
Abstract
Pilomatricomas are benign skin tumors often encountered by otolaryngologists but frequently misdiagnosed. Although they can occur at any age, they commonly present in children as a discolored superficial lesion adhered to the overlying skin. Accurate preoperative diagnosis is crucial for appropriate management, which is surgical in most cases. Here, we present bilateral pilomatricomas mimicking features of several other diagnoses in a pediatric patient. The patient was successfully treated with surgical excision. This case presented a unique diagnostic challenge, as the lesions exhibited features of several common diagnoses. In general, surgical management of pilomatricoma is curative, and recurrence is rare.
Introduction
Pilomatricomas are the third most commonly excised superficial lesions of the head and neck, following epidermoid cysts and lymph nodes. Nonetheless, they are frequently misdiagnosed by clinicians, with some studies reporting a preoperative diagnostic accuracy of less than 30%.1,2 This could be partially explained by physician unfamiliarity with the lesion. Pilomatricomas were first described by Malherbe and Chenantais in 1880 using the term “calcifying epitheliomas.”3,4 After several changes in nomenclature, Forbis and Helwig refined the term to pilomatrixoma, which more accurately described the masses as benign ectodermal tumors arising from the germinal matrix center of hair follicles. 5 More recently, authors have begun to use the term pilomatricoma.6,7 Despite a growing understanding of the pathophysiology of this entity, clinical recognition of pilomatricoma remains poor among practitioners of all specialties, including pediatric otolaryngology.
Pilomatricomas have a propensity to mimic other lesions such as hemangiomas or branchial cleft cysts, which could explain preoperative diagnostic inaccuracy. Accurate preoperative diagnosis, while difficult, is crucial for planning the correct surgery that is safe and minimizes the chances of recurrence. Thus, familiarity with pilomatricoma is needed among pediatric otolaryngologists. We present here a lesion whose location and clinical appearance mimicked other common entities, leading to a complicated diagnosis and workup. Treatment was successful surgical excision, and the patient recovered well.
Case Presentation
A 9-year-old female presented to our clinic with a 1-year history of bilateral, nontender, slowly enlarging neck masses. She denied any drainage from the masses. She was otherwise healthy and denied any fevers, chills, night sweats, or weight loss. She had no significant past medical history or family history of cancer. On physical examination, an oblong, mobile 2 × 3 cm left neck mass was found posteroinferior to the auricle (Figure 1). On the right, a similar subcentimeter mass was found just posterior to the angle of the mandible with less prominent overlying skin discoloration. Both masses demonstrated apparent central puncta and overlying blue-red skin discoloration. There was no lymphadenopathy. Ultrasonography of the left neck revealed a heterogeneous mass with significant vascularity favoring a diagnosis of hemangioma. This complicated further workup by precluding the possibility of obtaining fine-needle aspiration (FNA) due to the lesion’s vascularity and risk of hemorrhage. Magnetic resonance imaging (MRI) showed both masses as intimately associated with the underlying parotid tissue, but no definitive invasion was seen. These findings, in conjunction with the overlying punctum suggesting a fistula or sinus tract, were concerning for branchial cleft cyst.

Left neck mass: Irregular neck mass found just inferior and posterior to left auricle. Note overlying skin discoloration with what appears to be a central punctum.
Differential diagnosis included hemangioma, branchial cleft cyst, dermoid cyst, epidermoid cyst, vascular malformation, and pilomatricoma. The patient was taken to the operating room for successful left neck mass excision. The apparent punctum was explored intraoperatively, and there was no evidence of subcutaneous tract, sinus, or fistula. The surgical specimen consisted of skin ellipse overlying a well circumscribed subcutaneous mass (1.9 × 1.5 × 1.1 cm) with a gray-white, granular, cheesy-like cut surface. Histopathology showed islands of solid blue areas composed of basaloid cells encircling eosinophilic areas of “ghost cells” with abundant eosinophilic cytoplasm and faint cellular outlines. Focal areas of dystrophic calcification with a foreign body-type giant cell reaction were also noted (Figure 2). Final diagnosis was pilomatricoma. The patient was seen in clinic 1 week postoperatively, where the surgical site was found to be healing appropriately. At her own convenience, she plans to pursue future excision of the smaller mass on the right side, which is likely also a pilomatricoma.
