
Abstract
Objective
The aim of this study was to report the incidence and clinical course of a series of patients who were misdiagnosed with Bell's palsy and were eventually proven to have occult neoplasms.
Methods
Two hundred forty patients with unilateral facial paralysis who were assessed at the facial nerve reanimation clinic, Victoria Hospital, London Health Science Centre, from 2008 through 2017 were reviewed. Persistent paralysis without recovery was the presenting complaint.
Results
Nine patients (3.8%) who were proven to have occult neoplasms initially presented with a diagnosis of Bell's palsy. The mean diagnostic delay was 43.5 months. Four patients were proven to have skin cancers, 3 patients had parotid cancers, and 2 patients had facial nerve schwannomas as a final diagnosis. Initial magnetic resonance imaging (MRI) was performed in all 9 patients and 8 underwent a follow-up MRI. An occult tumor was identified upon review of the original MRI in one patient and at follow-up MRI in 8 patients. The mean time interval between the initial and follow-up imaging was 30.8 months. The disease status at most recent follow-up were no evidence of disease in 2 patients (22%) and alive with disease in 7 patients (78%). An irreversible, progressive pattern of facial paralysis combined with pain, multiple cranial neuropathies or history of skin cancer were predictable risk factors for occult tumors. Seven out of the 9 patients (77.8%) underwent at least one type of facial reanimation surgery, and the final subjective results by the surgeon were available for 5 patients. Three out of the 5 (60%) patients who were available for final subjective analysis were reported as Grade III according to the modified House-Brackmann scale.
Conclusion
Occult facial nerve neoplasm should be suspected in patients with progressive and irreversible facial paralysis but the diagnosis may only become evident with follow-up imaging. Facial reanimation surgery is a satisfactory option for these patients.
Graphical Abstract

Introduction
Approximately 20% of facial paralysis can be demonstrated to have specific causes, such as infections, inflammatory processes, or neoplasms and facial paralysis can be the first sign of a serious underlying disorder. Eighty percent of all peripheral facial nerve paralysis is initially labeled as idiopathic nerve paralysis, also known as Bell's palsy. Recovery is usually prompt and complete in 70% of these cases [1]. Neoplasms of the facial nerve is uncommon. It accounts for approximately 5% of all cases [2]. However, there has been no detailed report on the etiology of diagnostic delay, imaging analysis, long-term prognosis and functional results of facial reanimation for these patients. The purpose of this article was to analyze the incidence and clinical course of a series of patients who were misdiagnosed as having Bell's palsy and were eventually proven to have an occult neoplasm in a single facial nerve reanimation clinic.
Materials and methods
Patient demographics
The records of 240 patients with unilateral facial paralysis who were seen at the facial nerve reanimation clinic, Victoria Hospital, London Health Science Centre, from 2008 through 2017 were retrospectively reviewed in the study. The study group was composed of 121 men and 119 women (mean age: 57.3 years; range: 9–95 years).
Prolonged pattern of paralysis without recovery was the main complaint at our facial nerve reanimation clinic. Sixty-three of the 240 patients (26%) were diagnosed as having Bell's palsy. One hundred of the 240 patients (42%) were diagnosed with facial paralysis associated with tumor (parotid gland in 19 patients, acoustic neuroma in 27 patients, facial nerve schwannoma in 9 patients, skin cancers in 23 patients and other head and neck or skull base tumors in 22 patients). Thirty-eight of the 240 patients were associated with trauma (16%; iatrogenic in 15 and accident or stab wound in 23 patients) and 24 patients (10%) were diagnosed with facial paralysis associated with infection (Ramsay-Hunt syndrome in 19 patients and other infections in 5 patients). Fifteen patients (6%) were identified as having facial paralysis in association with recognizable congenital anomalies. Nine of the 63 patients (14.3%) who were referred with a clinical and MRI diagnosis of Bell's palsy were proven to have occult neoplasms.
Diagnostic imaging and outcome analysis
Two experienced head and neck neuroradiologists (R.K. and KY.T.) analyzed all MRIs. The treatment modality of occult neoplasm was determined on the basis of multidisciplinary team approaches, considering several factors, including size and site of the tumor, possibility of curative resection, general performance status of the patient, and preference of each patient. The tumor responses were evaluated using the RECIST 1.1 criteria [3].
