
Abstract
Introduction
Magnesium is an essential mineral that is required for many biochemical reactions in the metabolism of the human body, and it is of great importance because it is a cofactor of over 600 enzyme reactions and an activator of 200 enzymes. 1 Magnesium helps improve the maintenance of normal bones and teeth and the normal functioning of the neuromuscular, cardiovascular, and metabolic systems.1,2 In addition, it has important roles in electrolyte balance, energy production, protein and DNA synthesis, and psychological function. 1 Therefore, magnesium deficiency can be involved in many diseases clinically. In fact, many negative conditions have been reported to be associated with magnesium deficiency such as hypocalcemia, hypopotassemia, osteoporotic bones, cardiovascular and neurological disorders, hyperglycemia, cancer, and Covid-19.1,2 More specifically, magnesium deficiency is associated with diabetes mellitus, 3 preeclampsia, 4 migraine, 5 inflammation, 6 and oxidative stress. 7
Idiopathic facial nerve paresis is called Bell’s palsy and represents approximately 60% to 75% of cases with facial nerve palsy. 8 The most recent findings show that Bell’s palsy has a peripheral neuropathic nature of the facial nerve. 9 The situations associated with magnesium deficiency mentioned above (hyperglycemia, preeclampsia, migraine, inflammation, and oxidative stress)3-7 have been reported as risk factors related to Bell’s palsy.10-13 The diagnosis of Bell’s palsy is based on exclusions, and differential diagnosis is very important.8,11 Corticosteroids have strong evidence for the treatment of Bell’s palsy 8 ; however, its etiopathogenesis remains unclear during disease management. 11
As stated above, both magnesium deficiency3-7 and Bell’s palsy10-13 are associated with hyperglycemia, preeclampsia, migraine, inflammation, and oxidative stress. Furthermore, Bell’s palsy is accepted as peripheral neuropathy of the facial nerve, 9 and moreover the connection between magnesium deficiency and peripheral neuropathy has previously been reported.14,15 This common feature presents a logical basis to consider magnesium as peripheral neuropathy-related factor in Bell’s palsy. Especially, magnesium deficiency has been reported to be a strong factor related to diabetic peripheral neuropathy. 15 This relationship may also be applicable for facial nerve neuritis. Because magnesium ions can act as a neuroprotective effect by preventing N-methyl-D-aspartic acid (NMDA)-induced nerve damage, support peripheral nerve regeneration by inhibiting inflammatory response and apoptosis, maintain neuronal live and function by participating in the structure of protective molecules, and also promote axonal repair by proliferating Schwann cells. Therefore, magnesium has a paramount role in maintaining the health of the peripheral nerves.
However, to date studies of magnesium status have not been investigated in cases of Bell’s palsy. Therefore, considering the similarities and common features mentioned between Bell’s palsy and magnesium deficiency and the vital effects of magnesium ions on peripheral nerves, we hypothesized that patients with Bell’s palsy may have lower serum magnesium levels compared to healthy individuals. To our knowledge, no studies have addressed magnesium status in cases with Bell’s palsy. In the present study, a comparison was made between Bell’s palsy cases and healthy individuals in terms of serum magnesium concentrations.
Materials and Methods
This study was planned and conducted as a prospective case-control comparison. Ethics approval was received retrospectively (date: November 17, 2023; no. 2023/12-02), and the study was conducted following the ethical standards of the Declaration of Helsinki. The study was carried out at Van Yuzuncu Yil University Hospital between February 2016 and January 2017, and in this study, a total of 24 Bell’s palsy patients and 24 age, gender, and body mass index (BMI; kg/m2) matched healthy controls were included. Healthy controls were relatives and companions of patients from the same geographical regions. Written informed consent was obtained from all participants before any procedure was initiated. After fasting for 12 hours overnight and in the morning, blood samples were taken. Whether the samples belonged to patients or controls was kept secret from laboratory staff. Thus, the laboratory examination was performed blind.
