
Abstract
Keywords
Introduction
Rhinoplasty is a complex surgical procedure encompassing both functional and aesthetic aspects. At the core of rhinoplasty is the nasal tip, a sophisticated anatomical feature. Tip plasty plays a crucial role in achieving balanced facial proportions while ensuring nasal functionality. 1 The interaction among lower lateral cartilages, septal cartilage, adjacent soft tissues, tissue dynamics, and surgical techniques determines the nasal tip’s projection, rotation, and overall shape. 2 Surgeons utilize various grafting methods to achieve the desired projection and stability, providing essential support for the nasal tip. 3 Over time, these techniques have advanced, offering enhanced control and predictability. However, understanding their long-term impact on nasal tip support and stability remains an ongoing process.
The columellar strut graft, first introduced in 1932, 4 has became a widely adopted technique. Typically a rectangular cartilage piece is positioned between the medial crura to provide support and stability to the nasal tip. On the other hand, septal extension grafts extend from the caudal edge of the nasal septum into the lower lateral cartilages, these grafts offer crucial structural support to the nasal tip. To regulate and maintain tip projection, rotation, and the transition from the tip to the dorsum. 5 However, these techniques, while effective and reliable when properly placed, have their limitations. Columellar struts may undergo resorption and displacement, due to their lack of attachment to the caudal septum, and primarily resting between the alar cartilages, resulting in postoperative tip drooping. This positioning limits their efficacy in rotating the tip or altering the nasal angle. 6 Furthermore, septal extension grafts may, in some cases, require additional cartilage, such as conchal or costal cartilage, particularly when the available septal cartilage is insufficient. However, this requirement depends on individual patient anatomy and surgical planning. 6 In rhinoplasty, the choice between columellar strut and septal extension graft largely depends on the surgeon’s preference, as both methods are reported to effectively control the tip and enhance nasal tip projection and rotation. 3
Although these grafting techniques are widely used, existing comparative studies on their long-term effects, particularly on nasal tip stability, are still limited. Prior studies, such as those by Bellamy and Rohrich, 2 Sadeghi et al, 7 and Sazgar et al, 8 have explored the effectiveness of columellar strut and septal extension grafts in maintaining nasal tip stability. However, this study aims to build on these findings by providing a more detailed comparison of the long-term effects of these grafts on nasal projection and rotation. The insights gained from this study will aid surgeons in selecting the most appropriate graft technique to optimize surgical outcomes.
Methods
This retrospective analytic cohort study was conducted at King Saud University Medical City in Riyadh, Saudi Arabia. Involving patients who underwent primary rhinoplasty for nasal tip modification between March 2021 and March 2022. Patients were divided into 2 groups, receiving either a columellar strut graft or a septal extension graft. Both surgical techniques were carefully standardized to maintain consistency in other aspects of the procedure, ensuring that any observed differences in outcomes could be attributed to the grafting technique itself. To ensure the integrity of the study, patients with a history of previous nasal surgery, trauma, chronic diseases affecting wound healing, or incomplete medical and photographic records were excluded.
Sample Size Calculation
Rhinoplasty cases performed by the senior author (B.D.) from March 2021 to March 2022 were reviewed. Of the 292 cases initially identified, 240 were selected for inclusion based on their involvement in either columellar strut grafts or septal extension grafts. This sample constituted approximately 82.2% of the total cases operated on during this period.
Surgical Technique
In this study, rhinoplasty was performed on all patients by the senior author (B.D.) to ensure consistency. The operations were conducted under a combination of general anesthesia and targeted local anesthetic infiltration. The surgical process commenced with a transcolumellar incision, providing access to the internal nasal structures for precise manipulation and graft placement. Following dorsal osteocartilaginous hump reduction, the required grafts were harvested from the septal cartilage. Each patient underwent a cephalic trim of the alar cartilage and received a tip graft. The only variation in the surgical approach was the type of graft used, for group 1, the columellar strut graft technique was employed, with the graft inserted into a web created between the medial crura and secured with sutures (Figure 1). In group 2, the septal extension graft technique was used, with the graft placed into the caudal septum and secured using the tongue-in-groove technique. In this approach, both the medial and middle crura were sutured to the caudal septum to enhance rotational stability and ensure proper positioning of the nasal tip (Figure 2). The grafts in both groups served multiple purposes, including providing support, projection, and rotation to the nasal tip.
