
Abstract
Septic thrombophlebitis of the internal jugular vein (IJV), known as Lemierre’s syndrome, is a rare complication secondary to infections in the head and neck. Cholesteatoma of the middle ear complicated with Lemierre’s syndrome is rarely observed in clinical practice. Currently, the treatment controversy centers on whether anticoagulation therapy is necessary for IJV and distant metastatic emboli induced by Lemierre’s syndrome. A 46-year-old female patient with middle ear cholesteatoma underwent modified radical mastoidectomy and tympanoplasty surgery and complicated with Lemierre’s syndrome, presenting with intermittent high fever, chills, headache, and left lateral neck pain. Computed tomography (CT) revealed thrombosis and internal gas in the left IJV, while blood culture and blood pathogenic microorganism metagenomic detection were negative. We administered sodium ceftriaxone (1 g every 12 hours) for 3 days. According to the secretion culture results showing 90% Actinomyces europaeus and 10% Corynebacterium without mycolic acid, penicillin (2.4 million IU) was added intravenously every 6 hours. The patient’s infection worsened on the first day after surgery. We adjusted to upgrade anti-infection vancomycin 1 g every 12 hours, combined with meropenem (1 g every 8 hours) and metronidazole (0.5 g) every 8 hours for 4 weeks, and subcutaneous injection of enoxaparin 0.4 mL every 12 hours for 1 week, then adjusted to rivaroxaban tablets (15 mg bid). Amoxicillin-clavulanate for 2 weeks and rivaroxaban 10 mg were administered orally for 3 months after discharge. A follow-up neck CT scan with intravenous contrast suggested that the gas in the left IJV had disappeared, but the thrombus persisted. During the 3 month follow-up, the patient’s vital signs, blood routine, and D-dimer levels were within the normal range. The surgical area healed well, and the patient reported no discomfort. Lemierre’s syndrome represents a potentially-fatal complication that results in considerable mortality and must be identified early and aggressively treated.
Keywords
Introduction
Lemierre’s syndrome is a systemic septic embolism caused by thrombophlebitis of the internal jugular vein (IJV), and it arises as a complication of an infection in the region of head and neck, often due to anaerobic septic embolization.1,2 It is a rare disease with an estimated incidence of 1 in 1,000,000 per year, predominantly affecting adolescents and young adults. 3 The most common causative agent is Fusobacterium necrophorum, an anaerobic gram-negative bacillus that is a commensal of the oral flora; however, other pathogens such as Staphylococcus, Streptococcus, Proteus, and Bacteroides can also be responsible. Lemierre’s syndrome is a potentially-fatal complication that results in considerable mortality and must be identified early and aggressively treated.
We present a case of middle-aged female with middle ear cholesteatoma, which resulted in the development of Lemierre’s syndrome. A review of the relevant literature was also conducted.