Diagnosis and Exclusion Criteria
The acute paralysis of the peripheral facial nerve of the onset was defined as Bell’s palsy after exclusions and differential diagnosis were performed. Accordingly, medical conditions such as middle ear disease, cranio-otologic injury, neurological disorders, head and neck cancers, autoimmune dysfunction, diabetic neuropathy, and viral infections were excluded and Bell’s palsy was diagnosed. Those under 19 years of age and over 65 years of age were excluded from the study. Furthermore, relapsed palsy, old diagnosis, pregnancy, lactation, fasting, mental illness, cooperation disorders, malignancies, immunocompromisation, second causes of facial paralysis such as skull fracture, sharp trauma, iatrogenic, gastrointestinal absorption disorders, and magnesium supplementation were excluded.
Measurement of Serum Magnesium Concentration
Serum magnesium levels were determined by atomic absorption spectrometry. Atomic absorption spectrometry is considered a reference method for the determination of magnesium, and its sensitivity and accuracy are advantages. On the other hand, its disadvantages are technical features, the use of flammable gases, and their cost. 16 It is the widely used instrumented analysis method, providing absorption of the sent electromagnetic rays of the element atoms gasified by increasing the temperature. The method calculates the absorbed beam according to the Lambert-Beer law. In this method, the atom or substance passes from the low to high energy levels by absorbing the appropriate wavelength in the transmitted beam. The atom, which is in an excited state for 10−6 and 10−9 seconds, then returns to its original state by giving back the absorbed beam. To implement the method, the blood sample taken from each participant was transferred to biochemistry tubes, centrifuged for 10 minutes at 3000 rpm (Nuve NF-800). Separated serum was kept at −20°C. On the day of processing, all serum samples were carefully mixed and rotated to obtain the appropriate temperature (15°C-18°C). Then 1 mL of serum and 1 mL of 20% TCA were taken into Falcon tubes, respectively. The tubes were kept in an oven at 90°C for 15 minutes. Then they were cooled and centrifuged. The obtained supernatants were taken into other tubes and applied atomic absorption spectrometry (UV 1800 240V Shimadzu, serial no: A11454601759 CD).
Calibration for Atomic Absorption Spectrometry
A 100 ppm was taken from the 1000 ppm ready standard solution. Five standard solutions were prepared according to the sample concentration samples at 100 ppm. Then these prepared standards were fed to the devices. A calibration chart was obtained from the device. The concentration in the sample was prepared according to the chart. Thus, the device calculated the concentration in the sample. If faulty, the device cannot be calibrated.
Statistical Analysis
The variables in the 2 groups were assessed and compared using statistical analyzes. Statistical analyzes were performed with IBM SPSS version 20.0 (IBM Corp). Using the Kolmogorov–Smirnov test, it was determined whether continuous variables showed a normal distribution. Parametric and nonparametric tests were applied for normally and nonnormally distributed variables, respectively. Only magnesium variables were found to be nonnormally distributed in the Bell’s palsy group. Therefore, the Mann-Whitney U test was used in the comparison of magnesium scores between the groups. In addition, to compare between the male and female subgroups, the Mann-Whitney U test was applied. In the correlation analyses, Spearman’s correlation test and Pearson’s correlation test were used. For other continuous variables, the independent sample t test was used in comparisons between groups. Fisher’s exact test was applied to compare categorical variables. A P value <.05 was considered statistically significant.
Results
Table 1 presents the comparison between the groups in terms of individual characteristics and serum magnesium levels. The 2 groups were statistically similar in terms of age (P = .846), gender (P = 1.0), and BMI (P = .410). However, serum magnesium concentration exhibited a significant difference between the groups. In other words, Bell’s palsy patients had significantly lower serum magnesium levels (µg/dL) compared to healthy controls [11.44 ± 1.54 (8.9-15.8)] versus [27.35 ± 2.82 (24.3-36.2); P < .001; Table 1].
Comparison Between the Groups in Terms of Individual Features.
