
Abstract
Solitary fibrous tumors (SFTs) are a rare type of soft tissue tumor first identified as arising from pleura and usually arising in the thoracic cavity. The incidence of SFTs arising in the head and neck region is much lower, accounting for about 7% of SFT cases. Involvement of the larynx specifically is exceedingly rare and can have inconspicuous presentations, making them challenging to diagnose. This case report represents a patient with a history of urothelial cancer and obstructive sleep apnea who was ultimately found to have a fibrous tumor of the larynx, which was confirmed by histopathology and immunohistochemistry and treated with transoral microsurgical resection. This case report aims to shed light on an infrequently documented location of a solitary laryngeal fibrous tumor and a unique clinical presentation of this rare pathology and its successful surgical management.
Introduction
Solitary fibrous tumors (SFTs), previously known as hemangiopericytomas, are a type of rare soft tissue tumor arising from fibroblastic mesenchymal stem cells. 1 SFTs account for less than 2% of all soft tissue masses, with an annual incidence estimated at 0.35 per 100,000 individuals.2,3 SFTs usually affect adults of ages ranging from 20 to 70 years. 4 SFTs were first identified as soft tissue tumors arising from pleura in 1939 and have been known by various names, including benign mesothelioma and pleural fibroma, in the past. 5 While first identified in the pleura, SFTs have been documented as occurring in extra-pleural locations throughout the body, such as the abdominal cavity, viscera, meninges, and head and neck.5,6 Head and neck locations are more unusual in which SFTs have been reported and account for about 7% of SFT cases. 4 While cases involving the head and neck have been reported, cases involving the larynx are exceedingly rare and can have inconspicuous clinical presentations. 7 Herein, we present a report of a patient with a medical history of urothelial cancer and obstructive sleep apnea who was identified to have a fibrous tumor of the larynx. This case report highlights a rare presentation of a SFT occurring in an uncommon location within the larynx.
Case Presentation
A 59-year-old man presented for a laryngeal mass that was found incidentally on imaging for surveillance of urothelial cancer. The patient had undergone surgical resection and chemoimmunotherapy for urothelial cancer, and there was no evidence of disease for 2 months at the time of the imaging, with all treatments completed 2 years before presentation. The patient noted chronic intermittent dysphonia but denied any dysphagia or odynophagia. The surveillance CT chest, abdomen, and pelvis revealed a 3.4 × 3.4 × 3.9 cm soft tissue attenuation mass at the level of the vocal cords on the left.