Case Report
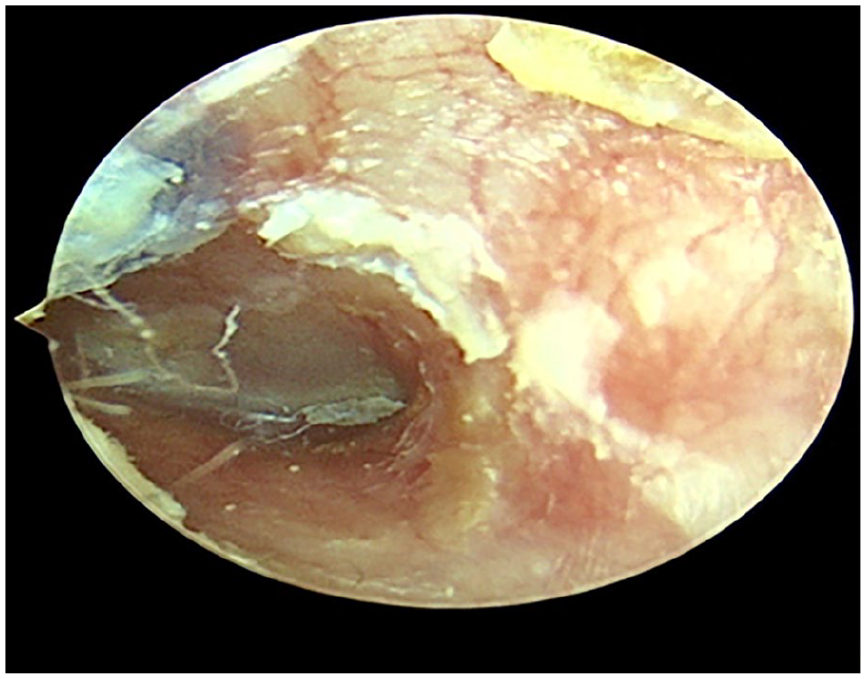
A 46-year-old woman visited the clinic complaining of a “recurrent pus discharge from the left ear accompanied by hearing loss for five years, which aggravated for 12 days.” Five years ago, the patient experienced pus discharge and hearing loss in the left ear along with intermittent headaches on the same side, but there were no symptoms of vertigo, nausea, vomiting, facial numbness, taste disturbances, or unconsciousness. The patient self-medicated, but the condition persisted with recurrent episodes. Twelve days prior to the visit, the symptoms intensified. The patient experienced a single episode of vertigo that lasted several hours, accompanied by nausea without vomiting, and a headache on the left side. Upon admission, the physical examination revealed stable vital signs. Specialist inspection revealed congestion and mild tenderness of the left mastoid skin, as well as cholesteatoma epithelium with yellow scabs and purulent secretions in the left external auditory canal (Figure 1). Tympanic membrane perforation was also observed. The computed tomography (CT) scan (Figure 2) reveals chronic middle ear mastoiditis on the left side, accompanied by osseous destruction and the possibility of cholesteatoma. The anterior wall of the sigmoid sinus is intact. The middle ear magnetic resonance imaging (MRI) reveals left plate impaired mastoid and chronic middle ear mastoiditis, considering cholesteatoma formation. Pure-tone audiometry indicates the average air conduction threshold for the left ear is 78 dB, and the boneconduction threshold is 39 dB. For the right ear, the average air and bone conduction threshold was 20 and 15 dB, respectively. Laboratory evaluation revealed leukocytosis with a white blood cell (WBC) of 11.14 × 109/L (neutrophils 88%) and a platelet count of 415.00 × 109/L. The C-reactive protein level was 51.23 mg/L.
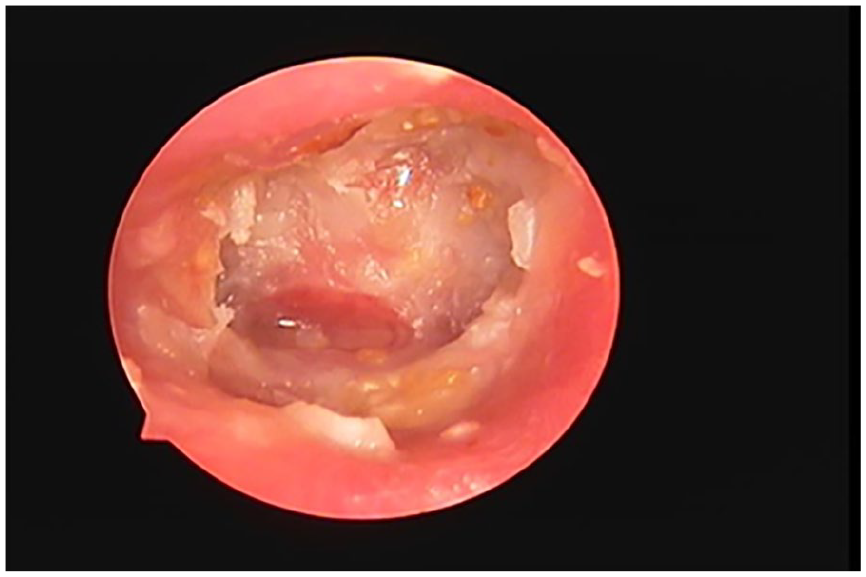
Preoperative endoscopic view of the ear canal showing the cholesteatoma epithelium and secretions.