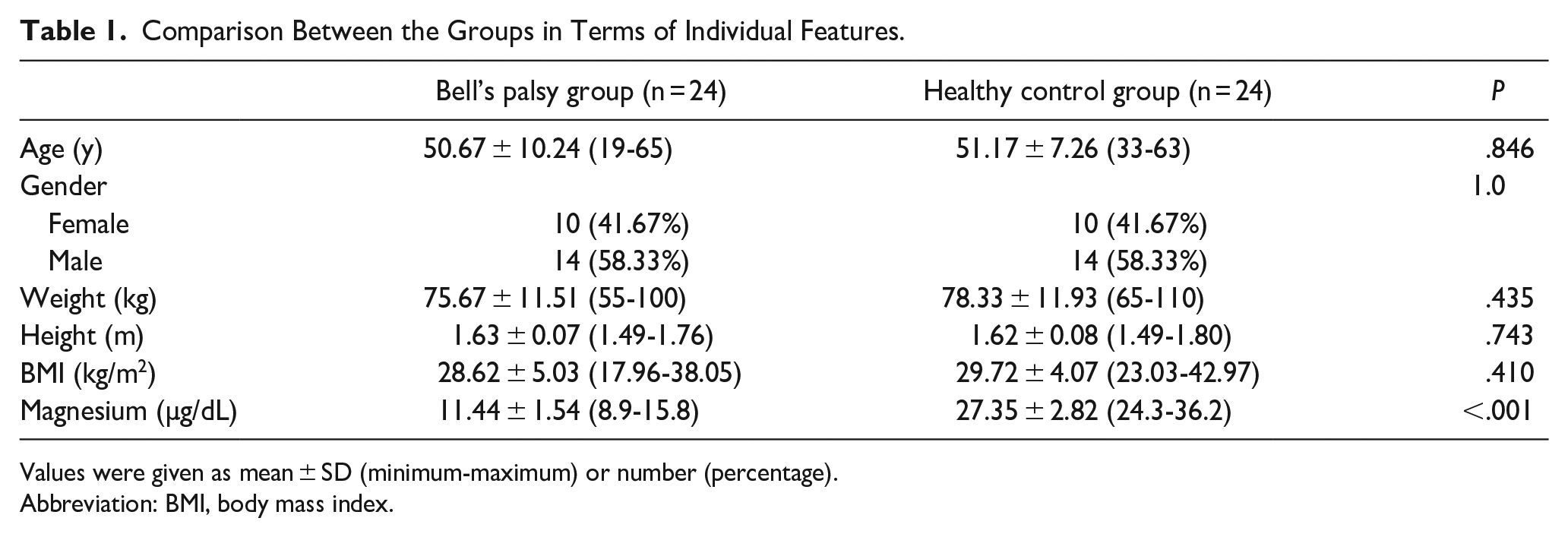
Values were given as mean ± SD (minimum-maximum) or number (percentage).
Abbreviation: BMI, body mass index.
Table 2 presents the comparison between male and female patients in terms of individual characteristics and magnesium levels. There were no significant differences between male and female patients in terms of serum magnesium levels (P = .616).
Comparison Between Male and Female Patients.
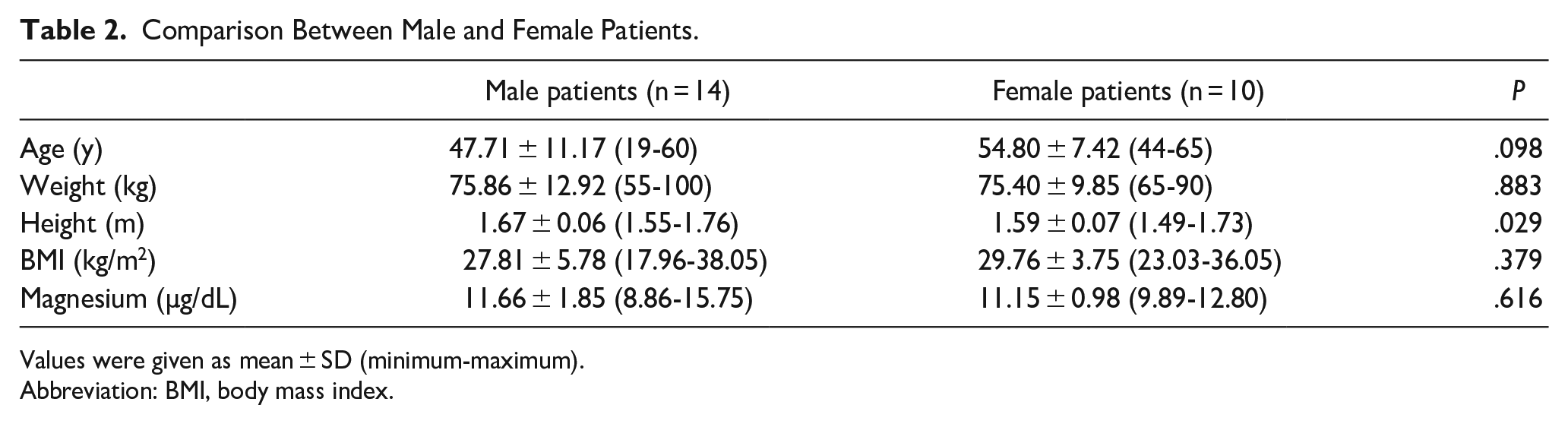
Values were given as mean ± SD (minimum-maximum).
