
Abstract
Introduction
Bell’s palsy (BP) is the most common type of peripheral palsy of the facial nerve and accounts for about 60% of all cases. The annual incidence of BP varies between 8 and 52.8 new cases per 100,000 individuals.1,2 BP affects a significant portion of the population, with a 1-in-60 chance of developing the disease in one’s lifetime, with higher occurrence rates noted during pregnancy and in individuals with diabetes mellitus.1,3 The condition is believed to be potentially caused by ischemic compression of the facial nerve within the meatal segment of the facial canal. 4
BP presents as unilateral abrupt weakness or paralysis of facial muscles, frequently accompanied by mild discomfort, numbness, increased sensitivity to sound, and altered taste perception. 5 Infectious, immunological, and ischemic processes are all implicated in the pathogenesis of BP. 6 The most probable explanation remains viral, suggesting that neurotropic herpes simplex viruses 1 and 2 and varicella-zoster viruses reactivate in the geniculate ganglion. 7 Furthermore, other viral infections and autoimmune diseases have also been proposed as potential pathomechanisms. 8
In approximately 71% of untreated cases, the disease resolves completely.1,3 Treatment involves high doses of corticosteroids and antiviral agents, although there is limited evidence of the efficacy of the latter. 9
Recurrent BP is a rare condition that may affect the same side or the opposite side of the face that was affected in the primary episode. The incidence of recurrent facial palsy is 2.6% to 15.2% in patients who already had a primary episode. 10 Although recurrent BP has been associated with systemic comorbidities such as diabetes and hypertension, the exact relationship and underlying mechanisms remain subject to further investigation. 11 Its prognosis is unclear, as the classification of the degree of palsy is not uniform between studies. It is not known whether the pathogenetic mechanisms underlying recurrent BP are the same as BP and, therefore, whether the therapeutic approaches should be different. 12
The objective of this study was to identify predictors of BP recurrence by analyzing the clinical characteristics, associated comorbidities, and outcomes in patients with primary and recurrent BP.
Materials and Methods
This retrospective study included patients diagnosed with BP at Alhada Armed Forces Hospital during 2018 to 2024. This study was approved by the Research Ethics Committee at Alhada Armed Forces Hospital, Taif City, Saudi Arabia (application number: 2024-924). The Department of Otolaryngology—Head and Neck Surgery provided the list of patients. Data were collected by the research team from patients’ files.
Study Population
The study included patients of all age groups and both sexes who were diagnosed with BP. Inclusion criteria were a diagnosis of BP based on clinical otolaryngology and neurological evaluations, initiation of treatment within 3 days of symptom onset with a standardized regimen of prednisone (1 mg/kg) for 10 days, and completion of follow-up with physical therapy and otolaryngology clinic until discharge. Patients with recurrent BP were treated with high-dose corticosteroids (prednisone 1 mg/kg/day for 10 days), and antiviral agents (eg, acyclovir) were added if viral infection was suspected. Patients with recurrent episodes underwent brain computed tomography (CT) and magnetic resonance imaging (MRI) scans to rule out central lesions such as tumors or vascular anomalies. Exclusion criteria were pregnancy; facial palsy resulting from metabolic, neurological, neoplastic, toxic, or iatrogenic causes; traumatic injury to the facial nerve, varicella-zoster virus infection (Ramsay-Hunt syndrome), Melkersson-Rosenthal syndrome, and central lesions that included any abnormal findings on imaging or clinical signs indicative of a central nervous system pathology.
Data Collection
Data on demographics; comorbid conditions such as diabetes, hypertension, and autoimmune diseases; previous viral infections; systemic infections; audio-vestibular symptoms; and family history of facial palsy were collected. Clinical data included palsy’s side and presence, recurrence timing, interval between episodes, and any other associated symptoms. The House-Brackmann facial grading scale, ranging from I (normal function) to VI (complete paralysis), was used to assess the severity of paresis/paralysis owing to its ease of use. Additional data from investigations and follow-ups with ENT specialists and physiotherapists were gathered to evaluate recovery outcomes. The primary outcome was recurrence of BP after the initial episode’s full recovery.