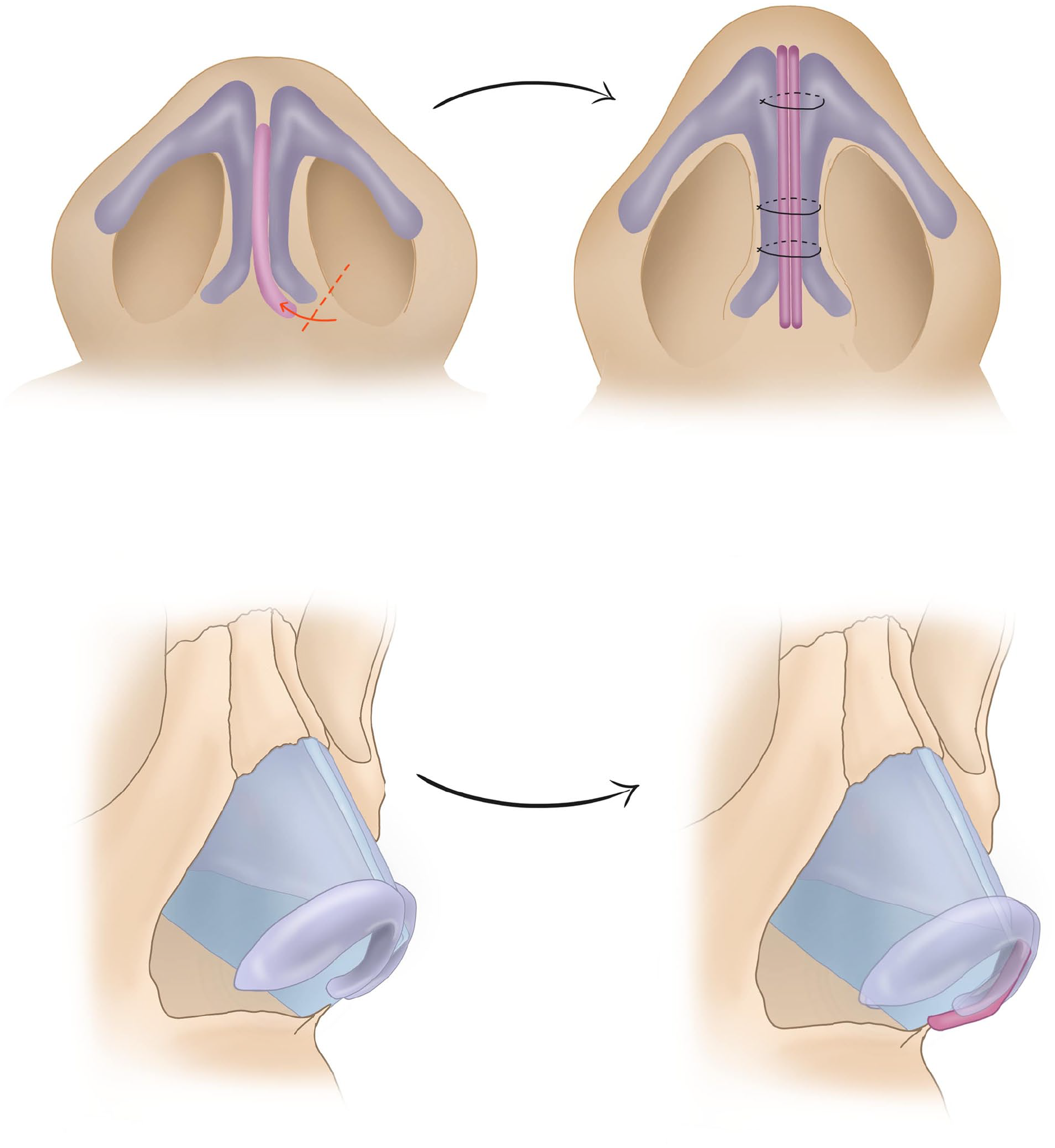
Columellar strut graft technique.
