
Abstract
Solitary fibrous tumor/hemangiopericytoma (SFT/HPC) is extremely rare, and most of them are immediately treated for radical resection. However, the information concerning its natural history remains unclear. In this report, we presented a patient with parapharyngeal SFT/HPC, who was not immediately treated with surgical resection at first diagnosis. After approximately 3 years, the tumor volume doubling time (TVDT) and specific growth rate (SGR) could be measured through 3 serial magnetic resonance imagings. The TVDTs in the early and late pretreatment stages were 350 and 180 days, respectively, while the SGRs were 0.002 and 0.003, respectively. The growth rate of this disease entity is generally slow and may accelerate in the disease process.
Keywords
Introduction
Among head and neck neoplasms, tumors arising in the parapharyngeal space (PPS) are relatively rare, occupying only 0.5%. 1 The most common types of tumors in PPS are salivary gland (45%) and neurogenic tumors (45%). Solitary fibrous tumor/hemangiopericytoma (SFT/HPC) was recognized as a new entity in 2016 World Health Organization (WHO) classification and uncommonly seen in PPS. Given the low incidence and immediate operation, it is not easy to obtain clinical data concerning SFT/HPC’s natural history which only one literature reported. 2 Here, we reported a case of SFT/HPC arising in PPS, and its tumor volume doubling time (TVDT) and specific growth rate (SGR) were calculated based on serial magnetic resonance imagings (MRIs).
Case Report
A 46-year-old woman presenting with a repeated headache and galactorrhea was admitted to our hospital 3 years ago. Magnetic resonance imaging revealed a microadenoma in the pituitary gland, and a mass in the left PPS measuring 22.9 mm × 15.1 mm × 22.9 mm (Figure 1A). However, the patient refused any local therapy for the PPS mass. Approximately 2 years later, the patient complained of mildly restricted mouth open lasting for 2 months. Magnetic resonance imaging examination revealed that the lesion in the pituitary was stable while the mass in the PPS had increased to 39.8 mm × 30.3 mm × 35.2 mm in size and adhered to the left parotid gland. The lesion was of heterogenously high-signal intensity on T2-weighted images and iso-signal intensity on T1-weighted images (Figure 1B-C).