A repeat dedicated CT neck was completed, which showed a 3.5 × 3.8 cm left supraglottic soft tissue mass with extension to the left false vocal cord. No pathologically enlarged cervical lymph nodes were identified (Figure 1A and B). A review of previous imaging from urothelial cancer surveillance found the initial development of a suspected mass at the level of the vocal cords 1 year before presentation. The patient also had been diagnosed with obstructive sleep apnea and had been utilizing continuous positive airway pressure at night for 5 years. Laryngoscopy revealed a large laryngeal mass involving the left larynx/hypopharynx, with the inability to visualize the left vocal cord due to mass effect and concerns for airway compromise (Figure 1C).
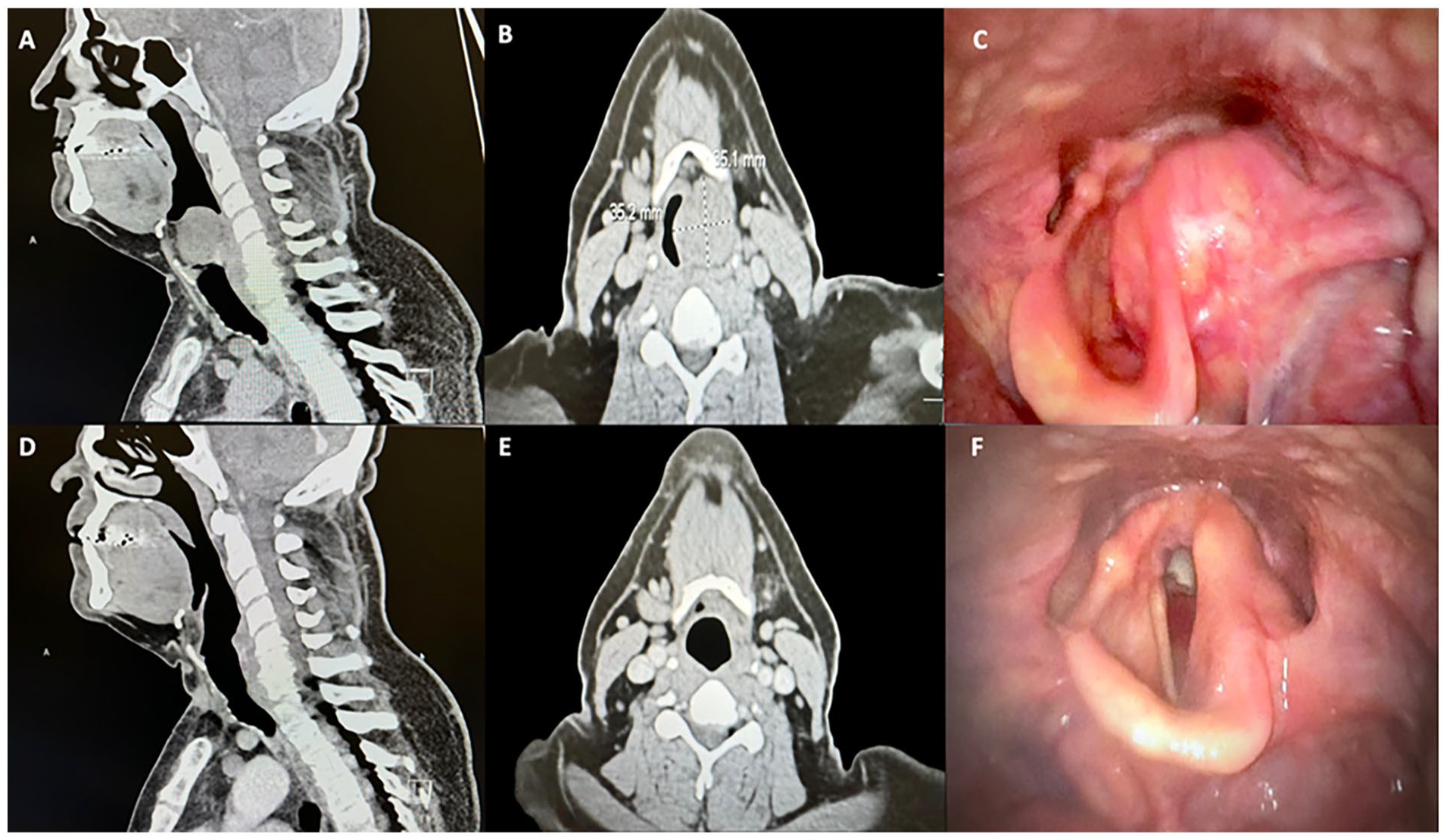
Preoperative and postoperative imaging of a solitary fibrous tumor in the larynx. (A) Sagittal and (B) axial preoperative CT images of the laryngeal mass. (C) Preoperative Laryngoscope view. (D) Axial and (E) sagittal postoperative CT imaging following resection. (F) Postoperative laryngoscope view.
The patient underwent transoral microsurgical resection of the laryngeal mass and tracheostomy placement. Surgical resection, including a carbon dioxide laser, was utilized with significant blunt dissection of the laryngeal tumor. Intraoperatively, the surrounding mucosa was noted to be adherent to the mass. The mass was dissected until it was noted to be freely mobile within its capsule. After significant sharp and blunt dissection, the mass was uncovered from the overlying mucosa. It was slowly mobilized from the left hypopharyngeal and the laryngeal tissues. The mass was then removed and sent for fresh permanent pathology lymphoma protocol and ruled out carcinoma and any benign tumor pathology. The patient tolerated the procedure well without any complications.
Pathology revealed fibrotic soft tissue, focally active chronic inflammation, and possible sampling of the underlying bland spindle cell lesion. The final diagnosis revealed a SFT. Immunostains of the spindle cells are diffusely, strongly positive for CD34 and negative for CD117, smooth muscle actin, Desmin, S-100, and pan-cytokeratin. Immunohistochemical stain for signal transducer and activator protein 6 (STAT6) is positive in a nuclear pattern, which is a highly specific finding of SFT (Figure 2).