Statistical Analyses
All statistical analyses were performed using SPSS version 23. Continuous variables were evaluated for normality using the Shapiro-Wilk test. In case of non-normality, nonparametric tests such as the Mann-Whitney U test were employed. Categorical variables were analyzed using Pearson’s chi-squared test. Logistic regression analysis was performed to identify independent predictors of BP recurrence. The dependent variable in the logistic regression model was BP recurrence, while the independent variables included age, sex, comorbidities, and severity of the initial presentation. Statistical significance was set at P < .05.
Results
A total of 254 patients were included in the study. Table 1 presents patients’ sociodemographics and medical history, highlighting a predominance of women (53.1% vs 46.9%). Most patients were aged 51 to 65 years (29.5%), followed by those aged 36 to 50 years (20.9%) and >65 years (16.9%). Regarding body mass index, 52.0% were obese; 22.8%, overweight; 19.7%, normal weight; and 5.5%, underweight. Diabetes mellitus was the most prevalent comorbidity (39.0%), followed by hypertension (32.7%), hypothyroidism (16.1%), other conditions (9.8%), autoimmune disorders (9.4%), and smoking and cerebrovascular accidents (3.1% each). Additionally, 28.3% of patients reported a family history of BP.
Sociodemographics and Medical History of Patients With BP.