Abbreviation: BMI, body mass index.
Table 3 presents the correlations between serum magnesium levels and other valuables, such as age, weight, height, and BMI. No significant correlations were found between serum magnesium levels and age, weight, height, BMI in patients, controls, and all participants.
Correlations of Serum Magnesium Levels With Other Valuables.
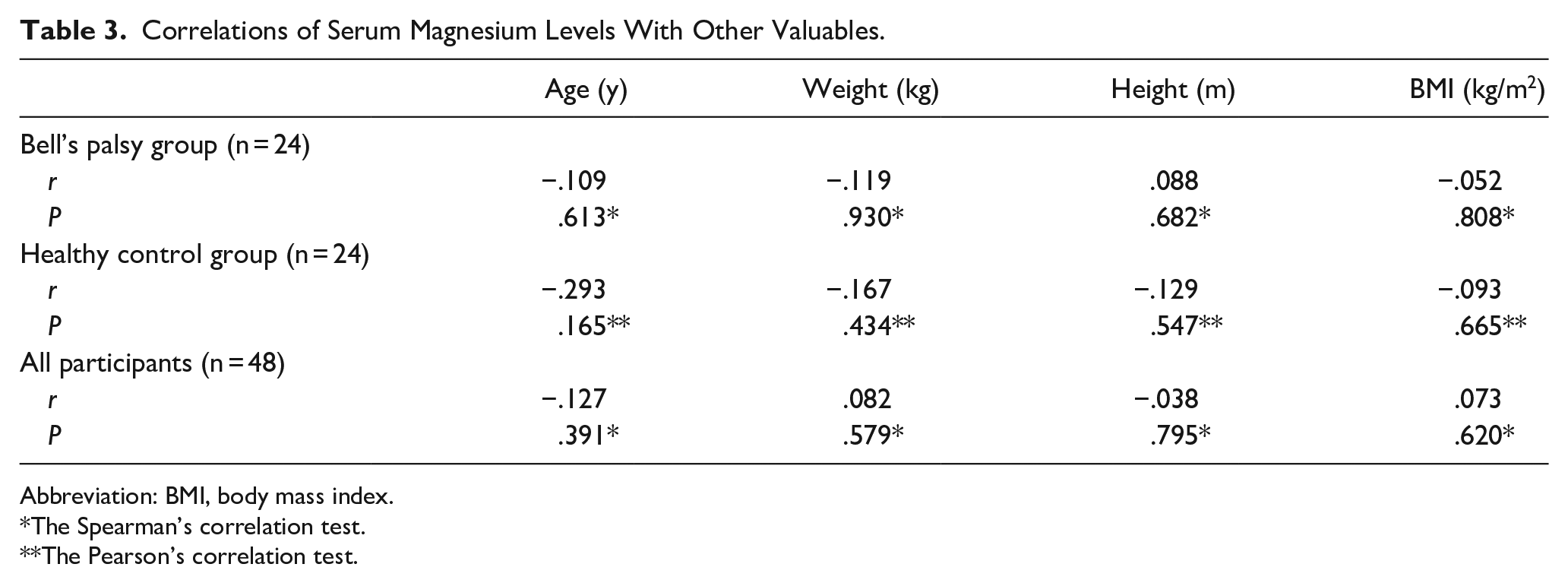
Abbreviation: BMI, body mass index.
The Spearman’s correlation test.
The Pearson’s correlation test.
Discussion
In this case-control study, serum magnesium levels were investigated in Bell’s palsy patients and matched healthy controls. According to the results of the statistical analysis, serum magnesium levels decreased in patients with Bell’s palsy compared to healthy controls. Therefore, decreased serum magnesium levels may be associated with Bell’s palsy. However, to our knowledge, this is the first report to address magnesium status in patients with Bell’s palsy. In addition, we cannot conclude whether a decrease in the concentration of magnesium is a cause or a consequence of Bell’s palsy by the case-control study design. Therefore, more studies are needed to address this topic in more detail.