Statistical analysis
The groups were compared using the chi-square to identify differences in presenting symptoms when comparing those with true Bell's to to those with an occult malignancy. Multivariate analysis was performed by logistic regression using IBM SPSS Statistics version 23.0 (IBM Corp., Armonk, NY, USA). A P value of less than 0.05 was considered significant.
Results
Patient demographics
The clinical findings, pathologic features and treatment outcomes of the occult neoplasm of facial nerve
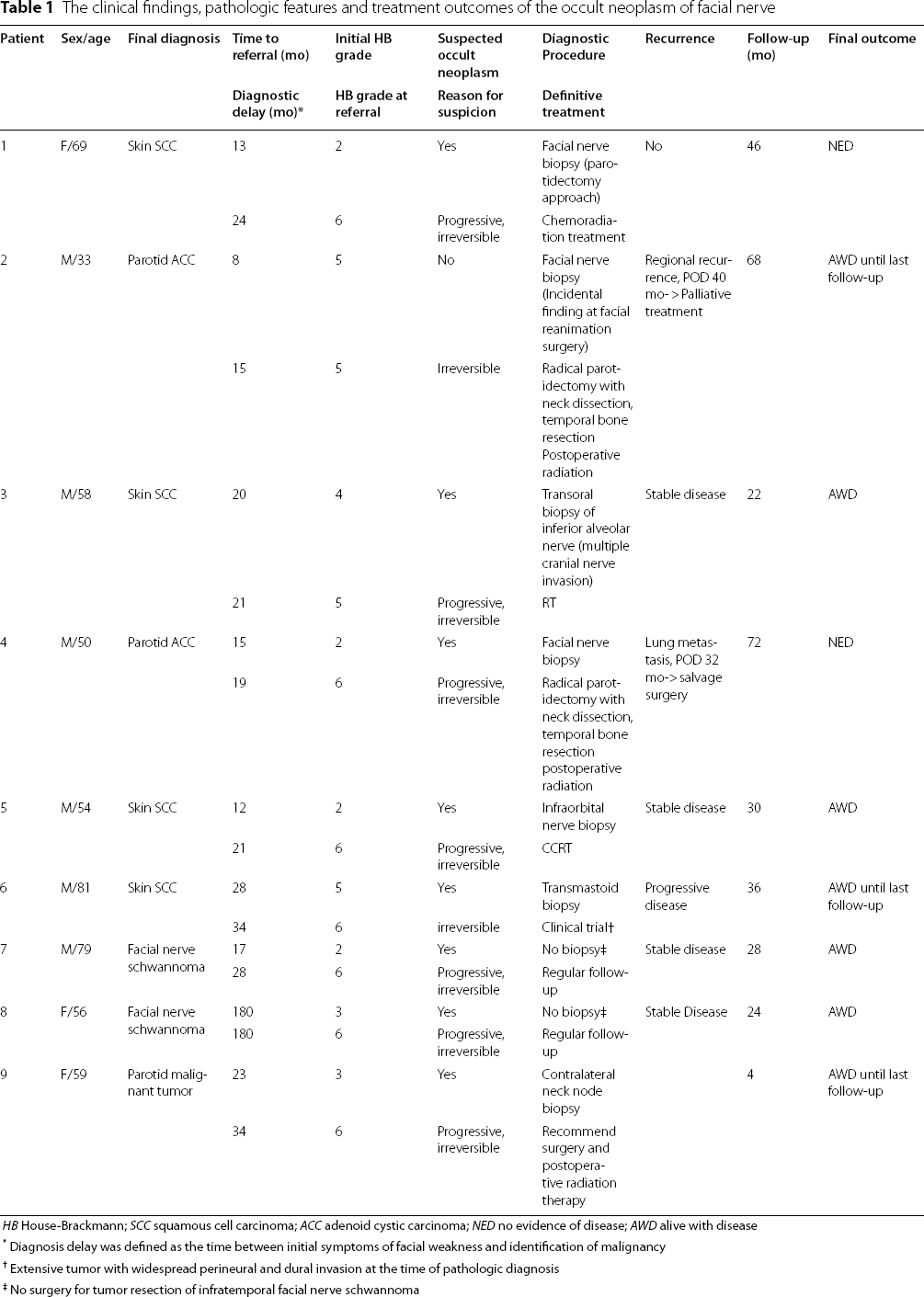
HB House-Brackmann; SCC squamous cell carcinoma; ACC adenoid cystic carcinoma; NED no evidence of disease; AWD alive with disease
*Diagnosis delay was defined as the time between initial symptoms of facial weakness and identification of malignancy
†Extensive tumor with widespread perineural and dural invasion at the time of pathologic diagnosis
‡No surgery for tumor resection of infratemporal facial nerve schwannoma
Occult neoplasm was suspected as the etiology of facial paralysis based on clinical pattern, in 8 patients at the first visit at our clinic, although they were transferred with the initial diagnosis of Bell's palsy. Facial nerve (n = 4, 44.4%), infraorbital nerve (n = 1, 11.1%), and inferior alveolar nerve (n = 1, 11.1%) biopsies were undertaken as diagnostic procedures. Metastatic parotid malignant tumor was identified with a fine needle aspiration biopsy in one patient. All patients with facial nerve schwannomas were diagnosed with follow-up imaging without facial nerve exploration.