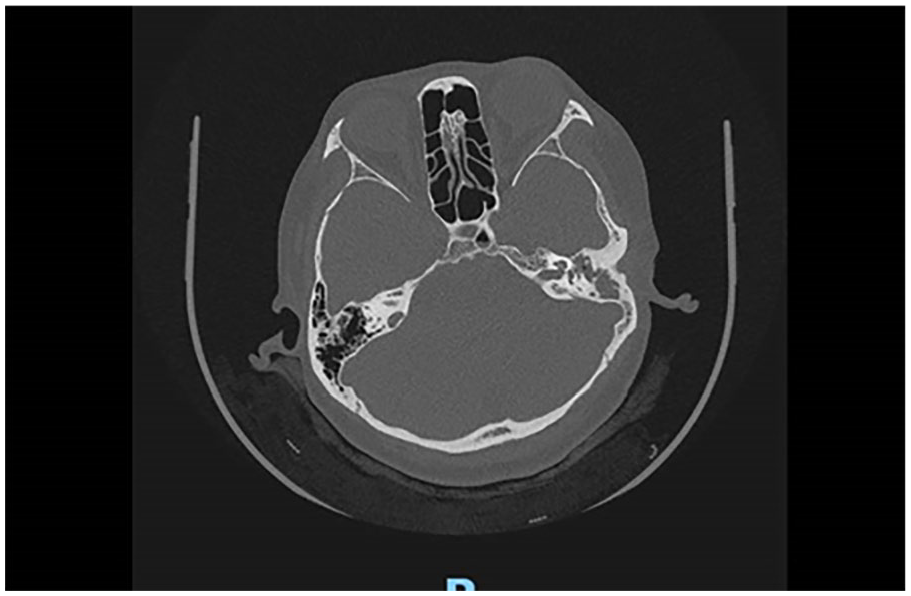
Preoperative temporal bone CT suggests middle ear cholesteatoma with intact sigmoid sinus bone. CT, computed tomography.
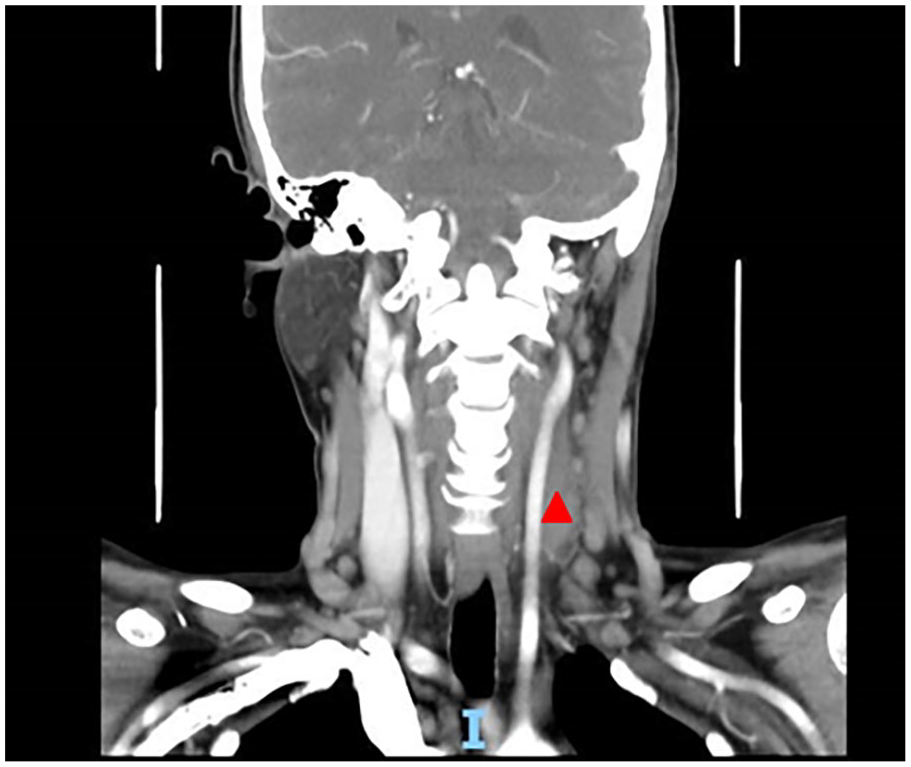
After admission, the patient received intravenous sodium ceftriaxone (1 g every 12 hours) and dexamethasone (10 mg) for anti-infection and anti-inflammatory treatments over 3 days. The secretion culture results showed 90% Actinomyces europaeus and 10% Corynebacterium without mycolic acid. After the skin test, 2.4 million IU penicillin was administered intravenously every 6 hours for anti-infection treatment. The patient was scheduled to undergo elective surgery under general anesthesia, including modified radical mastoidectomy and left ear tympanoplasty. The sigmoid sinus bone was intact, while the tegmen tympani bone was very thin, and part of the dura mater was exposed. The epitympanum, mesotympanum, and protympanum were filled with cholesteatoma. The bone of the