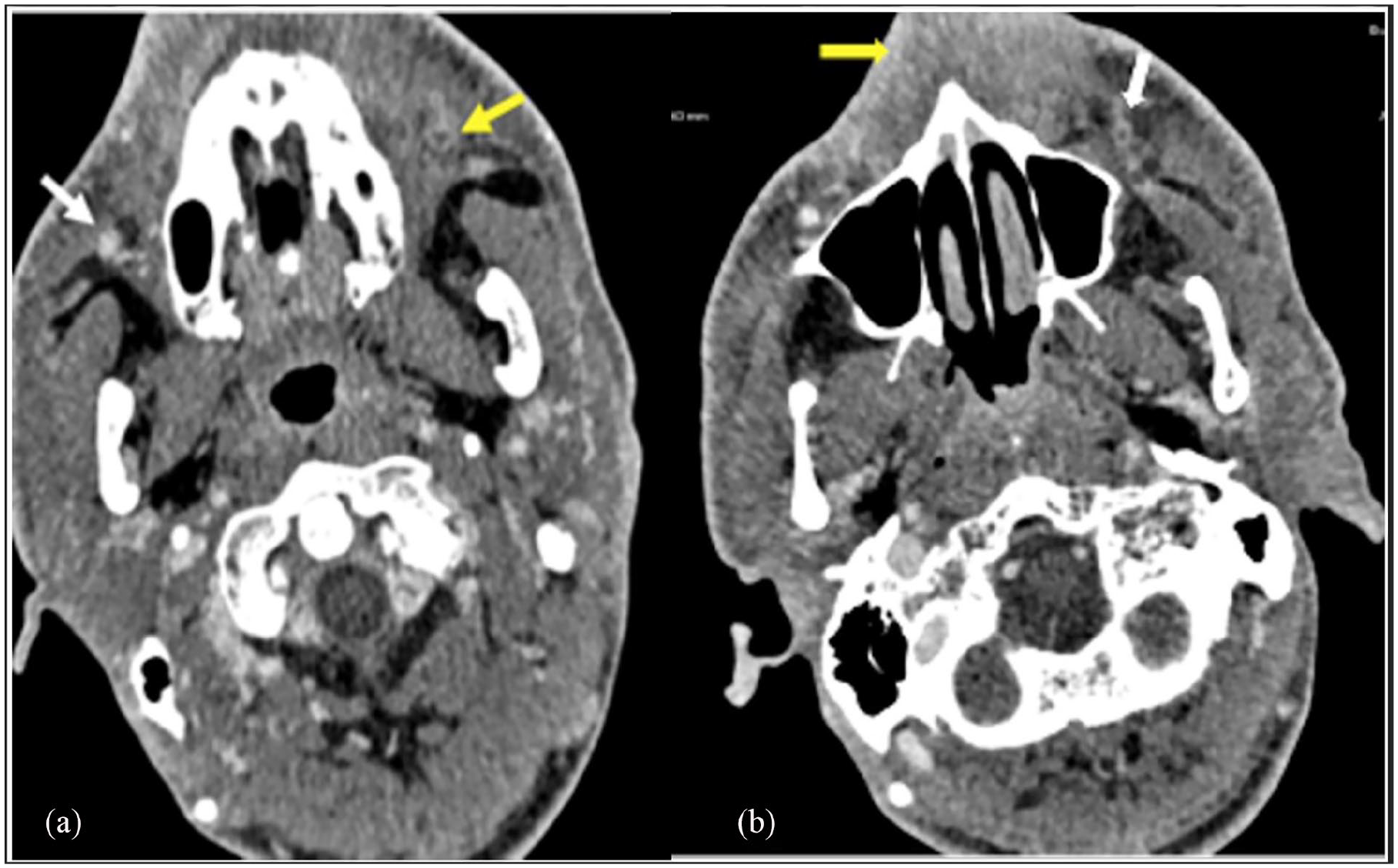
(a) Axial CT of the face showing left facial vein thrombosis (yellow arrow), normal appearance of the right facial vein (white arrow). (b) Axial CT of the face showing left facial vein thrombosis (white arrow), left side with subcutaneous fat stranding and edema (yellow arrow).
In the ED, the patient was connected to an oxygen source via nasal cannula and was able to maintain 100% oxygen saturation. He received initial resuscitation with intravenous fluids (500 mL of 0.9% normal saline and 1 L of lactated ringers), and his heart rate subsequently improved to 115 beats/min. Empiric antibiotic coverage included piperacillin/tazobactam and vancomycin was given, along with analgesia for pain control. After reviewing the patient’s clinical condition and CT findings, he was admitted under internal medicine service.
During the hospital stay, the patient was started on heparin infusion and continued broad spectrum antibiotics. The results of the blood and urine cultures were positive for methicillin-resistant Staphylococcus aureus (MRSA); hence, it was sensitive for vancomycin, gentamicin, and clindamycin, and it was resistant to oxacillin and cefazolin.
The infectious diseases team was consulted as a case of complicated MRSA bacteremia due to facial cellulitis with facial vein thrombosis. Their recommendations were to continue vancomycin and discontinue piperacillin/tazobactam and daily blood cultures. This vancomycin trough was achieved by a dose of 1 g every 8 h. The vancomycin course was recommended to be continued for 14 days after the first negative culture. They also requested additional images, including transesophageal echocardiography (TEE) to rule out infective endocarditis and a full-body CT to rule out the seeding of infections. TEE was technically difficult due to the patient’s facial swelling and concern for airway compromise with sedation. Therefore, transthoracic echocardiography was performed and was unremarkable. A chest CT showed focal caveating consolidation and multiple cavitating pulmonary nodules, which could represent septic emboli (Figure 4). The abdominal CT was unremarkable.