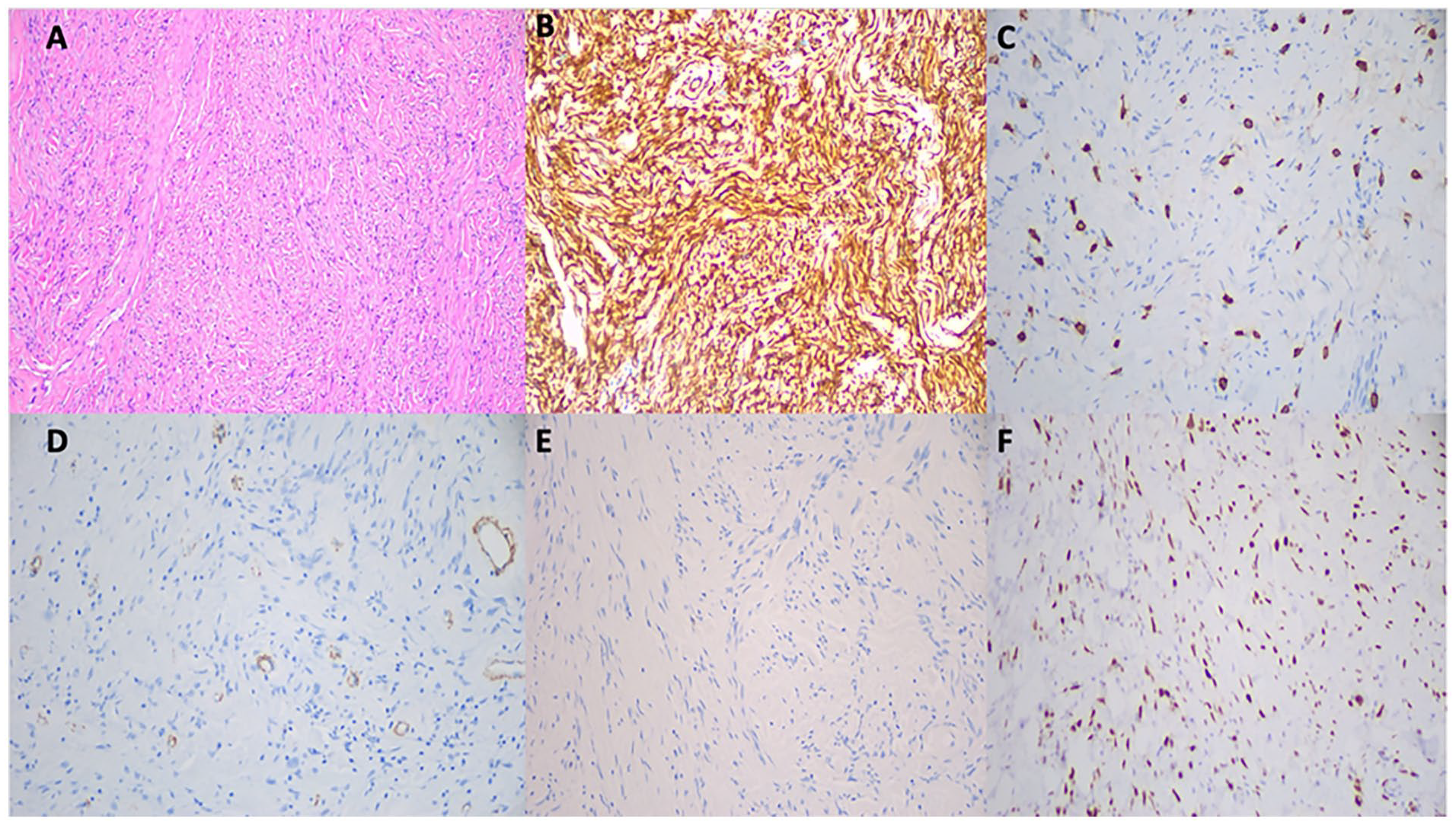
Postoperative histologic micrographs. (A) Histologic section (H&E 100× magnification) of the neoplasm shows a sclerosing/fibrotic spindle cell neoplasm with no overt histologic features of malignancy. There is no pleomorphism, necrosis, or marked increase in mitoses. (B) Immunostains of the spindle cells are diffusely, strongly positive for CD34 (200× magnification) and (C) negative for CD117 (200×), (D) smooth muscle actin (200×), and (E) Desmin (200×). (F) Immunohistochemical stain for STAT6 (200×) is positive in a nuclear pattern, a highly specific finding of a solitary fibrous tumor.
Postsurgical CT imaging revealed no soft tissue prominence or enhancing mass in the larynx, and no pathologically enlarged cervical adenopathy was found (Figure 1D and E). A postoperative laryngoscope was also completed, which revealed complete resolution in the previous tumor, full visualization of the hypopharynx and true and false vocal cords, with complete mobility of the vocal cords with glottic closure (Figure 1F). Currently, the patient is without dysphonia, with full vocal cord mobility, and without obstructive sleep apnea. The patient has had no clinical or radiologic evidence of disease 15 months postoperatively.