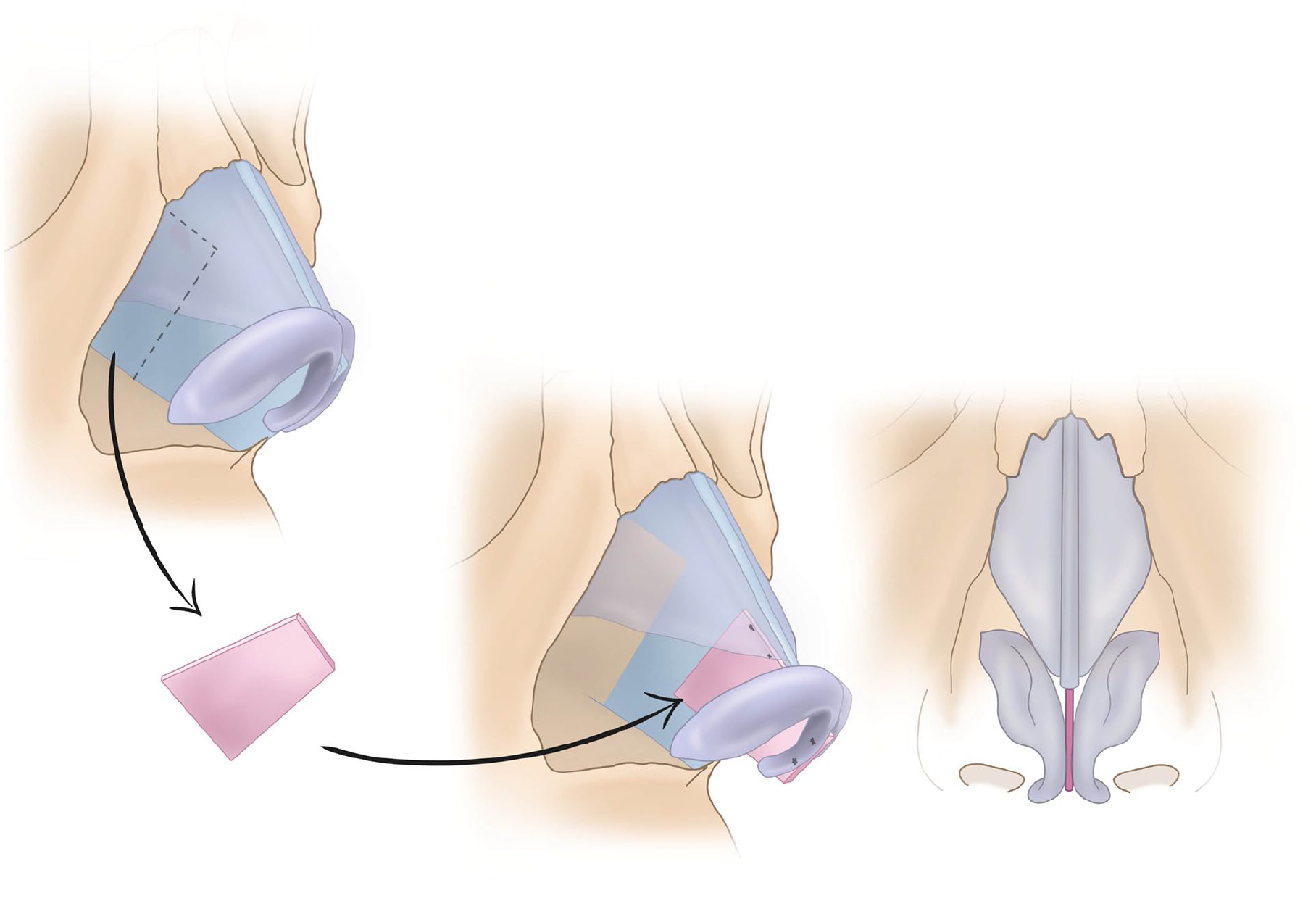
Septal extension graft technique.
Data Collection Protocol
A meticulous data collection protocol was established, wherein preoperative standardized photographs were taken in a controlled setting. This protocol ensured uniform lighting, background, and camera settings across all photographs, which included frontal, lateral, and basal views. These photographs served as the baseline for subsequent comparative analysis. Follow-up photographs taken at 6 and 18 months postoperatively adhered to the same standards, facilitating assessments of nasal tip projection and rotation.
Assessment Parameters
Primary outcomes included nasal tip projection and rotation stability, measured at 6 and 18 months postoperatively with photographic analysis. Secondary outcomes encompassed patient satisfaction, assessed using a validated Rhinoplasty outcome evaluation (ROE) questionnaire, as well as the incidence of postoperative complications such as infection, graft displacement, and the need for revision surgery.