horizontal semicircular canal was thinned and showed a blue line, indicating bone erosion. Postoperative treatment included ceftriaxone combined with penicillin for anti-infection therapy. On the first day after surgery, the patient experienced high fever (40°C) and chills, along with paroxysmal throbbing pain in the left head. On examination, no significant redness or abnormal secretions were observed at the incision site (Figure 3). However, slight congestion and tenderness were observed in the skin of the left mastoid area, as well as erythema and tenderness of the left lateral neck. Laboratory results showed a WBC count of 10.36 × 109/L, a platelet count of 458.00 × 109/L, a neutrophil percentage of 83.10%, a C-reactive protein level of 195.73 mg/L, and a Procalcitonin: 0.38 ng/mL. MRI of the head and neck revealed no obvious abnormalities in the skull, with a filling defect in the left IJV and exudation in the perivascular space (Figure 4a and b). CT of the neck with intravenous contrast was performed to evaluate what was thought to be an abscess. The CT revealed thrombosis and internal gas in the left IJV (Figure 5a and b).

Patient with no significant redness or abnormal secretions at the incision site, but left lateral neck erythema and tenderness.
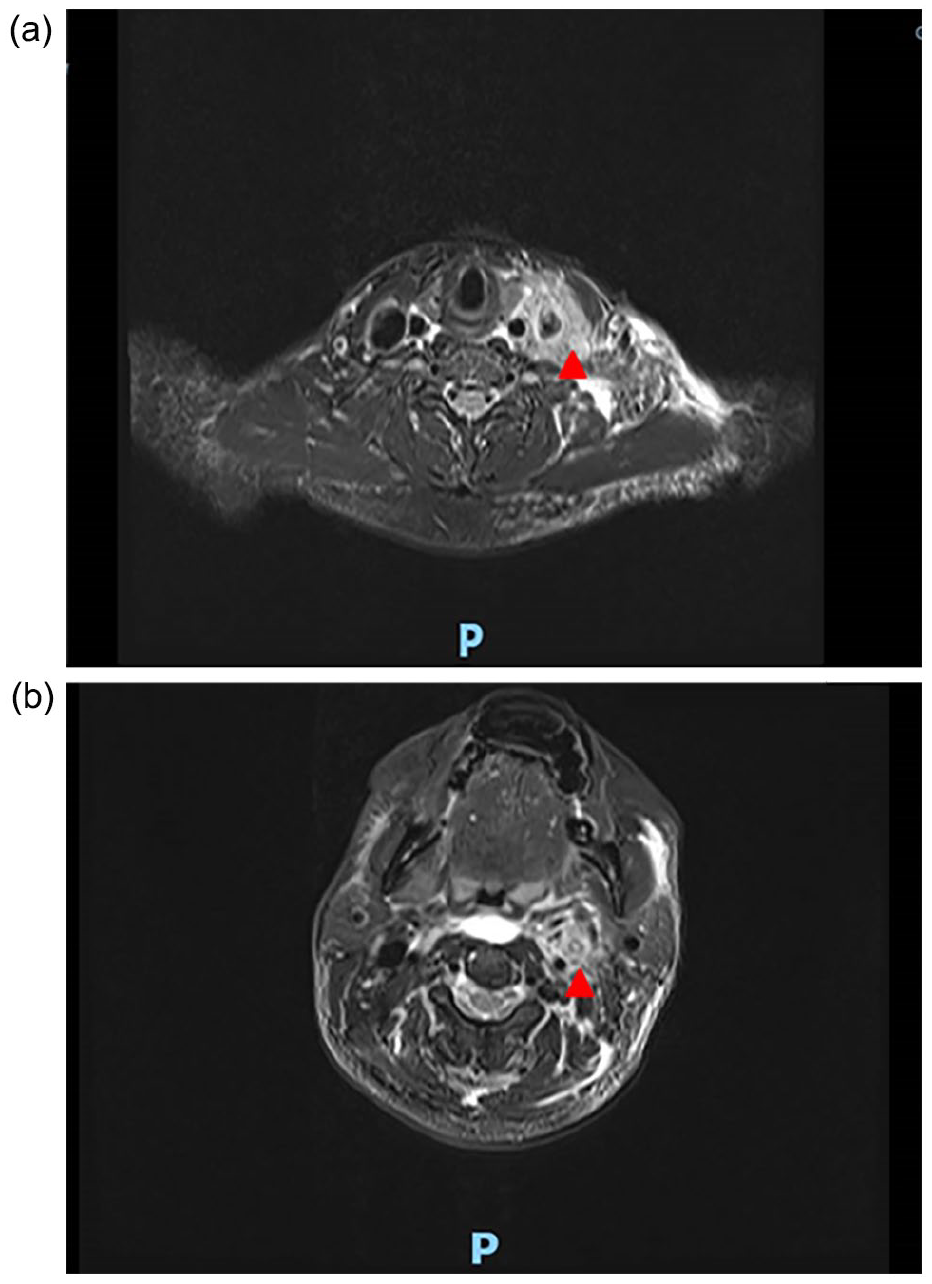
(a, b) Red triangle shows the filling defect in the left IJV. IJV, internal jugular vein.
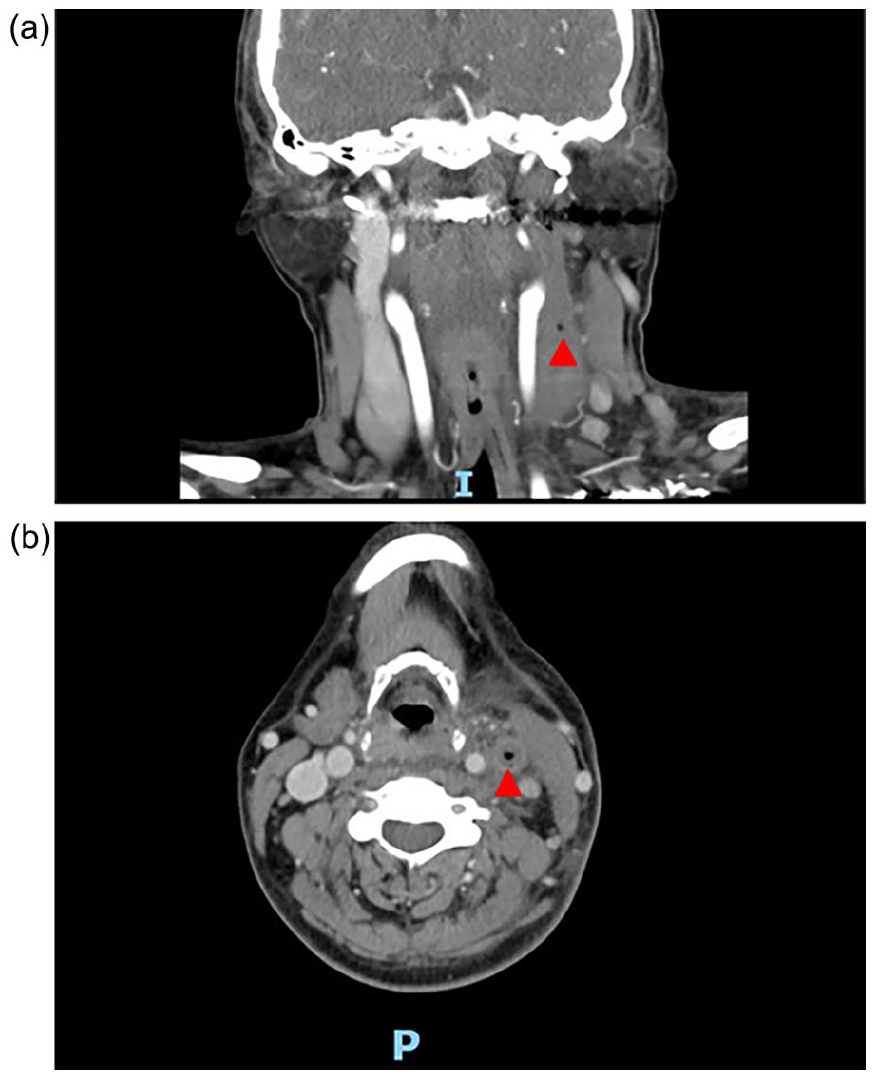
(a, b) Red triangle shows thrombosis and internal gas in the left IJV. IJV, internal jugular vein.
The anti-infective treatment plan was adjusted to upgrade ceftriaxone to vancomycin 1 g every 12 hours, combined with meropenem (1 g every 8 hours) and metronidazole (0.5 g) every 8 hours for anti-infection, and enoxaparin 0.4 mL every 12 hours for subcutaneous injection. Blood culture and blood pathogenic microorganism metagenomic detection were performed, and the results were negative after 5 days. During treatment, the patient presented intermittent fever and left-sided headache until the 10th day postoperation, while other vital signs were stable. The anti-infective treatment plan was modified to remove metronidazole and continued vancomycin + meropenem therapy. The anticoagulation regimen was adjusted to rivaroxaban tablets (15 mg bid). After completing 6 weeks of anti-infective therapy, the patient’s symptoms eased, and relevant laboratory indicators (eg, WBC count, C-reactive protein levels) returned to normal levels (Figure 6a-c). CT of the neck with intravenous contrast suggested that the gas in the left IJV had disappeared, but the thrombus persisted (Figure 7). After discharge, oral amoxicillin-clavulanate was administered for 2 weeks and oral rivaroxaban 10 mg for 3 months. During this period, the patient’s vital signs, blood routine, and D-dimer levels were all within the normal range. The surgical area healed well (Figure 8), and the patient reported no discomfort.