Diagnostic imaging and outcome analysis
Results of the imaging study of occult neoplasm patients

No number; FN facial nerve; SCC squamous cell carcinoma; ACC adenoid cystic carcinoma
*The occult tumor was identified at exploration surgery without follow-up MR
†Although the formal radiologic reports of the initial MR image from the radiologist at the outside hospital were compatible with Bell's palsy, our neuroradiologist re-evaluated the initial MR image and found a small suspicious lesion in the parotid deep lobe
Initial MR imaging was normal in one out of 9 patients (11.1%, patient 3). Abnormal asymmetric enhancement in the mastoid segment of the facial nerve developed at the follow-up MR image at 6 months, and the lesion was identified along the V3 branch of the trigeminal nerve in this patient (Fig. 1). The result of transoral biopsy of the inferior alveolar nerve was squamous cell carcinoma. The patient was in a state of stable disease (SD) after definitive radiotherapy (RT) at 22 months following treatment.
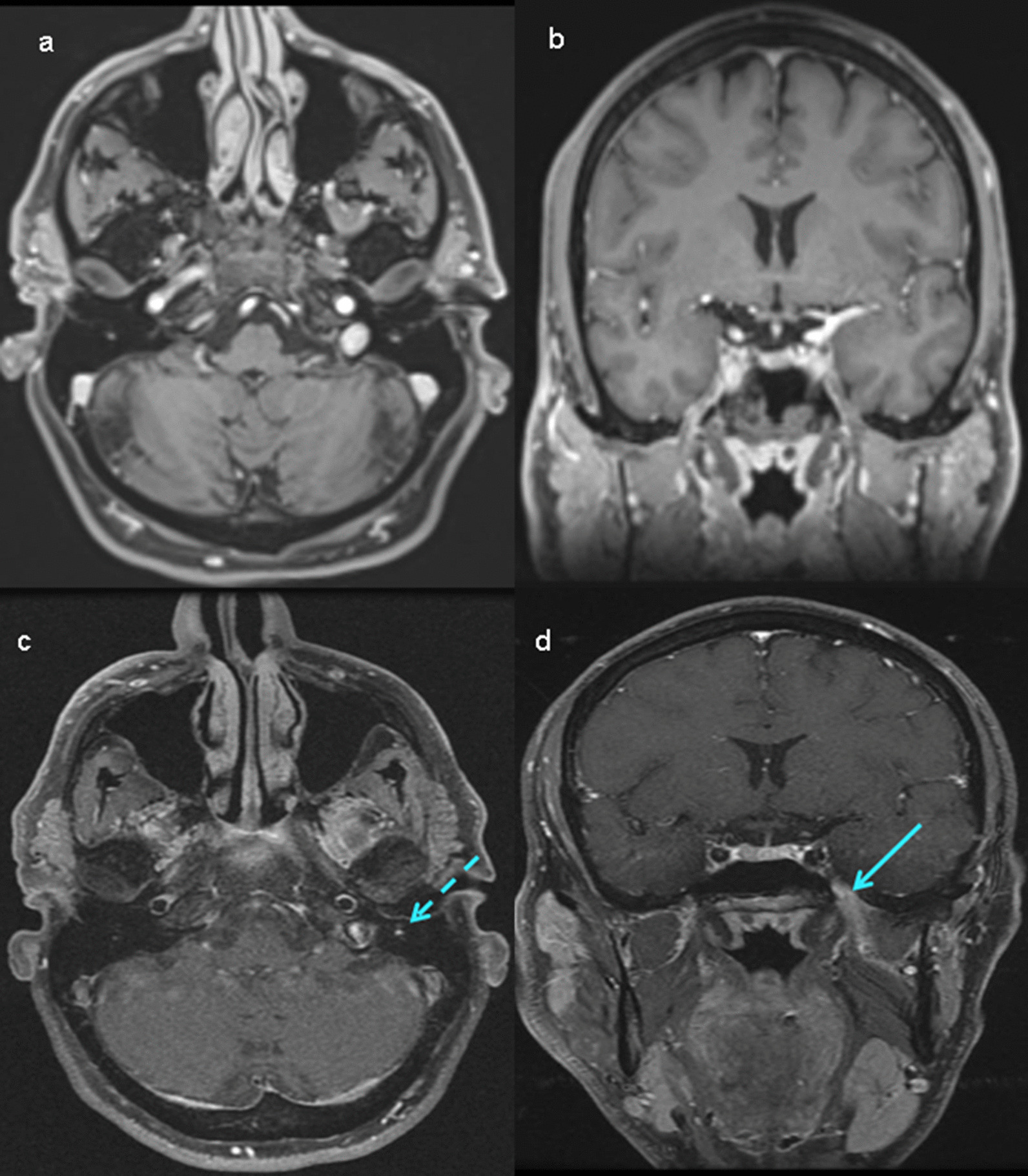
Comparison between initial and follow-T1 Post-gadolinium MR imaging in patient 3
Nonspecific enhancement of the facial nerve was reported in 2 patients (22.2%) at the initial MR. The extent of asymmetric enhancement was increased in these two patients at the follow-up MRI (Figs. 2 and 3). The final pathologic diagnoses were squamous cell carcinoma of the skin (patient 1) and adenoid cystic carcinoma of parotid gland (patient 4). Primary chemoradiation treatment was recommended and complete response (CR) was seen in patient 1. Patient 4 underwent radical surgery and postoperative radiation treatment. The patient developed lung metastasis, and subsequently underwent salvage surgery for isolated lung metastasis with video-assisted thoracoscopic surgery. Patients 1 and 4 were alive without significant morbidity at the time of this report.