Photographic Analysis
Photographic analysis was conducted using Rhinobase software to ensure standardized documentation of nasal tip projection and rotation. This software allowed for consistent and objective measurements that were independent of the individual performing the analysis, minimizing variability. Manual measurements using digital calipers were also performed as a secondary check, and we found that the results from Rhinobase closely matched those obtained through manual methods.
Statistical Analysis
The data analysis was conducted using SPSS software version 29. The primary focus of our analysis centered on evaluating the changes in nasal tip projection and rotation associated with columellar strut grafts and septal extension grafts over a period of 18 months. To assess tip projection, we conducted independent t-tests to compare the mean measurements at 3 pivotal time points: preoperatively (Time 0), 6 months postoperatively (Time 1), and 18 months postoperatively (Time 2) for each group. This analysis involved a detailed examination of the significance of changes from Time 0 to Time 1, and subsequently from Time 1 to Time 2, with an emphasis on the percentage changes in tip projection. The calculated P-values were instrumental in determining the statistical significance of these alterations, adopting a threshold of P < .05 to denote significance. Furthermore, for tip rotation, as assessed by variations in the nasolabial angle, paired sample t-tests were utilized to compare the angles at each time point within the respective groups. This part of the analysis was especially focused on the percentage change in the nasolabial angle from Time 1 to Time 2, aiming to identify any notable long-term changes in tip rotation. A comparative analysis was also performed to elucidate the relative effectiveness of both surgical techniques in maintaining tip projection and rotation over the time span of the study.
Ethical Considerations
This research was approved by the institutional review board at King Saud University Medical City. Strict confidentiality of patient data was maintained throughout the study. Due to its retrospective design, specific consent for this analysis was not required. Nevertheless, all patients had previously consented to the use of their medical records and photographs for research and educational purposes at the time of their surgery.
Results
The records of 240 patients were reviewed in this study. Among them, 120 patients received columellar strut graft (group 1), whereas 120 patients received a septal extension graft (group 2). All patients in the study were female. The average age was 25.2 ± 5 years in columellar strut grafts group and 25.8 ± 5.5 years in septal extension grafts group. The study centered on the changes in nasal tip projection and rotation at 3 pivotal time points: preoperative (Time 0), 6 months postoperative (Time 1), and 18 months postoperative (Time 2).
Tip Projection Analysis
When the Time 1 results were compared with the preoperative values (Time 0) in the columellar strut grafts group, a significant immediate postoperative improvement in tip projection increased from 32.3 ± 3.1 to 35.7 ± 7.3 mm. Similarly, the septal extension grafts group demonstrates improvement in tip projection, from 31.2 ± 4.1 to 33.8 ± 6.4 mm increased in nasal tip projection. However, in the long term, both techniques showed a slight regression in Time 2, the decrease in columellar strut grafts group was 35.1 ± 7.3 mm, indicating relatively stable results. The −1.7% change is not statistically significant (P = .69). As well in Time 2 of the septal extension grafts group tip projection decreased to 33.0 ± 5.9 mm, a slightly more pronounced reduction (−2.2%) than in the columellar strut grafts group, though this change is also not statistically significant (P = .50), indicating the initial improvements are largely maintained in both techniques.
Tip Rotation Analysis (Nasolabial Angle)
The mean nasolabial angle in the columellar strut grafts group increases from 107.3 ± 17.3 degrees (Time 0) to 118.5 ± 10.4 degrees (Time 1), then decreases to 112.5 ± 11.0 degrees (Time 2). The change (−5.08%) is statistically significant (P = .009), indicating a notable but not drastic reduction in the improved nasolabial angle over the long term (Time 1-Time 2). On the other hand, the septal extension grafts group demonstrates a −1.01% reduction in the improved nasolabial angle over the long term (Time 1-Time 2), which is not statistically significant (P = .64). This suggests a more stable outcome in terms of the nasolabial angle compared to the columellar strut group.