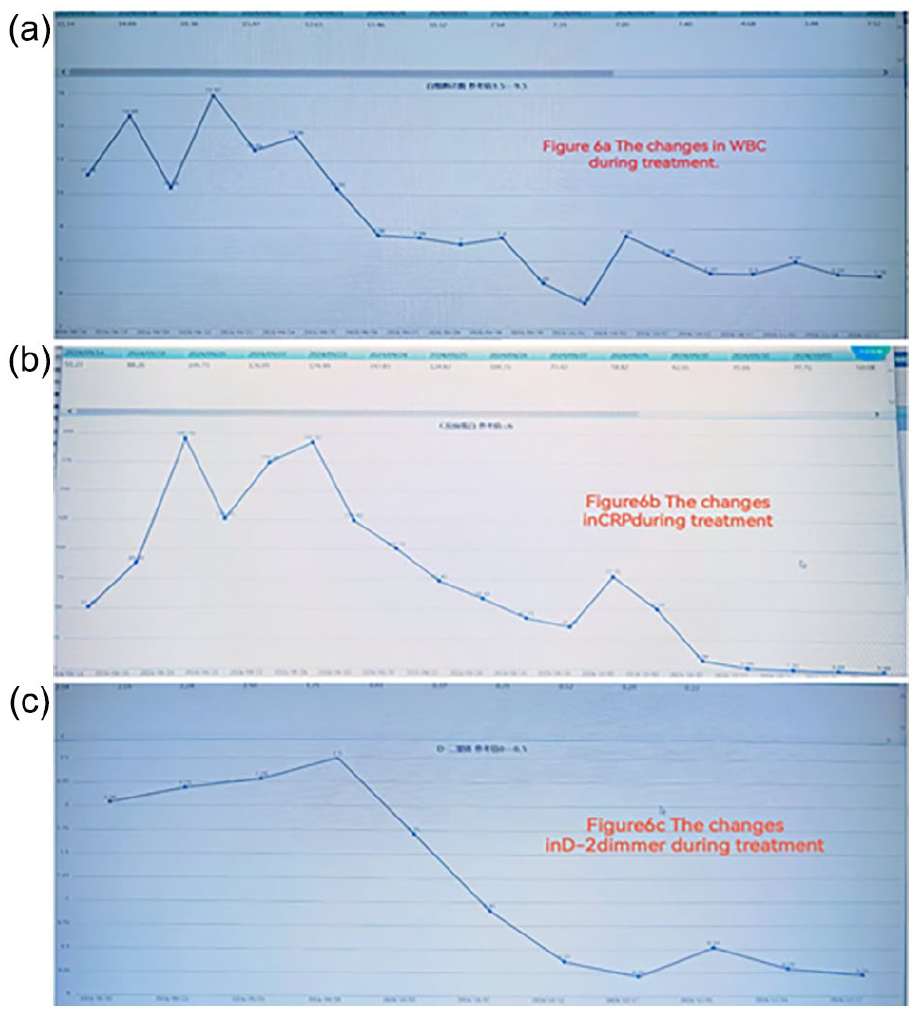
(a-c) WBC, CRP, and D-2dimmer changes during treatment. WBC, white blood cell; CRP, C-reactive protein.
Red triangle shows that the gas in the left internal jugular vein had disappeared, but the thrombus still existed.
Surgical area healed well.
Disscusion
Lemierre’s syndrome is characterized by anaerobic suppurative thrombophlebitis that affects the IJV. It was initially recognized as a complication of pharyngeal infections and has since been associated with various other sources. The progression of the disease can be further complicated by the presence of septic emboli. Reports of Lemierre’s syndrome have declined significantly after the widespread use of antibiotics, with the incidence suggested to be approximately 1 per million. 3 Due to its rarity, there is insufficient clinical understanding of the condition. Treatment typically consists of a prolonged course of antibiotic therapy, initially administered intravenously. The mortality rate in this case series recently reported to be as low as 6.4%. 4 According to a series of cases released in 2005 by Goldenberg et al, the duration of antibiotic treatment ranging from 5 days to 6 weeks. Nine children with Lemire-like syndrome were analyzed, and 7 of them had evidence of thrombophilia, including antiphospholipid antibodies and elevated factor VIII activity. Eight of the 9 children were administered anticoagulants for a median duration of 3 months. At the 1 year follow-up, all patients survived without the recurrence of venous thromboembolism, although 38% showed no resolution of the thrombosis. 5
Lemierre’s syndrome, as originally defined, is more closely related to individuals who are previously healthy and develop suppurative thrombophlebitis following oropharyngeal infection. Nonetheless, considering the analogous pathophysiology of septicemias originating from other sources, such as otitis media or mastoiditis, cases of these origins have also been classified as Lemierre or Lemierre-like syndromes. There are a few reports in the literature on otitis media as a cause of suppurative thrombophlebitis. Recently, Le Monnier et al described 25 cases of middle ear infections due to F. necrophorum infection, 3 of which were consistent with Lemierre’s syndrome. 6 In 2021, Kjellberg et al reported Lemierre’s syndrome caused by F. necrophorum complicated by multiple brain abscesses. 7 In 2023, Tensei Suzuki reported a case of blindness caused by Lemierre’s syndrome. 8
In our case, we did not find F. necrophorum but Actinomyces europaeus in the secretions, and the metagenomic detection of the blood microbiota was negative. Based on clinical symptoms, physical examination, laboratory data, and imaging examinations, the patient was diagnosed with septic thrombophlebitis of the IJV, which is a characteristic of Lemierre’s syndrome. Owing to its rarity, high clinical suspicion is required to establish a diagnosis of Lemierre’s syndrome.