Comparison between initial and follow-up axial T1 Post-gadolinium MR imaging in patient 1

Comparison between initial and follow-up axial T1 Post- gadolinium MR imaging in patient 4
In 3 patients (patient 3, 4 and 9), the initial MRI conducted at an outside hospital prior to referral were re-evaluated by our neuroradiologists following their initial clinic visit. In one case, a small suspicious lesion in the parotid deep lobe was found (patient 9). This patient was lost to follow-up. In 5 cases, only the dictated MRI reports (consistent with Bell's palsy) from the outside hospital without images were available (patient 2, 5, 6, 7 and 8) and repeat imaging was performed at our institution. The final diagnosis of these patients were facial nerve schwannoma in 2 patients (patients 7 and 8), skin squamous cell carcinoma in 2 patients (patient 5 and 6) and parotid adenoid cystic carcinoma in 1 patient (patient 2). All patients with facial nerve schwannoma refused surgical resection of infratemporal tumor. Of the two patients with skin cancer, one patient (patient 5) underwent definitive chemoradiotherapy (CRT) and stable disease (SD) was achieved. A clinical trial was recommended for the other patient with skin cancer because of extensive perineural and dural invasion (patient 6). Radical surgery and postoperative radiation treatment was performed for the other parotid cancer patient who underwent surgical exploration without follow-up MR (patient No. 2). This patient developed regional recurrence that was not considered for salvage treatment because of the extensive perineural extension.
The final outcomes of the occult tumor patients (n = 9) were no evidence of disease in 2 patients (22%) and alive with disease in 7 patients (78%) during a mean follow-up of 36.7 months (range 4–72 months).
