
Abstract
Keratoacanthoma (KA) is a self-regressing cutaneous tumor sharing clinical and histopathological similarities with squamous cell carcinoma. It is relatively uncommon and presents diagnostic challenges, particularly in pediatric patients. This paper presents a case study of KA affecting the upper lip keratosis in a 6-year-old girl. Through a comprehensive analysis of the pathogenesis, differential diagnosis, and treatment approaches of KA in children based on existing literature, we aim to offer clinical insights and guidance for practice.
Introduction
Keratoacanthoma (KA) is a skin tumor originating from the epithelium of the hair follicle, commonly observed in adults, predominantly middle-aged and older males. This condition typically manifests as rapidly growing, self-limiting round or oval nodules with central keratinization and raised margins. 1 However, KA is exceedingly rare in children, particularly in the context of occurrences on the upper lip. 2 Given that parents are often vigilant regarding skin irregularities in children and may promptly seek medical evaluation, KA in pediatric cases may exhibit atypical clinical characteristics that can be mistaken for squamous cell carcinoma (SCC) during the diagnosis process, especially in the early stages, thereby complicating the diagnostic challenge.3-6 Although KA is commonly categorized as a benign lesion, its rapid growth patterns and the potential for malignant transformation underscore the significance of early detection and intervention. 7 This study presents a case of keratinizing acanthoma on the upper lip of a 4-year-old girl. The clinical presentation, histopathological characteristics, and treatment outcomes were evaluated, and challenges in the diagnosis and management of the condition were deliberated in conjunction with pertinent literature.
Case Report
The patient, a 4-year-old girl, presented with a progressively enlarging brown nodular lesion on the upper lip. According to parental reports, the lesion had exhibited rapid growth over the past 2 months, with no notable discomfort experienced by the child. Upon physical examination, the lesion appeared as a round, elevated nodule measuring approximately 1.0 cm in diameter. It was covered with a brown crust, affecting the skin, and vermilion border of the midline of the upper lip (Figure 1). The lesion featured a central keratinized plug, displayed no signs of ulceration or hemorrhage, had well-defined borders, and a sessile base, and did not present with redness, swelling, or tenderness in the surrounding tissues. In addition, there was no history of trauma to the affected area. Due to the rapid growth of the tumor and challenges in distinguishing it from SCC, surgical excision was deemed necessary (Figure 2). The lesion was entirely excised during the surgical procedure, and intraoperative rapid biopsy analysis confirmed the absence of residual margins. The histopathological assessment revealed findings consistent with KA, including epithelial hyperplasia, hyperkeratosis, spinous layer thickening, basal nuclei with deep staining and pleomorphism, crater-like structures with central keratinizing plugs, and vitreous keratinocytes. Subsequently, a diagnosis of KA was established based on the observed histopathological characteristics (Figures 3 and 4). Following the surgery, the patient recuperated well.

The initial presentation revealed nodular exophytic lesions on the upper lip, which were obscured by brown-pigmented crusts.

The immediate postoperative assessment.
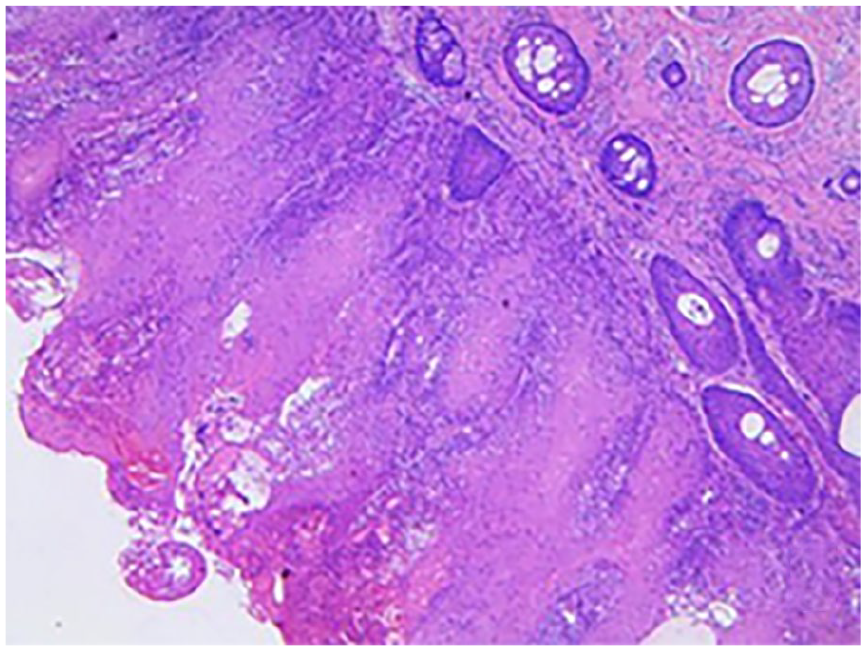
Histological examination showed epithelial hyperplasia with crater-like structures and central keratinizing plugs, along with an increased number of sebaceous glands.