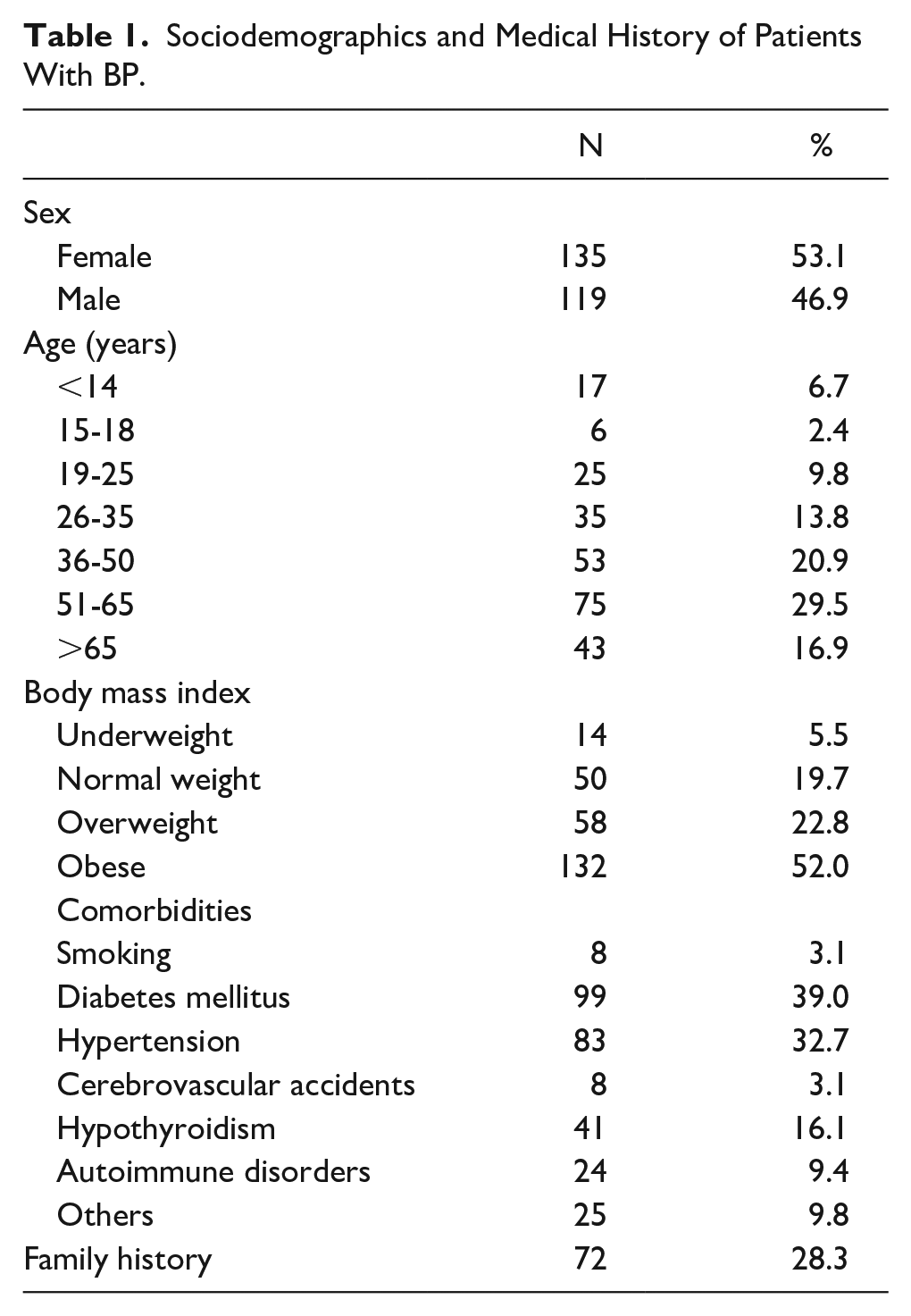
Table 2 presents BP–related characteristics. Most patients did not experience BP recurrence (79.1%), whereas 20.9% did. Most patients did not have viral infections (88.2%), whereas 11.8% had. The severity of BP was graded as follows: grade 1, 7.5%; grade 2, 30.3%; grade 3, 24.0%; grade 4, 24.8%; grade 5, 11.4%; and grade 6, 2.0%. The side of BP was almost evenly split between the right (49.6%) and left (50.4%) sides. Regarding additional symptoms, 19.7% experienced vertigo; 21.7%, tinnitus, and 6.7%, decreased hearing. Recovery from the current episode of BP was complete in 66.9% of cases, partial in 24.8%, and not achieved in 8.3%. For those with recurrent episodes (n = 53), all patients reported complete recovery, with a duration of recovery spanning 1 to 3 months for 35.8%, 4 to 6 months for 26.4%, 7 to 9 months for 30.2%, and 10 to 12 months, and >12 months for 3.8%. Regarding the side of recurrence, 35.8% experienced recurrence on the same side, while 64.2% had new onset on the opposite side. Among the 53 patients with recurrent BP, 97% experienced 1 recurrence, while 3% had 2 or more episodes. The median time to recurrence was 12 months (range: 6-24 months), and the median follow-up time for all patients was 12 months.
BP-Related Characteristics.
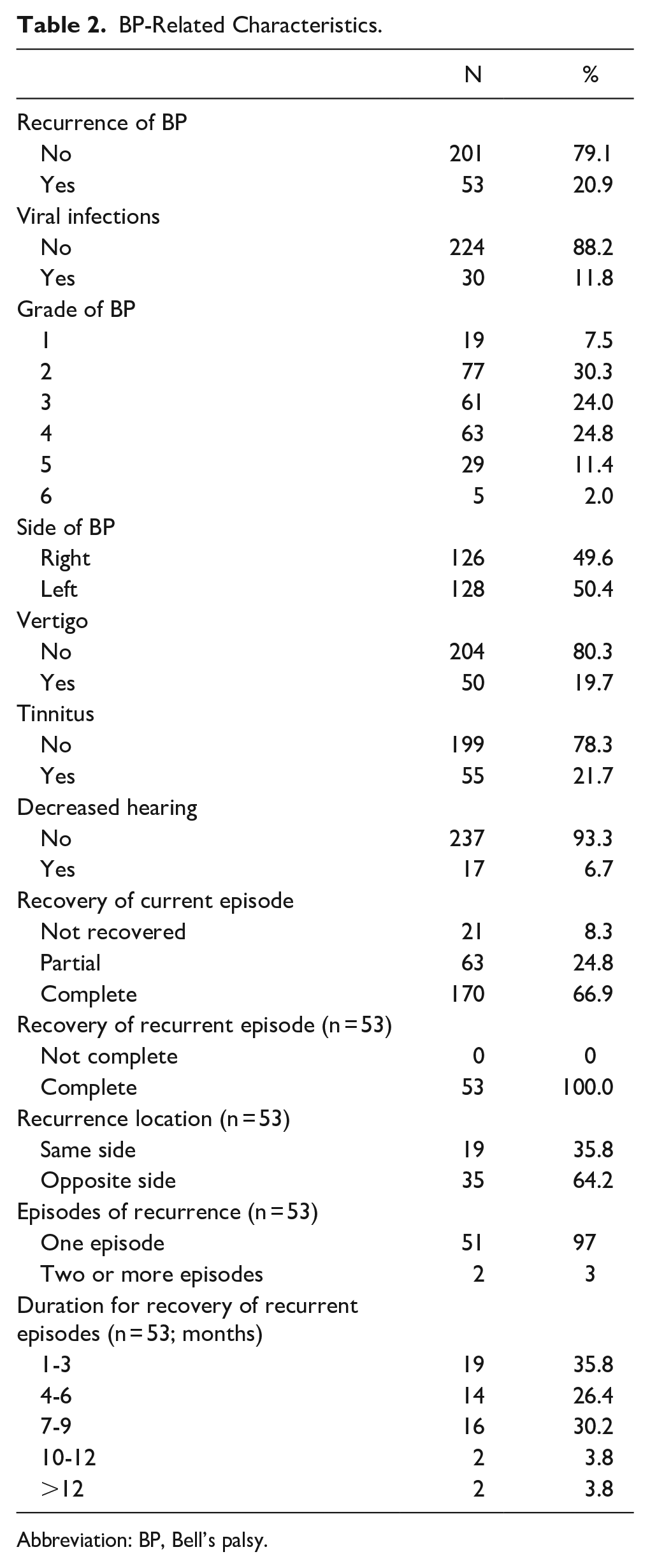
Abbreviation: BP, Bell’s palsy.