Discussion
This case represented a rare location and presentation for a SFT. The anatomical location of this tumor contributed to the complexity of the case, given the indistinct clinical presentation and potential for respiratory compromise. Previous studies have identified dysphonia as the most common presenting symptom of laryngeal fibrous tumors. 8 This emphasizes the importance of including laryngeal tumors in the differential diagnosis for a patient with unexplained hoarseness. Chronic dysphonia, primarily when occurring for more than 3 weeks, should be evaluated for a potentially identifiable underlying cause. 9 Obstructive sleep apnea itself was also an indication in this patient’s case to consider the potential for an upper aero-digestive tract lesion. 10 There have been previously described case reports of SFTs of the tongue and oropharynx presenting with obstructive sleep apnea.10,11 SFTs have also been identified to cause paraneoplastic phenomena, such as paraneoplastic osteoarthropathy and hypoglycemia. 12 The variety of potential clinical presentations for SFTs makes them very challenging to diagnose as they are uncommon and often not suspected.
STAT6 immunostaining is highly specific for SFTs. 13 The STAT6 gene encodes a cytoplasmic protein that functions as a transcription factor. 1 In contrast, NGFI-A binding protein 2 (NAB2) is a transcriptional repressor that functions to repress the transcription factor Early growth response 1 (EGR1). 1 The intrachromosomal NAB2-STAT6 gene fusion on chromosome 12 has been identified to promote STAT6 nuclear expression and SFT oncogenesis through the fusion of the activation domain of STAT6 with the DNA-binding domain of NAB2.1,13 NAB2-STAT6 translocates to the nucleus and disrupts the repressive function of NAB2 on EGR1, ultimately resulting in upregulated EGR1 function. 14 Since NAB2-STAT6 translocates to the nucleus, nuclear STAT6 immunostaining is especially helpful in diagnosing SFTs, as was true in this patient’s case. 14
Once the diagnosis of a SFT has been confirmed, the treatment of choice is typically surgical resection; however, 10% to 30% of patients experience a recurrence of their tumor. 15 This significant recurrence rate suggests an area for consideration in the management of these tumors. SFTs have been determined to be fairly vascular tumors. 4 Current studies, including two prospective phase II clinical trials, have shown that antiangiogenics may be effective in managing these tumors and that their use should be considered. The main notable exception for the use of antiangiogenics is in dedifferentiated SFTs, as chemotherapy is usually the management of choice for these patients.4,16 While surgical resection currently remains the first-line treatment of SFTs for most patients, these studies suggest likely benefits from incorporating antiangiogenics when feasible. 4 In addition to antiangiogenic therapies, NAB2-STAT6 has also been identified as a potential therapeutic target in the treatment of SFTs. 16 Antisense oligonucleotide (ASO)-based therapy has recently become an area of interest as this therapy is able to target the C-terminal of STAT6 transcript in the NAB2-STAT6 fusion. 1 This therapy has been shown to reduce the expression of NAB2-STAT6 fusion transcripts and tumor growth in vitro, providing an encouraging area of research for future therapies. 1 Future studies will need to continue to evaluate the effectiveness of these potential therapies and compare them to the current recommendations of surgical resection.
Conclusions
This rare case of a SFT of the larynx represents both a rare location for a SFT as well as a rare and inconspicuous clinical presentation. This case report serves to add to the current understanding of the clinical workup of SFTs by raising awareness to their clinical manifestation in the head and neck region. This patient’s tumor presented clinically in a rather benign way that could have led to negative consequences had the tumor begun to compromise this patient’s airway. The anatomical location and potential for respiratory compromise in this patient highlight the need for a low threshold for further clinical workup in the patient with persistent dysphonia. SFTs can be difficult to identify clinically and warrant immunohistochemistry evaluation to confirm the diagnosis. STAT6 is a particularly important marker for diagnosis but has also recently become a potential therapeutic target in treating SFTs. While ASO-based therapy against STAT6 and antiangiogenic therapy are currently being studied as potential future therapies, further research is needed to compare these therapies to the current surgical treatment of choice, especially in sensitive locations such as the head and neck.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
The study complied with institutional standards for patient confidentiality and ethical conduct. The manuscript was reviewed by an Institutional Review Board and received ethical approval.
Consent to Participate
Not applicable.
Consent for Publication
Written informed consent for publication of clinical details and images was obtained from the Institutional Review Board, as well as disclosures from the patient.
Data Availability
Data sharing does not apply to this article as no datasets were generated or analyzed during the current study.