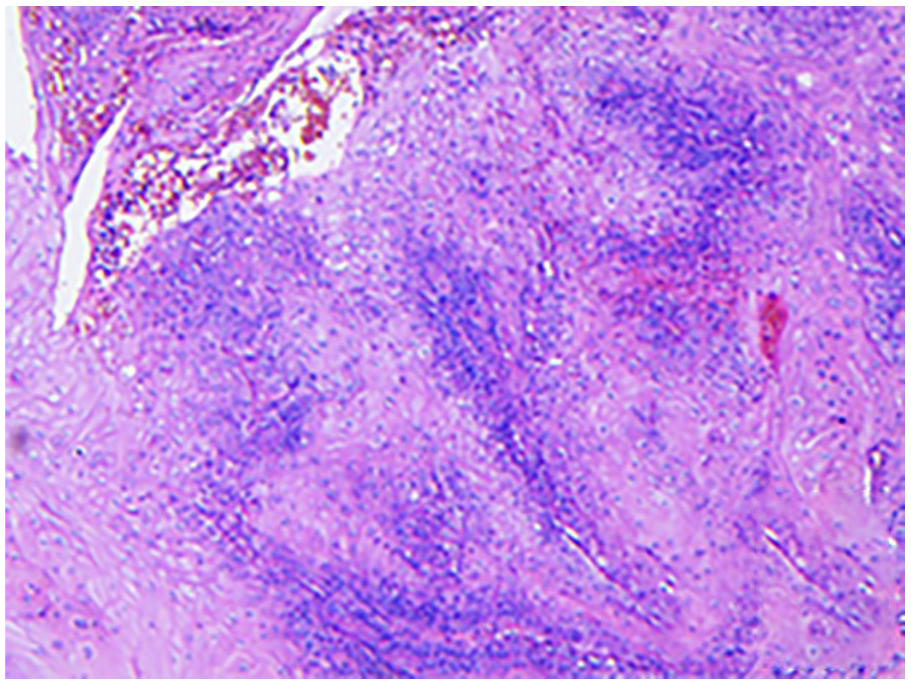
Nuclear atypia was observed, with vitreous keratinocytes being evident.
Discussion
The precise biological characteristics of KA as a cutaneous tumor arising from the hair follicle remain incompletely elucidated. 8 In adults, the development of KA is frequently linked to external factors including ultraviolet radiation exposure and trauma.9,10 Nevertheless, the impact of these factors on pediatric populations has not been definitively established. Some studies propose that KA in children might be correlated with genetic predisposition, localized skin inflammation, or other immunological disorders.11-13 Limited case reports suggest that the pathogenesis of KA in pediatric patients could potentially diverge from that observed in adults, potentially implicating distinct molecular signaling pathways or immune responses.
The differential diagnosis of KA poses a clinical dilemma. KA and SCC both manifest as rapidly growing skin nodules with central keratinizing plugs or ulcers. 14 Consequently, clinicians often encounter challenges in distinguishing between the 2 based solely on their visual appearance during the initial assessment. This diagnostic complexity is further heightened in pediatric cases, as the clinical features of skin tumors in children are typically less pronounced compared to those in adults. Histopathologically, KA is characterized by a central keratinized core and cup-shaped basal architecture, with the orderly and compact arrangement of peripheral cells. However, the differentiation between KA and SCC can be intricate due to shared histological features, such as abnormal cell proliferation and hyperkeratosis. 4 Although immunohistochemical markers such as Ki-67 and p53 can aid in the differentiation between KA and SCC to some extent, there are instances where KA may demonstrate elevated proliferative indices or aberrant p53 expression, necessitating a comprehensive analysis by a clinical pathologist integrating clinical presentations, pathological features, and immunohistochemistry results.15-19 Moreover, although the majority of KA cases follow a self-limiting course and resolve spontaneously within a few months, certain cases may exhibit aggressive growth patterns or anomalous clinical behaviors. Clinicians should remain vigilant for the potential of malignant transformation in cases of KA displaying atypical growth characteristics.14,20,21 Some literature reports suggest that long-standing non-healing KA may progress to or coexist with SCC. 7 Therefore, in cases of skin nodules with ambiguous diagnoses, particularly in pediatric patients, prompt excision and thorough pathological examination are advised to prevent misdiagnosis and treatment delays.