No agent was identified in blood cultures or metagenomic analysis, likely due to suppression by prior antibiotic administration. This deviates from the classical presentation of the syndrome. In terms of anti-infection, ceftriaxone, and penicillin were initially used based on the results of the secretion culture. However, the clinical symptoms worsened, prompting the use of vancomycin, meropenem, and metronidazole for 6 weeks to control the infection. With regard to the anticoagulation, there are a few reports suggesting the benefit of anticoagulation in patients with Lemierre’s syndrome. However, there is currently no clear consensus on the role and efficacy of anticoagulation in preventing septic embolic events originating from IJV thrombosis. 9 In recent reviews, only 21% to 30% of affected patients were treated with anticoagulation therapy. 10 However, anticoagulation has previously been recommended in acute settings or for patients with extensive thromboses. It is also recommended for cases where thromboses display retrograde progression to the cavernous sinus.11-13 Our patient underwent heparin anticoagulation followed by rivaroxaban and experienced no evidence of secondary septic embolism. Therapeutic anticoagulation was performed for 3 months. Finally, completd clinical recovery was achieved.
Conclusions
We present a rare case of middle ear cholestoma in a patient who developed Lemierre’s syndrome after mastoidectomy, and very few cases have been reported. Clinicians must recognize that it is a serious condition that can lead to death in some cases. In our case, adequate and full-course antibiotic and anticoagulant treatment led to patient recovery.
Footnotes
Author Contributions
Conceptualization: Z.X.; Data Curation: Z.X.; Formal analysis: D.H.; Investigation:Z.X., D.H.; Methodology: Y.M., Z.Y.; Project administration: Z.C.; Resources: Z.X., D.H.; Supervision: C.Q.; Validation: W.Y., J.J.; Visualization: Z.X., D.H.; Writing – original draft: Z.X.; Writing – review & editing: Z.X.
Data Access Statement
All relevant data are within the paper and its Supporting Information files.
Data Availability Statement
Data sharing is not applicable to this article as no new data were created or analyzed in this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This studeywas funded by Science and Technology Program of Guizhou Province (Qiankehe Basics ZK [2024] Common 410); Guizhou Province’s 14th Five-Year Plan Key disciplines of Traditional Chinese Medicine and Ethnic Medicine (QZYYZDXK (PY) -2021-06). This study was supported by a grant from the Research Projects on Traditional Chinese Medicine and Ethnic Medicine of the Provincial Administration of Traditional Chinese Medicine from the Foundation of Basic Research (QZYY-2023-026). This study was conducted under the research program of the First Affiliated Hospital of Guizhou TCM University. Zhu Xiaoyu was supported by a grant from this ministry.
Ethical Compliance
Written informed consent for the publication of this case report was obtained from the patient. Also, the First Affilated Hospital of Guizhou TCM university’s Ethics Committee approved the submission.