Table 3 presents the prevalence of BP recurrence based on various sociodemographic, medical, and clinical characteristics. Recurrence was significantly more common among women than among men (26.7% vs 14.3%; P = .015). Age did not significantly affect the recurrence rate (P = .835). Patients with obesity had a high recurrence rate (23.5%); however, the difference was not significant (P = .577). Smoking status did not lead to a significant difference in the recurrence rate (P = .140). Diabetes (33.3%, P < .001), hypertension (41.0%, P < .001), hypothyroidism (56.1%, P < .001), and autoimmune disorders (54.2%, P < .001) were significantly associated with high recurrence rates. Patients with a family history of BP had a significantly-high recurrence rate (48.6%, P < .001). The grade of BP significantly influenced recurrence, with higher grades showing increased recurrence (P < .001). The side of BP and cardiovascular diseases did not significantly affect recurrence (P > .05). Vertigo (40.0%, P < .001) and decreased hearing (70.6%, P < .001) were significantly associated with high recurrence rates. Tinnitus resulted in a high recurrence rate (29.1%), but no significant difference was observed (P = .090). Recovery from the current episode was significantly associated with recurrence, with non-recovered patients having the highest recurrence rate (52.4%, P < .001).
Prevalence of Recurrence of BP Based on Sociodemographic, Medical, and Clinical Characteristics.
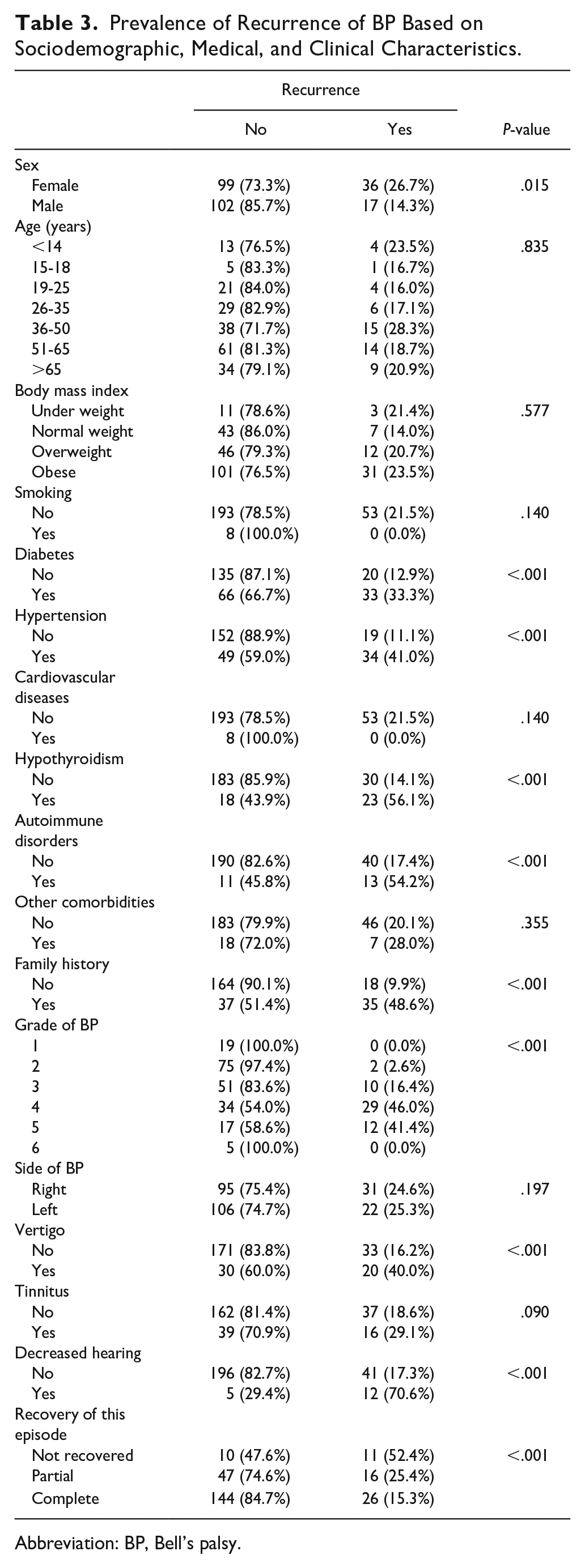
Abbreviation: BP, Bell’s palsy.