Various potential common mechanisms can be put forward that underlying coexisting magnesium deficiency and Bell’s palsy. Magnesium deficiency is associated with hyperglycemia, preeclampsia, migraine, inflammation, and oxidative stress.3-7 These conditions are also reported risk factors related to Bell’s palsy.10-13 Furthermore, Bell’s palsy is considered peripheral neuropathy of the facial nerve, 9 and the connection of magnesium deficiency with peripheral neuropathy has previously been reported previously.14,15 Taking all together, the logical and scientific background of the coexistence of magnesium deficiency and Bell’s palsy emerges.
Magnesium is also involved in the immune response as a cofactor for immunoglobulin biosynthesis and other reactions that participate in the functions of T and B cells. 17 Furthermore, magnesium is required as a synthesizer, transporter, and activator of vitamin D, which is an important molecule in the fight against infections. 18 Another reasonable basis for the relationship between magnesium deficiency and Bell’s palsy is the infection-predisposing role of magnesium deficiency 18 and infection-related nature of Bell’s palsy. 19 Therefore, the association of magnesium deficiency with infection-related diseases such as Bell’s palsy is scientific and worth considering.6,7,17-20
In the present study, low serum magnesium concentration was determined in patients with Bell’s palsy. Taking into account the similarities between Bell’s palsy and magnesium deficiency mentioned above,3-7,10-13 this result was reasonably expected and is compatible with the hypothesis of the study. In addition, the finding of a low serum magnesium concentration in patients with Bell’s palsy can provide some questions and ideas for future studies. For example, (a) Is there a link between serum magnesium concentration and Bell’s palsy severity? (b) Is there a link between serum magnesium concentration and Bell’s palsy recovery? (c) Can magnesium supplements treat Bell’s palsy?
Although magnesium status has been investigated in many disorders, 21 no report to date addressed the possible relationship between this important element and Bell’s palsy. For this reason, we cannot mention comparative results from different studies, and thus the discussion on the topic in this study lacks depth and satisfaction.
Previous studies have reported that magnesium is indispensable for all; however, it is of greater importance in women 22 and aging. 21 However, our results from the subgroup analysis comparing male and female patients gave similar magnesium levels in terms of gender. In addition, there was no significant correlation between magnesium and age in the patients. These results suggest that the relationship between Bell’s palsy and magnesium may not be related to gender or aging.
In addition, there are some limitations to this study. First of all, it should be noted that the study is a single-center study and the number of cases is small. These may limit the generalizability and reliability of the results. Another limitation, the thought of whether the low concentration of magnesium is a cause or a consequence of Bell’s palsy is sensible, because magnesium deficiency is related to intake, absorption, renal excretion, and drugs-age interactions. 20 Therefore, the disorder may have caused patients to have difficulty eating and drinking leading to a reduced magnesium intake. Finally, the lack of answers to the aforementioned questions in this study should be considered as other limitations. However, it should be taken into account that this is the first study on the research topic and thus these limitations can be tolerated. Also, the mentioned limitations can give some motivations and ideas for future studies.
In conclusion, the results suggest an association between decreased serum magnesium concentration and Bell’s palsy. However, this study should be confirmed by future research and its limitations should be considered. In addition, future studies should focus on the role of magnesium in severity, recovery, and treatment of Bell’s palsy. After detailed studies, if the role of magnesium in Bell’s palsy is proven to be completely correct, the physiopathological mechanisms underlying the disorder can be more understandable. In addition, more effective diagnostic and therapeutic processes can be achieved in patients with Bell’s palsy.
Footnotes
Acknowledgements
The authors thank to Prof Dr Halit Demir for biochemical measurements.
Authors’ Note
The copyright transfer statement and the submission letter have been signed by all authors.
Author Contributions
CYD and NB: conception and design of the work, recruitment and treatment of participants, acquisition of data, analysis and interpretation of data, draft of the manuscript. All authors read and approved the final manuscript.
Data Availability Statement
Data supporting the conclusions in this study are available from the corresponding author on a reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Van Yuzuncu Yil University (date: November 17, 2023; no. 2023/12-02). Written informed consent for this research was obtained from the patients.