Patient Satisfaction Using ROE
The ROE questionnaire was used to assess patient satisfaction at multiple postoperative intervals, with a maximum score of 24 indicating higher satisfaction. Both the columellar strut and septal extension graft groups demonstrated high initial satisfaction, with average scores of 21 and 22, respectively. Over time, the septal extension graft group maintained more consistent satisfaction levels, with stable ROE scores at the 18-month follow-up. In contrast, the columellar strut group experienced a slight decline in satisfaction, particularly in terms of nasal tip rotation stability by the 18-month mark.
Incidence of Postoperative Complications and Revision Surgery Rates
The incidence of common postoperative complications such as infection and graft displacement was negligible in both groups. However, revision surgery rates were tracked as an indicator of surgical success and patient satisfaction. In group 1, the revision surgery rate was 5%, while in group 2, it was 4.167%. These percentages indicate a minor variation in the need for additional surgical interventions between the techniques. Analyzing the difference in revision surgery rates between the 2 groups for statistical significance did not reveal a notable distinction, suggesting comparable likelihoods of requiring revision surgery for both surgical techniques.
Discussion
The present study meticulously compared the nasal tip stability following rhinoplasty between 2 techniques, columellar strut grafts, and septal extension grafts. The focus was on assessing their effectiveness in maintaining nasal tip projection and rotation over time.
Nasal tip plasty is among the most important and crucial aspects of rhinoplasty, playing a vital role both functionally and aesthetically. 9 It is influenced by the surgical approach, techniques, and postoperative healing. 3 Effective control of nasal tip projection and rotation are key components for achieving aesthetically pleasing and functional nasal tips. Several techniques have been described in the literature for effectively enhancing and altering nasal tip projection and rotation. 1 Among these, columellar strut grafts and septal extension grafts are commonly used in rhinoplasty. The columellar strut graft is placed between the medial crura along the caudal septum down to the anterior nasal spine. Conversely, the septal extension graft is fixed along the caudal septum and placed above the anterior nasal spine. 3 Both techniques are reliable for achieving smooth and predictable rotation and projection of the nasal tip. However, maintaining long-term nasal tip stability is a significant concern in rhinoplasty for both the surgeon and the patient.
In our study, both columellar strut and septal extension graft techniques are effective in altering nasal tip projection, with stable long-term outcomes. However, in terms of tip rotation, the columellar strut group exhibits a significant initial increase followed by a slight regression, while the septal extension graft group maintains more consistent results over time. These findings suggest that the columellar strut technique may be more suitable for patients seeking a more significant alteration in tip rotation, whereas the septal extension graft may be preferable for those seeking stable, long-term outcomes with minimal change in tip rotation. Our results distinctly favor septal extension grafts due to their enhanced ability to sustain postoperative outcomes. These findings are consistent with those of similar studies. A retrospective cohort study using 3-dimensional photogrammetric evaluation compared columellar strut grafts and septal extension grafts over a 12-month period. Both groups showed a decrease in nasal tip projection and rotation over time, but the reduction in tip projection was not statistically significant between the 2 techniques. However, septal extension grafts demonstrated better long-term maintenance of tip rotation. 3 Our results also align with Bellamy and Rohrich et al 2 who reported that septal extension grafts provide superior long-term nasal tip stability compared to columellar strut grafts. In their retrospective review, the septal extension graft group experienced only a 0.2% loss in nasal projection at 1 year, compared to a significant 4.7% loss in the columellar strut group. Additionally, the mean rotation loss was 1.3 degrees in the septal extension group, compared to 4.9 degrees in the columellar strut group. Similarly, Sadeghi et al, 7 found that septal extension grafts offered better control over tip rotation with greater long-term stability. Sazgar et al 8 confirmed these findings, demonstrating that septal extension grafts showed better maintenance of both projection and rotation compared to columellar struts. Collectively, these studies highlight a growing consensus that septal extension grafts are more effective for ensuring sustained postoperative outcomes in rhinoplasty, particularly in maintaining nasal tip projection and rotation.