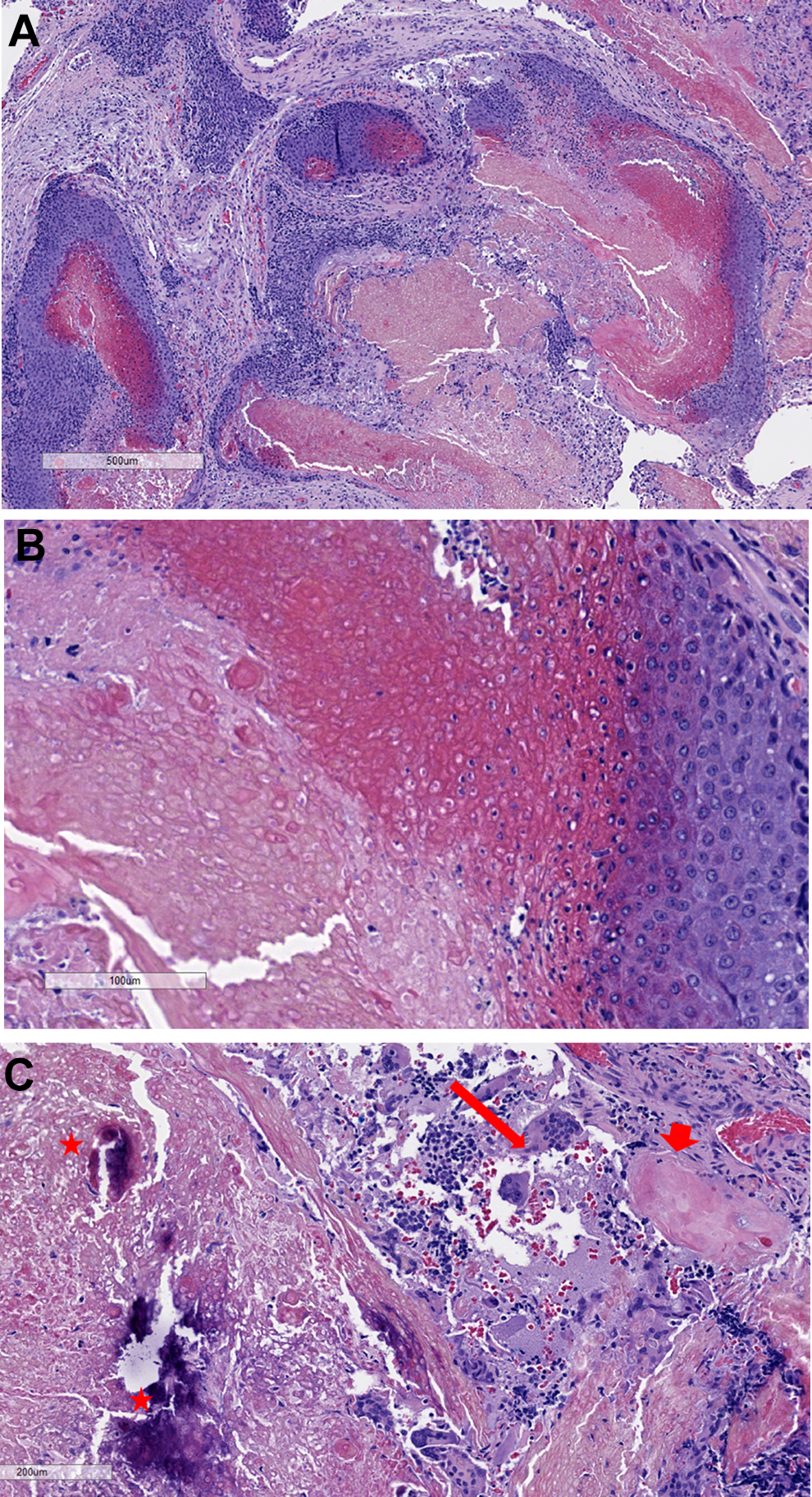
Histopathology slides: (A) islands of solid blue areas composed of basaloid cells, encircling eosinophilic areas of “ghost cells” (H&E, ×40). (B) Higher magnification showing basaloid cells with scant cytoplasm, round nuclei, encircling ghost cells with abundant eosinophilic cytoplasm and faint cellular outlines (H&E, ×200). (C) Most of the tumor is composed of eosinophilic keratinous debris (short arrowheads), with focal areas of dystrophic calcification (stars) and a foreign body-type giant cell reaction (long arrow) to keratin and ghost cells (H&E, ×100).
