
Abstract
Solitary fibrous tumors (SFTs) are rare mesenchymal tumors that occur in various soft tissues and organs throughout the body. Superficial SFTs in the head and neck region are uncommon and reports of such cases are limited. An elderly Japanese woman in her 80s presented to our clinic with a smooth mass in the right parotideomasseteric region. Ultrasonography and magnetic resonance imaging revealed a well-defined subcutaneous mass measuring 20 mm. For a definitive diagnosis and treatment, surgical resection was performed under local anesthesia. Intraoperatively, a brown-colored tumor was identified beneath the skin, without surrounding tissue adhesion, and was completely excised. Immunohistochemistry, revealing the expression of STAT6, confirmed the diagnosis of SFT. Based on the SFT risk classification, this case was classified into the low-risk group, and no recurrence occurred during the 4 year postoperative period. According to the 2020 World Health Organization Classification of Soft Tissue Tumors, SFTs belong to the intermediate category with recurrence potential. In previous studies, cases of positive margins and recurrence have been reported in superficial SFTs, and SFTs may show benign features on clinical presentation but require precise surgical manipulation. Therefore, it is crucial for otolaryngologists to gain a comprehensive understanding of this tumor for appropriate treatment.
Introduction
Solitary fibrous tumors (SFTs) are rare tumors of mesenchymal origin that occur in the soft tissues throughout the body.
The head and neck region accounts for approximately 10% of all SFTs, with superficial SFTs comprising approximately 15% of all cases compared to deep-seated SFTs.1,2 Therefore, superficial head and neck SFTs are rare.
According to the 2020 World Health Organization Classification of Soft Tissue Tumors, SFTs are categorized as intermediate and are notable for their possibility of recurrence. 3
This report presents a case study of a superficial SFT located in the parotideomasseteric region, detailing its clinical presentation, imaging studies, surgical procedures, and postoperative progress.
In addition, we describe the immunochemical examinations essential for diagnosing SFT, risk assessment, and surgical considerations.
Case Report
The patient, an octogenarian Japanese woman, had been aware of a mass in the right parotideomasseteric region for 3 years. The mass gradually increased in size, prompting further evaluation in our department.
Palpation revealed a mobile, smooth, elastic, firm mass with no signs of tenderness.
Ultrasonography revealed a 20 mm × 10 mm borderline, internally homogeneous, hypoechoic lesion, and magnetic resonance imaging (MRI) demonstrated a 20 mm × 18 mm × 13 mm mass with a T1 low signal, T2 mildly high signal, and contrast enhancement (Figure 1).

Axial MRI shows a well-defined, ovoid mass with a capsule situated external to the right parotid gland. (a) T1WI showing homogeneous low signal intensity. (b) T2-weighted image showing mildly high signal intensity with heterogeneous features. (c) Contrast-enhanced T1WI illustrates the marked and heterogeneous enhancement of the lesion. MRI, magnetic resonance imaging; T1WI, T1-weighted image.
Fine needle aspiration (FNA) cytology suggested a suspicious malignancy, leading to resection under local anesthesia for definitive diagnosis and treatment.
Intraoperatively, a skin incision promptly exposed the tumor surface beneath the skin, with no adhesions to the dermis detected. Given the suspected malignant FNA results, the surrounding fatty tissue was also resected.
Conversely, the dermis and parotid capsule adjacent to the tumor were easily dissected without adhesions; therefore, these tissues were not excised concurrently.
The tumor was completely excised, the surgical site was irrigated with physiological saline, and the surgery was concluded.
Macroscopic examination revealed a brown 22 mm × 20 mm mass with a smooth capsule (Figure 2a).