Table 4 presents the multiple logistic regression analysis of the risk factors for BP recurrence. Individuals aged 26 to 35 years [odds ratio (OR) = 18.07 (4.88-47.09) P = .001] and 36 to 50 years [OR = 35.91 (2.21-584.95), P = .012] were significantly more likely to experience recurrence than those aged >65 years. Diabetes mellitus [OR = 27.66 (2.26 to 338.49), P = .009], hypertension [OR = 40.08 (4.16-386.50), P = 0.001], hypothyroidism (OR = 13.65 [1.49-124.92] P = 0.021), autoimmune disease [OR = 22.46 (1.03-491.67), P = 0.048], and a family history of BP [OR = 134.35 (14.40-1253.50), P < 0.001] were significantly associated with an increased recurrence risk.
Multiple Logistic Regression Analysis of Risk of Recurrence of BP.
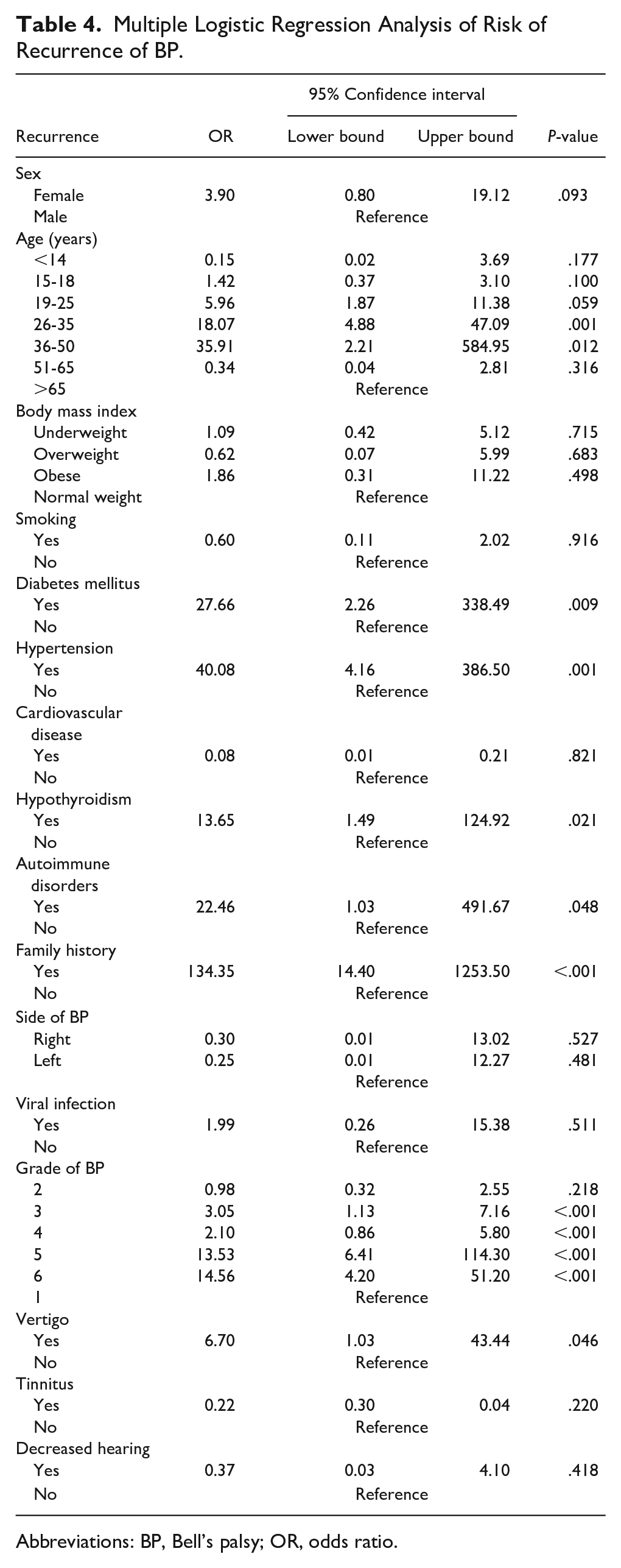
Abbreviations: BP, Bell’s palsy; OR, odds ratio.