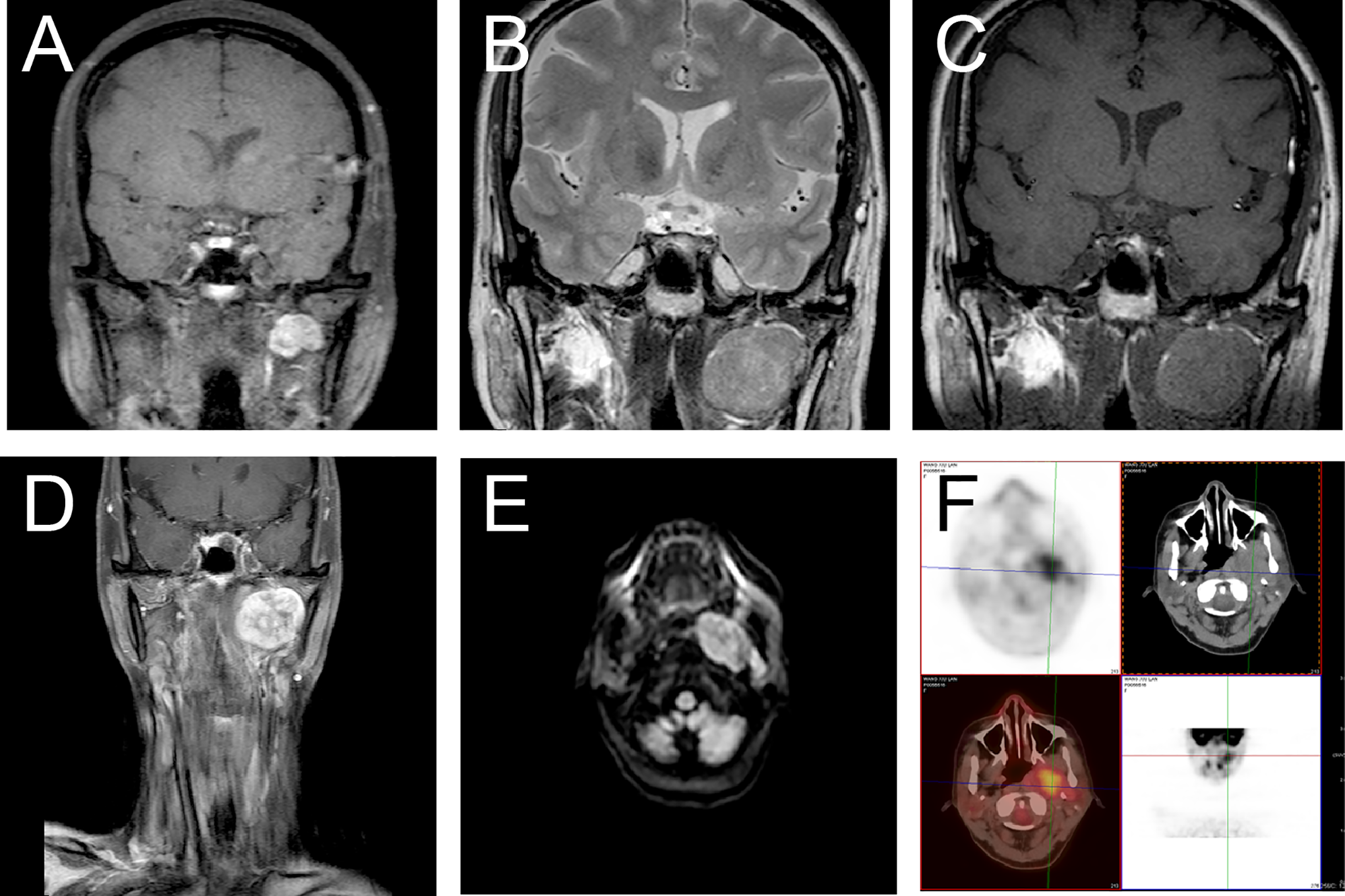
Sequential radiographs of the patient with solitary fibrous tumor/hemangiopericytoma (SFT/HPC) (A) The initial magnetic resonance imaging (MRI), performed 3 years previously, presented a mass in the left parapharyngeal space. (B-C) The second MRI revealed a heterogeneous high intensity lesion on T2W (B) and isointensity lesion on T1W (C). (D-E) The third MRI showed coronal T1-weighted image (T1WI) (D) with contrast showed a strong enhancement except the inner fiber. On diffusion-weighted imaging (DWI) (E), the lesion has high signal. (F) Positron emission tomography–computed tomography (PET-CT) reveals increased uptake of 18F-deoxidized glucose (FDG).
After a consultation at a multidisciplinary team, the patient was advised to undergo a radical excision of the mass. However, the patient did not receive operation until 4 months later due to aggravating symptoms. Preoperative MRI disclosed that the mass had further increased to 42.1 mm × 34.6 mm × 46.5 mm. The lesion exhibited inhomogeneous enhancement (Figure 1D) after gadolinium administration (Gd), and heterogeneous high-signal intensities on diffusion-weighted imaging (Figure 1E). Besides, PET scan indicated moderately increased uptake of 18F-deoxidized glucose in the mass and the nodules in the deep lobe of the parotid gland (Figure 1F). On operation, the lesion tightly adhered to the parotid gland’s deep lobe, and therefore piecemeal resection was carried out.
Microscopically, the resected specimen showed a patternless cell growth pattern with alternating hypercellular and hypocellular areas (Figure 2A). The characteristic hemangiopericytoma-like vasculatures were richly distributed in the mesenchyma (Figure 2B). The tumor cells were composed of round to spindle-shaped cells embedded in dense collagen fibers, and the mitotic count was 4/10 high-power fields in some areas (Figure 2C).