Discussion
Pilomatricoma (formerly known as pilomatrixoma) is a benign tumor of the hair follicle matrix which often presents in the pediatric population.1,7 In one large review study by Yencha, approximately 45% arose before 21 years of age. 8 Another study showed that 60% arose within the first 2 decades of life with the highest incidence in children between the ages of 8 and 13 years. 9 The incidence of multiple pilomatricomas arising in the same patient has been reported to be 3.5%. 9 There is a female preponderance, and most cases arise in Caucasian patients. 1
Over 50% of pilomatricomas occur in the head and neck region, thus knowledge of these lesions is particularly salient for otolaryngologists.7,10 Within the head and neck, pilomatricomas are most commonly found on the neck, the cheek, and the preauricular region. Lesions classically present as superficial, rock-hard masses with overlying bluish or reddish discoloration or ulceration. 10 Most are less than 3 cm in diameter. They are well-circumscribed masses that may be adhered to the overlying skin, but they ought to move freely from underlying soft tissue structures. The “tent sign” was described by Graham and Merwin in 1978 and involves stretching the overlying skin so that the irregularity of the lesion and multiple angles and facets can be palpated. 11 This sign has been said to be pathognomonic for pilomatricoma. 10 The “teeter-totter sign” involves pressing one edge of the lesion, which displaces the opposite edge through the skin like a teeter-totter. The teeter-totter sign and the tent sign are the most helpful physical examination findings for diagnosis of pilomatricoma. 10
Unfortunately, pilomatricomas are frequently misdiagnosed. Although this case exhibited characteristics which were classic for pilomatricoma, it was necessary to first rule out several other differential diagnoses. First branchial cleft cyst was high on the differential diagnosis given the location of the lesions just inferior to the auricle and the presence of an apparent punctum, which was concerning for an associated sinus tract or fistula. However, branchial cleft cysts are unlikely to exhibit vascularity, and they are not typically associated with skin discoloration unless infected, making it a less likely diagnosis in this case. 12 Late-onset infantile hemangioma has been demonstrated in children up to 8 years of age. 13 It was considered as a possible diagnosis in this case, especially given the radiologic signs of significant vascularity. However, late-onset infantile hemangiomas are exceedingly rare, and pilomatricoma also can be highly vascular. 14 Epidermoid cyst (also known as epidermal inclusion cyst, epidermal cyst, and sebaceous cyst) could not be definitively ruled out preoperatively, especially given the overlying “puncta.” However, epidermoid cysts typically grow within the first few years of life, are unlikely to exhibit late growth patterns and do not typically have an overlying skin hue. 12 In addition, the lesion in this case was found not to have a true punctum on intraoperative exploration. Pilomatricomas are known to create a punctum-like appearance due to overlying skin tethering, 10 which complicated diagnosis in this case. Other masses that should be included on the differential diagnosis for pilomatricoma include lipoma, foreign body reaction, degenerating fibroxanthoma, osteoma cutis, and ossifying hematoma. 10
Some authors assert that radiologic imaging of pilomatricoma has “little diagnostic value” given the superficial location.10,15 Others advocate for computed tomography or MRI in masses overlying the parotid gland to help distinguish boundaries of the lesion relative to the gland. On ultrasound, they present as well-defined, hyperechoic or isoechoic nodules with a hypoechoic rim and posterior shadowing. Computed tomography shows a well-defined mass of soft tissue density with mild to moderate enhancement with contrast. There may be intralesional calcific foci. Magnetic resonance imaging findings are inconsistent but tend to show a mass with homogenous, intermediate signal intensity on T1-weighted imaging and heterogenous, intermediate signal intensity on T2-weighted imaging. A retrospective study by Kato et al found that pilomatricomas commonly display reticular and ring-like enhancement on fat-suppressed gadolinium-enhanced T1-weighted images, whereas fat-suppressed T2-weighted imaging may show reticular and ring-like hyperintensities. 16
Grossly, the tumor is well-circumscribed with a cheesy, yellow-white cut surface and a gritty consistency secondary to calcification. 17 Histological examination reveals well-demarcated dermal nodules surrounded by a capsule of compressed fibrous tissue located in the lower dermis and extending into the subcutaneous fat. The tumor cells form well-organized islands arranged in a circular configuration with nucleated basophilic cells on the periphery and the characteristic anucleated shadow or “ghost cells” in the center. These islands are associated with a foreign body-type giant cell reaction to the keratinous debris and ghost cells.7,17,18 Dystrophic calcification can be found in 69% of tumors. 9 Although FNA may be helpful in preoperative diagnosis, the absence of ghost cells in the aspirate is common and may lead to misdiagnosis.10,15
The natural history of pilomatricoma is continued growth or persistence of lesion—spontaneous regression has never been reported. 7 Standard treatment is wide local excision with at least 1 to 2 cm margins with malignant variants, as there have been rare cases of metastatic pilomatrix carcinoma.7,19 Surgical excision is curative, and recurrence is rare, with rates reported by some authors between 0% and 3%.3,8,10,14,15,20 Multiple recurrences following excision suggests a higher likelihood of malignant transformation. 7 Thus, clinicians regularly taking care of pediatric patients ought to be aware of this commonly misdiagnosed lesion to ensure accurate diagnosis and appropriate intervention.
Conclusion
Despite occasionally being thought of as a trivial diagnosis, pilomatricoma has the potential to present a significant diagnostic challenge. Although the diagnosis is ultimately made by our pathology colleagues, increasing familiarity with these lesions among pediatric otolaryngologists is important for accurate preoperative diagnosis. This case illustrates a classic dilemma that any clinician may encounter when diagnosing pediatric neck masses. Prompt diagnosis and recognition is key to proper preoperative planning and safe surgical management.
Footnotes
Authors’ Note
This manuscript has not been published and is not under consideration elsewhere. N. A. Rossi, R. Gietzen, C. G. Clement, H. S. Pine, W. Szeremeta, and S. Daram contributed to drafting and editing of manuscript. H.S. Pine, B. J. McKinnon, W. Szeremeta, and S. Daram contributed to concept, guidance, and review of manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.