Regarding the grade of BP, grade 3 [OR = 3.05 (1.13-7.16), P < .001], grade 4 [OR = 2.10 (0.86-5.80), P < .001], grade 5 [OR = 13.53 (6.41-114.30), P < .001], and grade 6 [OR = 14.56 (4.20-51.20), P ≤ .001] were significantly associated with an increased recurrence risk compared with grades 1 and 2. Vertigo also significantly increased the risk of BP [OR = 6.70 (1.03-43.44), P = .046]. Tinnitus, decreased hearing, sex, obesity, smoking, and body mass index did not significantly affect the risk of recurrence.
Discussion
The recurrence rate of BP in our study was notably higher (20.9%) than the general estimate of 4% to 7%. This may be attributed to the specific characteristics of our cohort, which included a significant proportion of patients with comorbidities such as diabetes (33.3%), hypertension (41.0%), and hypothyroidism (56.1%). These comorbidities are known to be significantly associated with higher recurrence rates (P < .001). Additionally, this aligns with the findings of Ralli et al., 12 who observed a poor prognosis for recurrent ipsilateral attacks but a good recovery for bilateral alternating palsies. 1 In contrast, Pitts et al. reported no adverse impact on recovery regardless of the site of recurrence. 11 Approximately 16% of untreated BP cases have resulted in permanent moderate-to-severe weakness. 3 Although this statistic does not directly correlate with recurrence, it highlights that a significant proportion of patients experience long-term effects potentially linked to an increased likelihood of recurrence. The study findings showed that most cases of BP (grades 1-3) were not very severe, indicating a positive trend, with most cases being mild to moderate. The presence of viral infections in 11.8% of our patients aligns with the long-suspected link between viral infections and BP. While the exact mechanism remains unclear, studies suggest that reactivation of latent herpes viruses, particularly the herpes simplex virus, plays a role in triggering an inflammatory response within the facial nerve, leading to palsy.12-14
The distribution of BP severity in our study revealed a diverse range of presentations. Notably, grade 2 (30.3%) and grade 4 (24.8%) were the most common, indicating that a considerable proportion of patients experienced moderate-to-severe facial weakness. This finding contrasts with our previous observation that >60% of cases presented with mild-to-moderate severity (grades 1-3). This discrepancy may stem from variations in classification systems used or reflect the inclusion of recurrent cases in the current analysis, which could potentially skew the severity distribution toward severe presentations.15,16 Consistent with the established understanding of BP, our study showed a near-even split between the right- (49.6%) and left-side (50.4%) involvement, confirming the lack of side predilection.
The significant association between female sex and increased recurrence (26.7% vs 14.3%, P = .015) aligns with the findings of Cirpaciu and Goanta, who observed a higher prevalence of recurrent idiopathic facial palsy in female patients than in male patients. Although age alone did not significantly affect recurrence, the presence of comorbidities affected recurrence. The strong association of diabetes (33.3%, P < .001), hypertension (41.0%, P < .001), hypothyroidism (56.1%, P < .001), and autoimmune disorders (54.2%, P < .001) with high recurrence rates underscores the potential role of underlying health conditions in influencing BP recurrence. Therefore, it is important to consider potential confounding variables. For instance, the presence of multiple comorbidities in a single patient could exacerbate the likelihood of recurrence, and the interrelationship between these conditions could complicate the analysis.17,18 Additional reported symptoms, such as vertigo (19.7%) and tinnitus (21.7%), were consistent with an increase in the recurrence of BP.