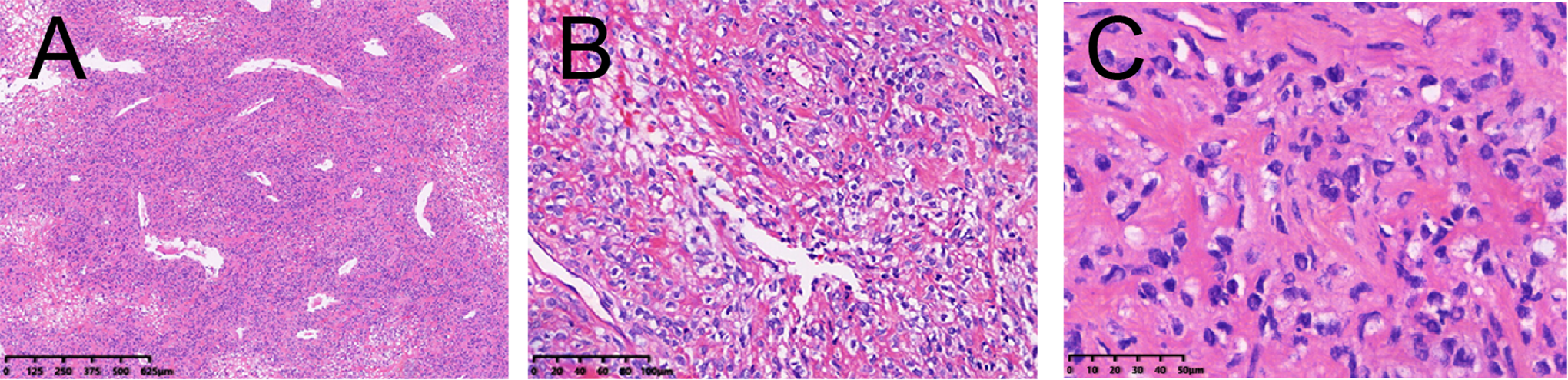
Morphological findings of the solitary fibrous tumor/hemangiopericytoma (SFT/HPC) (A) low-power view of tumor revealed a patternless growth pattern with alternating hypocellular and hypercellular areas and dispersed variable size vessels around the tissue sections. (B) The characteristic staghorn-shaped branching vessels can be seen in tumor. (C) In high-power view, the tumor is comprised round to spindle-shaped cells with collagen fibers and the mitotic figures can be detected.
Due to the restricted operation space, an en bloc resection was not easy to operate and the margin status was indeterminate. Immunohistochemistry demonstrated that the tumor cells were positive for STAT6, CD34, CD99, BCL-2 but negative for CK (pan), s-100, desmin, SMA, HMB45, and CD31 (Figure 3A-F) and the Ki-67 index was 10%. Based on the 2016 WHO classification system of central nervous system tumors, the final diagnosis was SFT/HPC (WHO Grade II).
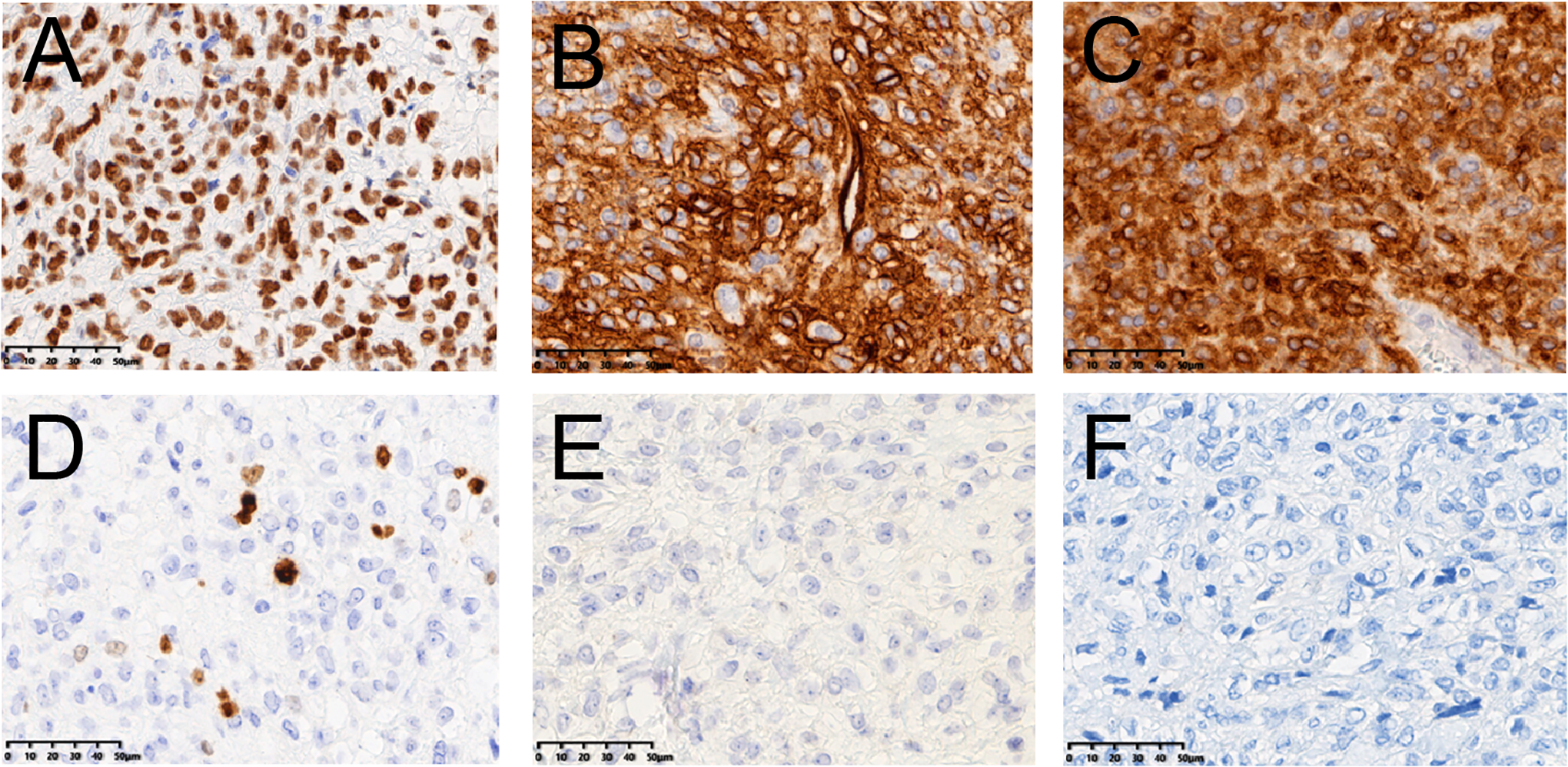
Immunohistochemical staining analysis. It shows positivity for (A) signal transducer and activator of transcription 6 (STAT6) (B) cluster of differentiation 34 (CD34) (C) B-cell lymphoma 2 (BCL-2) (D) Ki-67 (10%), and negative for (E) S-100 and (F) cytokeratin (×400).
Given the high recurrence rate of the disease with an undefined surgical margin, postoperative radiotherapy was recommended for the patient, with a total dose of 60 Gy in 30 fractions. After a follow-up of one year, there was no evidence of recurrence or metastasis.