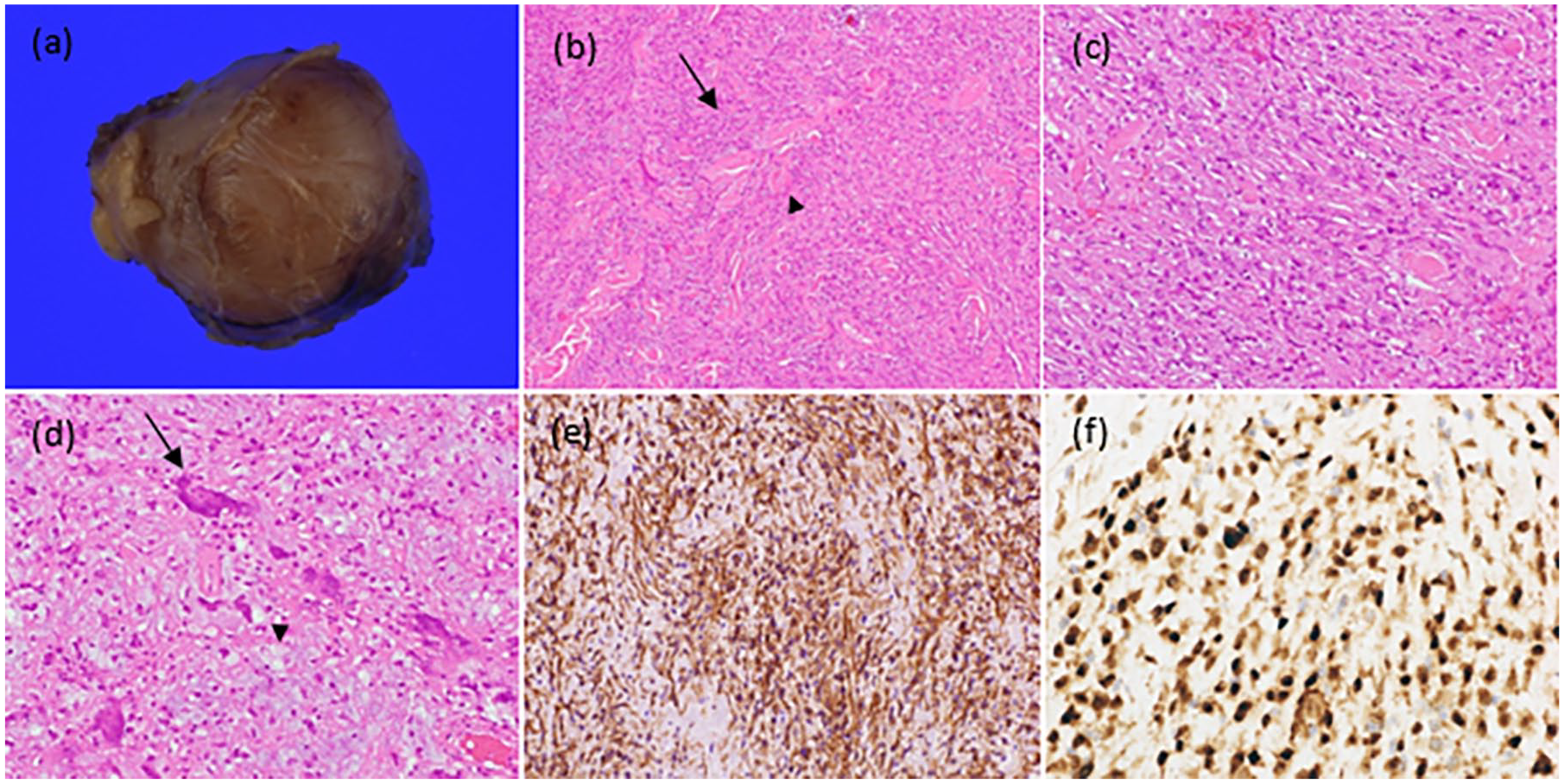
(a) Gross examination reveals a brownish mass encapsulated with a smooth surface. (b) Photomicrograph at ×100 magnification stained with hematoxylin and eosin demonstrates spindled cells (arrow) with collagen bundles (arrowhead). (c) Photomicrograph at ×400 magnification stained with hematoxylin and eosin demonstrates low-grade cytological atypia. (d) Photomicrograph at ×400 magnification stained with hematoxylin and eosin demonstrates multinucleated giant cells (arrow) with myxoid stroma (arrowhead). (e) Nuclear CD34 expression is observed in a significant number of tumors histologically. (f) Immunohistochemistry reveals nuclear expression of STAT6 in numerous tumor cells.
Histopathological examination revealed spindle-shaped cells with mild cellular atypia and collagen fibers (Figure 2b). Mild atypia was observed (Figure 2c). In addition, mucinous changes (arrowhead) were observed in some cells, along with multinucleated giant cells (arrow; Figure 2d).