The treatment modalities for KA encompass a range of options, including surgical resection, electrocautery and curettage, cryotherapy, topical drug therapy, radiation therapy, photodynamic therapy, systemic therapy, and immunotherapy. 22 Surgical excision stands as the preferred method, particularly in cases where the differential diagnosis is uncertain or the tumor demonstrates rapid growth. Surgery not only ensures complete removal of the affected tissue but also facilitates adequate sampling for pathological evaluation to confirm the tumor’s nature and exclude malignancy. 19 In the presented case, the patient underwent total excision of the upper lip lesion, with subsequent postoperative pathological assessment confirming keratinizing acanthoma. No recurrence was observed during the follow-up period, underscoring the efficacy of surgical resection in managing KA in children. Electrocautery, curettage, and cryotherapy are suitable for small or superficial lesions; topical drug therapy and photodynamic therapy are beneficial for patients in the early stages or with significant cosmetic concerns; radiation therapy is indicated for inoperable patients or those with multiple lesions; and systemic therapy and immunotherapy are employed for extensive or treatment-resistant KA. 23 When selecting surgical interventions for pediatric patients, considerations should include cosmetic outcomes and functional restoration. The regenerative potential of children’s skin often leads to favorable healing results; however, surgical planning must prioritize minimizing the risk of postoperative scarring and functional impairment, particularly in procedures involving the face or other exposed areas. Postoperative surveillance is crucial to detect potential recurrences or complications, necessitating regular clinical assessments and imaging evaluations.
While KA generally exhibits a favorable prognosis, long-term prognostic information in pediatric patients is currently scarce. Existing literature indicates that patients with KA who undergo surgical excision experience lower recurrence rates, particularly when the lesion is completely resected. 14 Given the limited number of pediatric cases and the constraints on follow-up duration, additional case data are required to comprehensively delineate the prognostic features of KA in children.
Certain studies propose that KA may exhibit a more intricate clinical trajectory under particular conditions, such as recurrent relapses or concurrent immunosuppressive conditions. 24 Hence, in pediatric patients with KA, particularly those with underlying immunodeficiency or systemic illnesses, enhanced long-term monitoring is recommended. This should be coupled with imaging studies and other adjunct diagnostic modalities as needed to promptly identify and address the potential risks of recurrence or transformation.
Future investigations concerning KA in the pediatric population should center on its pathogenesis, molecular pathological characteristics, and long-term prognosis. Genomic and molecular biology inquiries hold promise for identifying distinct molecular markers linked to KA pathogenesis, potentially yielding novel avenues for early detection and personalized therapeutic approaches. Furthermore, the aggregation of comprehensive KA case data in children via multi-center collaborative research endeavors can facilitate the development of more comprehensive diagnostic and treatment protocols, ultimately enhancing diagnostic precision and therapeutic outcomes in clinical settings.
In summary, this article underscores the significance of prompt diagnosis, surgical resection, and sustained monitoring in managing KA in pediatric patients, as elucidated through an in-depth examination of a rare case involving KA on the upper lip in a child. Despite the infrequent and atypical occurrence of KA in children, the diagnostic and therapeutic approaches for pediatric KA necessitate consideration of the pathological characteristics, clinical presentations, and treatment modalities to optimize treatment outcomes and ensure long-term prognostic success.
Footnotes
Author Contributions
J.W.: conception and design of the study, acquisition of data, data analysis, and interpretation, drafting of the manuscript and critical revision, approval of final version of the manuscript. Y.Q.: conception and design of the study, acquisition of data, data analysis, and interpretation, drafting of the manuscript and critical revision, approval of final version of manuscript. F.W.: acquisition of data. X.Y.: drafting of the manuscript and critical revision, approval of final version of the manuscript. C.Z.: drafting of the manuscript and critical revision, approval of final version of the manuscript.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Statement
The studies involving human participants were reviewed and approved by the ethics committee of Qingdao Women and Children’s Hospital.
Informed Consent
The patient’s legal guardian provided written informed consent to participate in this study.