Interestingly, we obtained 3 MRIs at the initial visit, during the follow-up for pituitary microadenoma after 2 years, and another 4 months later before surgery. We obtained data on tumor growth rate in 2 stages. Tumor volume doubling time could be calculated based on 3 MRIs at 3 time points, precisely day 0, day 847, and day 971. We measured the tumor volume by ellipsoid volume = l × w × h (π/6). Using Schwartz’s equation 3 : TVDT = (T−T0) × log2/(logV/V0), where (T−T0) represents the time interval between the 2 imaging studies, and V0 and V indicate the volume of the tumor at the 2 measurement time. Tumor volume doubling times were calculated to be 350 days and 184 days in 2 intervals. As an alternative, SGR was evaluated, specifically SGR = ln(V/V0)/(T–T0). 4 In our case, the SGRs were 0.002 and 0.003, respectively.
Discussion
Solitary fibrous tumor/hemangiopericytoma is uncommon, representing only 1% to 2% of all soft tissue tumors and can occur in almost any part of the body. 5 The incidence of SFT/HPC in the parapharyngeal region is relatively low. Up to date, only 22 cases of SFT/HPC arising in this region were reported in English literature (summarized in Table 1).6-27
Clinical Characteristics of Reported Cases.
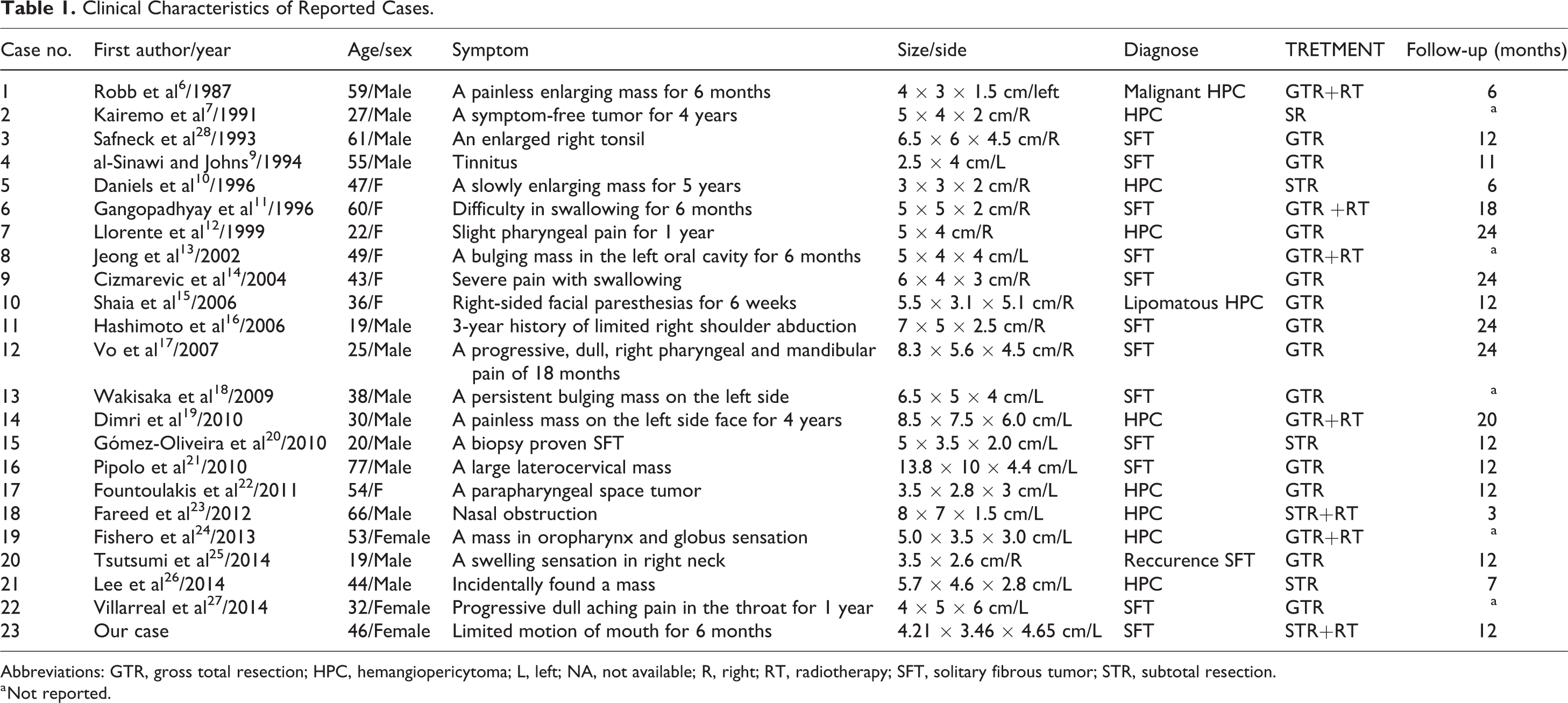
Abbreviations: GTR, gross total resection; HPC, hemangiopericytoma; L, left; NA, not available; R, right; RT, radiotherapy; SFT, solitary fibrous tumor; STR, subtotal resection.
a Not reported.
Solitary fibrous tumor/hemangiopericytoma is a kind of slow-growing tumor. To our knowledge, there is only one English literature describing the TVDT of SFT/HPC arising in the pleura. 2 We are the first to report the TVDT and SGR of extrapleural SFT/HPC. In pulmonary lesions, the tumor growth rate is crucial in distinguishing the likelihood of malignancy and histologic subtypes. However, the correlation between the growth rate and prognosis in SFT/HPC is uncertain. Due to the patient’s willingness in our case, the tumor development period was more than 2 years