Overall, 66.9% of the patients achieved complete recovery from the current episode. This aligns with the findings of McCaul et al., who reported that approximately 71% of untreated BP cases resolved completely. 19 However, 8.3% of the patients did not recover and required medical attention. The fact that all patients with recurrence reported complete recovery is promising. However, the extended recovery duration for some patients, with 30.2% requiring 7 to 9 months and a small percentage exceeding 10 months, highlights the potential long-term effects of recurrence.
The findings from our study revealed significant independent associations between various factors and the recurrence of BP using the multiple regression analysis. Individuals aged 26 to 35 and 36 to 50 years exhibited a markedly-higher likelihood of recurrence than individuals aged >65 years. This suggests that younger adults are more susceptible to recurrent episodes than older adults, which might be because of the different immune response dynamics or hormonal factors in these age groups. Cirpaciu and Goanta found that recurrence was frequent among younger individuals, with the first episode often occurring during childhood. 9 Similarly, Holland reported a peak incidence of BP during 15 to 40 years. 5 The immune system undergoes significant maturation and is modulated with age. Younger adults may experience a robust inflammatory response to triggers, such as viral reactivation, potentially increasing the likelihood of nerve damage and recurrence. 8 Hormonal fluctuations, particularly in women of reproductive age, may play a role. 20 Some studies have suggested an association between BP and pregnancy or hormonal changes.21,22 Although our study did not specifically analyze genetic factors within age groups, it is plausible that genetic predispositions to BP are more prevalent or have stronger effects in younger individuals than in older individuals. 23
In the context of BP, it is important to consider other diseases that may present with facial nerve paralysis to ensure accurate diagnosis and treatment. Several conditions can mimic BP and must be excluded before diagnosing the patient to have a BP including Lyme disease, Ramsay-Hunt syndrome, sarcoidosis, Guillain-Barré syndrome, and stroke. These conditions must be carefully differentiated from BP through clinical evaluation and appropriate testing. Lyme disease, caused by Borrelia burgdorferi, may present with facial palsy, especially in endemic areas, and requires serological testing for diagnosis. Ramsay-Hunt syndrome, due to the reactivation of varicella-zoster, involves facial paralysis with ear vesicles, and antiviral therapy with corticosteroids is important for treatment. Guillain-Barré syndrome can cause bilateral facial paralysis and limb weakness, distinguished by nerve conduction studies and cerebrospinal fluid analysis. Sarcoidosis may present with facial paralysis and systemic signs such as pulmonary involvement, and it requires imaging and biopsy for confirmation. Finally, a stroke may present with upper facial palsy and mimic BP but typically involves additional neurological deficits, making brain imaging (CT/MRI) crucial to rule out.24-28
Limitations
This study is limited by its retrospective design, which may introduce selection bias and recall bias. Moreover, the absence of a prospective control group limits the ability to draw causal conclusions. Further, the relatively-high recurrence rate in our cohort may reflect the tertiary care setting, which tends to see more severe or recurrent cases. Further studies are needed to provide valuable insights, and a large sample size would strengthen the statistical power and generalizability of the findings to a broader population.
Conclusion
This study provides important insights into the recurrence and prognosis of BP. Notably, the recurrence rate in our patient population was higher than that reported previously. Our findings corroborate previous research that links recurrence with systemic comorbidities, such as diabetes, hypertension, hypothyroidism, and autoimmune disorders, suggesting that these conditions significantly influence the likelihood of BP recurrence. Demographic analysis showed a high prevalence of BP in female patients and middle-aged adults, indicating potential sex- and age-related vulnerabilities.
Footnotes
Author Contributions
All authors contributed equally to the planning, literature survey, data collection, analysis, and manuscript writing.
Data Availability
Data supporting the conclusions in this study are available from the corresponding author on a reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
The study was approved by the Research Ethics Committee of Alhada Armed Forces Hospital, Taif City, Saudi Arabia (application number: 2024-924).
Consent to Participate
Not applicable.