Axial chest CT showing two different sections showing multiple cavitary lesions in the right lung.
The hematology team was consulted and they recommended starting enoxaparin 1 mg/kg subcutaneously twice a day during admission and transitioning to apixaban 5 mg twice daily after discharge for a total of 3 months.
After 18 days of admission, the patient was clinically stable and fit for discharge. He was discharged on linezolid 600 mg orally twice daily for another 2 weeks to complete a total course of 4 weeks for his complicated MRSA bacteremia. One month after discharge, we contacted the patient’s brother who reported that the patient is back to his normal state of health, with the facial swelling having subsided.
Discussion
This case highlights the complexity of investigating soft tissue infections, which are a common presentation in ED settings. Examples of common ED head and neck soft tissue infections include cellulitis, impetigo, erysipelas, and periorbital cellulitis. Most infections can be treated with oral antibiotics and outpatient follow-up. However, certain features should alert the physician to investigate for possible complications, including STP, which is considered as one of the most serious complications due to its high mortality rate if left untreated. 1 These features include presenting with systemic manifestation, failure to respond to outpatient antibiotics, or in the setting of immunocompromise. In this case report, the patient presented with systemic manifestations that prompted suspicion for further complications associated with his periorbital and facial cellulitis.
This presentation is rare, and only a few cases are reported to date. A previous literature review by Paker et al. identified 12 cases until 2018. We found eight more cases in our literature review. Two cases were related to dental disease or post dental extraction,10,11 one case was related to periorbital cellulitis, 12 three tonsil-related infections,13–15 one preseptal cellulitis, 16 and one submandibular sialadenitis case. 17 Blood cultures and relevant tissue cultures were taken from all cases. Particularly, three cases were positive for MRSA, two cases were positive for F. necrophorum, whereas the rest had either a negative culture or the result was not mentioned. Septic emboli were observed in seven cases, all of which traveled to the lungs. One case also involved the brain, and one case did not have any distant involvement. Treatment for all cases was a course of intravenous antibiotics. Five of the eight cases were anticoagulated. As for the surgical interventions, only two cases required surgery. One of which had pneumonia/pleural effusion attributed to septic emboli that did not respond to thoracentesis. The cardiothoracic surgery team was consulted, and they decided to perform left anterior thoracotomy with a pericardial window and drain placement, and a right video-assisted thoracoscopic surgery, which was converted to a right open thoracotomy with hematoma evacuation and decortication. 14 The other case was complicated by the progression of the facial vein thrombosis to the cavernous sinus, which led to bilateral internal carotid artery stenosis and endarteritis, which ultimately resulted in bilateral Middle Cerebral Artery and Anterior Cerebral Artery emboli and watershed infarctions. The patient’s condition deteriorated with worsening ventriculitis and suspected watershed infarcts secondary to bilateral Internal Carotid Artery (ICA) stenosis, necessitating neurosurgical intervention with right ICA stenting. The patient also had bilateral pulmonary septic emboli due to thrombophlebitis in the internal jugular veins. Unfortunately, due to the patient’s ongoing sepsis and poor neurological outcome, hospice care was initiated, and the patient passed away 3 weeks later. 16 All cases except one experienced full recovery without any reported mortality. Table 1 provides a summary of the abovementioned cases including age, gender, primary source.
Summary of the facial vein thrombophlebitis cases.

MRSA, methicillin-resistant Staphylococcus aureus; HCV, Hepatitis C Virus.
Our patient’s investigations and management were similar to the previously reported cases. He underwent a full assessment to investigate seeding infections. A chest CT revealed findings that could be representative of septic emboli. Blood and urine cultures were positive for MRSA. The patient received a full course of antibiotics, primarily vancomycin, and anticoagulation therapy. Initially, he was started on a heparin infusion, then followed by enoxaparin during hospitalization, with a recommendation to switch to apixaban after discharge. At the 1 month follow-up, his family reported that the patient has made a full recovery.
To address the controversy on the use of anticoagulation in such cases, the diagnostic aspect should be considered. In other words, a closer look at this presentation to determine if it is a variant of Lemierre’s syndrome might help in the management approach. Classically, Lemierre’s syndrome would present in sepsis preceded by pharyngitis, thrombosis of internal jugular vein and its tributaries, and metastatic septic embolism.18,19 Based on a systematic review of Lemierre’s syndrome, anticoagulation use is an option depending more on the patient’s status and hospital protocols. 20 In our case, there was neither prodrome pharyngitis nor extension to the internal jugular vein as the contrast-enhanced CT revealed. Similarly, in two studies, the names Lemierre-like syndrome and Lemierre’s syndrome variant were given to the cases where the thrombus was in the facial vein with no preceding pharyngitis.10,21 Both cases considered Lemierre’s syndrome as a possible diagnosis and did not include anticoagulants in the management arguing that the internal jugular vein was intact, and the anticoagulant therapy should be used if the deep veins are involved besides the lack of clinical trials of anticoagulation therapy in this setting.10,20,21 Other studies similar to the present case, however, suggested that anticoagulation should be used to prevent further complications of the emboli.22–24 Despite scarce case reports and the lack of controlled clinical trials on the role of anticoagulants in these cases, consistent treatment outcomes support adapting similar treatment regimen if such a presentation is encountered in the future. 1
Conclusion
Facial vein thrombosis and thrombophlebitis can complicate facial soft tissue, ENT, and odontogenic infections. Its complications include bacteremia and septic embolism, especially to the lung, and the treatment should be directed at appropriate antibiotic therapy. While anticoagulation may be controversial, its use can be associated with clinical benefit and improvement.
Footnotes
Acknowledgements
None.
Correction (February 2025):
Author contributions
All authors contributed equally in every step of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.