Risk factor analysis of occult neoplasm
The risk factor analysis of occult neoplasm
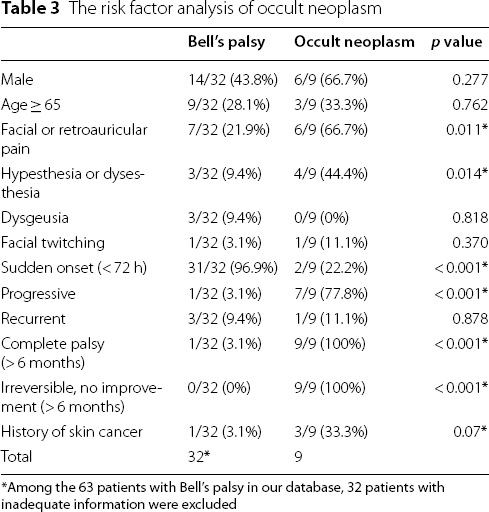
*Among the 63 patients with Bell's palsy in our database, 32 patients with inadequate information were excluded
Facial reanimation surgery
Seven out of 9 the patients (77.8%) underwent at least one type of facial reanimation surgery. Three patients underwent facial reanimation as a concurrent operation with ablation surgery, and 4 patients had a staged operation. The mean number of reanimation surgeries was 1.6 (range 0–3). Surgery for the upper face included upper eyelid gold weight (n = 6, 85.7%) and lower lid tendon suspension (n = 3, 42.8%) and nerve interposition cable graft (n = 1, 14.3%). Static suspension to midface and mouth (n = 4, 57.1%), dynamic suspension (n = 2, 28.6%). and gracilis free flap (n = 2, 28.6%) were used for the lower face reanimations.
Facial reanimation surgery

*Surgery was performed at another hospital

Final outcome after facial reanimation surgery in patient 4. Gold weight implant, lower lid tendon suspension, and gracilis
Discussion
Many etiological factors can cause unilateral facial palsy but Bell's palsy, is the most common diagnosis. In the report of 1989 patients presenting to a tertiary facial nerve center, Bell's palsy accounted for 38%, acoustic neuroma resections 10%, cancer 7%, iatrogenic injuries 7%, varicella zoster 7%, benign lesions 5%, congenital palsy 5%, Lyme disease 4%, and other causes 17%. [6] There has been no report on the analysis of etiologies from a facial nerve reanimation clinic that mainly offers interventions to help restore a more normal appearance. The prolonged pattern of paralysis without recovery was the main complaint at our facial nerve reanimation clinic. Forty-two percent of the patients were diagnosed with facial paralysis associated with tumors, 26% with Bell's palsy, 16% with trauma, 10% with infection and 6% with congenital anomalies. There was a significantly higher rate of tumors compared to results of previous reports [6].
Bell's palsy is the most common cause of facial nerve paralysis or weakness and is typically self-limited. Bell's palsy may be associated with mild pain, numbness, increased sensitivity to sound, and alterations in taste. Onset is usually rapid (< 72 h), with spontaneous recovery occurring within 2 to 8 weeks in more than 80% of patients. Although Bell palsy has a classic presentation readily identified with a thorough history and physical exam, it remains a diagnosis of exclusion after other potential causes are ruled out [7].
Facial paralysis of neoplastic origin is estimated to represent the etiology in approximately 5% of all cases [2]. Neoplastic origin may be neurogenic primary lesions of the seventh cranial nerve or secondary, extrinsic neoplasms [2]. We analyzed 9 patients with unilateral facial paralysis, all of whom had an initial diagnosis of Bell's palsy and were ultimately diagnosed with occult neoplasms. The formal radiologic report of the initial MRI of the patients reported no evidence of tumorous lesions. We doubted the diagnoses of Bell's palsy based on the unusual histories that were inconsistent with Bell's palsy with respect to the progressive and irreversible unilateral facial paralysis in all patients. Persistent facial paralysis with no return of any function beyond 6 months is usually not idiopathic [8].
The diagnosis of Bell palsy based on the MRI findings in some situations may lead to a false sense of security for patients with unilateral facial paralysis. Despite the dramatic advances in technologies of the various diagnostic modalities, Jackson et al. wrote that there remain limitations of resolution, and false-negative results are not uncommon [9]. Surgical exploration of the facial nerve may serves as a diagnostic and therapeutic approach in selected circumstances [9]. Surgical exploration of the parotid gland and facial nerve should be considered in patients with facial nerve paralysis who show no signs of regeneration 6 months after the onset of paralysis and/or persistent electrophysiological signs of ongoing neuronal degeneration, even if imaging tests, such as MRI studies, show no evidence of tumor [2].