Immunohistochemical staining demonstrated that the tumor cells were positive for CD68 and CD34 but negative for desmin, S-100 protein, and D2-40. The Ki-67 labeling index was less than 1% for the tumor cells (Figure 2e). Based on the positive CD68 and CD34 results, benign fibrous histiocytosis or a superficial CD34-positive tumor was initially suspected. However, additional immunostaining for STAT6 revealed positive nuclei, leading to the diagnosis of SFT (Figure 2f). Resection margins were confirmed as negative, and the patients were categorized into the low-risk group according to the SFT risk classification. The patient remained recurrence-free for the subsequent 4 years and eventually died of unrelated health conditions.
Discussion
SFTs are rare mesenchymal tumors that occur in soft tissues throughout the body. Approximately 10% of these tumors occur in the head and neck region, including the oral cavity, sinuses, neck, and thyroid gland. 1 Superficial SFTs, such as those occurring subcutaneously, account for only 15% of all SFTs compared to their deep-seated counterparts. Consequently, superficial SFTs of the head and neck regions are rare.
In the present case, the tumor was located subcutaneously and showed no adhesion to surrounding tissues. As a result, the resection of the tumor was relatively straightforward. However, despite the apparent ease of removal, it is crucial to highlight that SFTs exhibit a 5 year recurrence rate of 29%, a metastatic rate of 34%, and positive resection margins have been identified as a risk factor for local recurrence. 2
Therefore, precise surgical techniques are essential for the surgical management of these tumors.
The diagnosis of SFT is difficult preoperatively owing to the lack of specific findings on computed tomography, MRI, and FNA. Immunohistochemistry is essential for the definitive diagnosis of SFT.
In this case, the positive CD68 and CD34 findings initially raised the suspicion of fibrous histiocytoma or a superficial CD34-positive fibroblastic tumor.
To further differentiate SFT, STAT6 expression was examined using immunohistochemistry, which revealed a positive nucleus, ultimately confirming the diagnosis of SFT.
In 2013, NAB2-STAT6 gene fusion was identified in SFT, and STAT6 immunohistochemical testing was subsequently proposed. Its diagnostic specificity has been reported to be 98%, making it essential for the definitive diagnosis of SFT. 4
According to the risk assessment model proposed by Demicco et al, 1 factors such as age (>55 years), tumor diameter (>15 cm), mitotic count (>4/10 HPF), and subsequent tumor necrosis (>10%) have been identified as predictive factors for metastasis. 1
In the present case, only age was found to be relevant; as a result, the patient was classified into the low-risk group.
Surgical resection is the standard treatment for SFT. In this case, as there was no adhesion to the surrounding tissue, and considering the patient’s advanced age, a minimally invasive procedure was chosen. Consequently, no combined resection of the dermis or the parotid capsule was performed. Pathological examination revealed that the resection margins were close but negative, and no evidence of recurrence or metastasis was observed 4 years post surgery.
Few studies have documented the excisional margins in superficial SFTs. However, Ganly et al 5 reported that among 12 cases of SFTs in the head and neck region, 3 exhibited positive excisional margins and 2 of them were categorized as superficial.
Based on our experience with this case and previous reports, 2 factors can be considered as the reasons for positive resection margins in superficial SFTs.
First, SFTs often present as smooth tumors with well-defined borders, leading to their initial misclassification as benign tumors when a diagnosis is not established.
Second, the surrounding tissues in the head and neck region are confined to a narrow anatomical space, making it difficult to achieve sufficient margins during surgery.
While superficial tumors, as in this case, are anatomically easier to resect than deep-seated tumors, special attention must be given to tumors with the potential for recurrence, such as SFTs. Otolaryngologists should have a comprehensive understanding of SFT, consider them in the differential diagnosis, and perform precise resections to avoid the risk of positive margins.
In conclusion, this report presents a case of a superficial SFT in an elderly patient. Immunohistochemistry for STAT6 is valuable for accurate diagnosis. Minimally invasive surgery was performed, and 4 years after the surgery, no recurrence or metastasis was observed.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for this case report was obtained from the Juntendo University Shizuoka Hospital Ethics Committee.
Informed Consent
Informed consent for the publication of this case report and any accompanying images was obtained verbally from the patient’s next of kin. The family members were provided with a detailed explanation of the purpose of the report and expressed their consent for the use of the deceased patient’s medical information for educational and research purposes.