without any intervention. Therefore, we obtained 3 serial MRIs to divide the tumor growth process into 2 stages. Interestingly, we could infer the growth rates in 2 stages and found the second growth rate was faster than the first. The difference may be attributed to the growth space, in which the tumor growth space was relatively unrestricted in the first interval. In contrast, the tumor growth was confined in the second interval resulting in the apparent symptom. Additionally, some internal and external stimulus could change biological behavior such as genetic events, host immunity, cell loss, and so on. The variabilities in volume measurements and the different interval time may also account for the growth rate change. It reported that SGR shows more superior to quantify tumor growth rate compared with TVDT. 4 From the result of SGR in our case, the later pretreatment interval is accelerated, similar to the TVDTs.
In conclusion, our case is the first to analyze the growth rate in different stages. Using 2 indexes—TVDT and SGR, we find the overall growth rate is slow and accelerated over time. An additional study to elucidate the correlation between tumor growth behavior and the prognosis is necessary. Our results showed the uncertainty of SFT/HPC biological behavior, so long-term follow-up is warranted.
Footnotes
Authors’ Note
Ethical approval is not applicable for this article. This article does not contain any studies with human or animal subjects. Verbal informed consent was obtained from the patient for her anonymized information to be published in this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from Chinese Medicine Research Program of Zhejiang Province [2018ZZ014] and Zhejiang Provincial Key Discipline of Traditional Chinese Medicine [2017-XK-A32].