If the facial nerve paralysis progresses slowly to complete paralysis and persists without any sign of recovery, it strongly suggests a neoplastic lesion involving the facial nerve. A slow progression of facial paralysis is the clinical characteristic of the neoplastic disorder, in contrast with the typical brief and self-limited course of Bell palsy. Nevertheless, a sudden onset of facial paralysis does not always exclude tumor involvement of the facial nerve. Progressing unilateral facial paralysis beyond 3 weeks and no evidence of recovery after 6 months of paralysis strongly suggest neoplastic involvement in the facial nerve [1].
Pain was also the main associated complaint in our cohort (6 out of the 9 patients; 66.7%). Although facial pain is not unusual in patients with Ramsey-Hunt syndrome or Bell's palsy, its presence must be investigated. Jackson and Glasscock [9] reported that pain was identified in 18% of their patients with facial nerve neoplasm. Persistent pain beyond several months after onset of facial paralysis should warrant further investigation for an occult neoplasm [8].
A cranial neuropathy other than the facial nerve is sometimes seen in patients with Bell palsy. However, a high level of suspicion is necessary when there are persistent sensory and motor deficits beyond the facial nerve [8] .
Previous treatment history of regional skin cancer is also known to be a strong causal factor for facial nerve paralysis, especially in patients with pain involving other nerves [8]. In our series, 3 of the 9 patients had a history of a regional skin squamous cell carcinoma.
In our cohort, the possible reasons for diagnostic delay were no abnormal findings on the initial image, nonspecific facial nerve enhancement on initial MR, or non-enhancement with gadolinium. Therefore, follow-up imaging with adequate coverage of the entire facial nerve and neuroradiology consultation appears to be an essential component to mitigate diagnostic delay. In our, patient 2 did not receive repeat imaging prior to surgery as no occult neoplasm was suspected. This patient was a 33-year-old-male with a typical history of right Bell's palsy. Quality and severity did not change over 8 months. At that time, there were only MRI report from other center (without consultation from neuroradiologist) and the report of MRI did not show any etiology. Four months later, he underwent reconstructive surgery after extensive consultation. The facial nerve was identified through a retrograde approach, and we found completely abnormal and infiltrative tumor invading the facial nerve. It was small but very hard mass arising from deep to the facial nerve extending into the parapharyngeal space. The final diagnosis was high-grade adenoid cystic carcinoma measuring at least 2 cm in size, with perineural infiltration and microscopically positive margin. After surgery, he received adjuvant radiation treatment. This would be an example of the occult neoplasm identified by consulting a neuroradiologist or repeating MRI images.
None of the nine patients would have been confirmed to have a neoplasm without rigorous and long-term follow up. Therefore, careful and deliberate follow-up incorporating appropriate imaging evaluated by expert radiologists is essential when confronted with atypical presentations of facial paralysis.
The approach to re-animation is especially challenging for these patients because of the diagnostic dilemma coupled with limited options due to their late presentations. In our study, seven out of the 9 patients (77.8%) underwent at least one type of facial reanimation surgery. Three out of the five (60%) patients were graded as HB III with satisfactory symmetry, mouth angle excursion and eye protection. Even in patients with occult neoplasms and those alive with disease, facial reanimation surgery an improve quality of life in selected patients.
The limitations of this study were that because of the low number of patients with occult neoplasms making strong recommendations should be done with caution. The source of initial HB grade may not be accurate because of the retrospective nature of this study.
Conclusion
Occult facial nerve neoplasm should be suspected in patients with progressive and irreversible facial paralysis. Repeat MRI and surgical exploration may be required to make the diagnosis. Facial reanimation surgery should be offered for these patients.
Footnotes
Acknowledgements
Not applicable
Author contributions
EC: Collected the data/Contributed data or analysis tools/Performed the analysis/Wrote the paper. DM: Conceived and designed the analysis/Collected the data. KF: Collected the data/Contributed data or analysis tools. DM: Contributed data or analysis tools. AN: Contributed data or analysis tools. RK: Collected the data/Contributed data or analysis tools/Performed the analysis. KY: Contributed data or analysis tools/Performed the analysis. JY: Conceived and designed the analysis/Collected the data/Contributed data or analysis tools/Performed the analysis. All authors read and approved the final manuscript.
Funding
Not applicable.
Availability of data and materials
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Declarations
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.