Akkus et al. compared nasal projection using columellar grafts versus septal extension grafts, both grafts showed an increase in nasal projection postoperatively, which decreased over time. However, this decrease was less and more stable in patients who received septal extension grafts. 10 Moreover, In a randomized controlled trial conducted by Arda Kucukguven, septal extension grafts provided better tip projection and rotation stability compared to the columellar strut grafts. 11 This alignment with existing studies not only strengthens the credibility of our results but also emphasizes a growing consensus within the surgical community regarding the optimal choice of grafts for lasting outcomes in rhinoplasty. The initial nasal appearance following rhinoplasty is anticipated to undergo change over time due to different factors such as graft shrinkage, resorption, or displacement. 10 The septal extension graft technique demonstrates a more stabilized nasal tip position compared to the columellar strut graft technique. This advantage of septal extension grafts is primarily attributed to their structural characteristics by being larger and stronger, they offer more robust support to the nasal tip. This support is likely a key factor in preventing the nasal tip from drooping over time. Furthermore, septal extension grafts exhibit a lower propensity for contraction compared to columellar strut grafts. Contraction, where the graft shrinks over time and potentially alters surgical results, is a significant concern in rhinoplasty. The composition of septal extension grafts, including thicker and stronger cartilage, appears to significantly reduce the risk of nasal tip drooping, thus preserving tip projection and rotation more effectively. Although the use of thicker cartilage in septal extension grafts may provide strong structural support, there is a potential for subtle asymmetry in some cases. With careful surgical technique and precise graft placement, this risk can be minimized.
In the columellar strut technique, the floating cartilage is placed in a pocket between the medial crura, which is not directly fixed to the septum or base structure, 3 In contrast, the septal extension graft is firmly sutured to the caudal septum, anatomically fixed to the nasal spine, providing a secure point of attachment for the medial crura and domes. 3 Biomechanical tests demonstrate that the cartilaginous septum compared to other nasal cartilages possesses the greatest intrinsic strength, serving as an effective supporting structure. Nasal tip support is thought to be influenced by several factors, with the caudal septum playing an important role. Other structures, such as the nasal ligaments, may also contribute to maintaining long-term tip stability. Ensuring proper support from these elements is crucial to achieving favorable surgical outcomes. Therefore, reinforcing and addressing the caudal septum should be a core component in tip plasty.12 -14
The objective measures of a successful rhinoplasty, despite their accuracy, often overlook patient satisfaction—a pivotal determinant of rhinoplasty success or failure. In our study, we employed The ROE questionnaire, an easy-to-apply tool for a reliable and standardized assessment of post-rhinoplasty quality of life. It assesses qualitative aspects such as emotional, social, and psychological factors. 15 For both techniques—columellar strut grafts and septal extension grafts—the average ROE scores were 21 and 22, respectively, indicating a high level of satisfaction both aesthetically and functionally, with no statistically significant difference between the 2 techniques. The revision surgery rates were monitored as indicators of surgical success and patient satisfaction. In the columellar strut grafts group, the revision surgery rate was 5%, while in the septal extension grafts group, it was slightly lower at 4.167%. The similarity in revision surgery rates, despite a minor numerical difference, does not signify a significant variance. This suggests parallel levels of effectiveness and patient contentment with both columellar strut grafts and septal extension grafts.
In this study, all cases were performed by the same experienced surgeon, ensuring consistency in the surgical technique, measured outcomes, and duration of follow-up, with an assessment of patients’ satisfaction. Nevertheless, it has some limitations, being confined to a female population, which may affect the generalizability of the findings. Gender differences in skin thickness, cartilage structure, and healing patterns could influence nasal tip support and projection outcomes. Another limitation is being a single-center study. Although skin thickness is a crucial factor influencing nasal tip projection and support, this study did not categorize patients based on skin thickness. Variations in skin thickness may affect the long-term stability of grafts and surgical outcomes. Future studies should include skin thickness as a variable to further understand its impact on rhinoplasty outcomes and ensure more personalized surgical planning. However, to the authors’ knowledge, this is the only study that subjectively compared columellar strut grafts and septal extension grafts techniques through photographic analysis and assessed patients’ satisfaction using ROE scores and revision rates. The authors of this study recommend further research with a larger, more diverse sample size, encompassing both genders and with an extended follow-up duration, to facilitate clinical decision-making and guide the selection of the most appropriate technique.
Conclusion
Both grafting techniques exhibited an initial increase in tip projection from preoperative measurements to early postoperative results, followed by a slight regression at later stages. However, this change was not statistically significant for either group, indicating that both grafting methods can ensure stable tip projection in rhinoplasty. A clear difference emerged in tip rotation, measured by the nasolabial angle. The columellar strut group experienced a notable increase in tip rotation initially, followed by a significant decrease, while the septal extension graft group showed minimal and not statistically significant changes in tip rotation over the same period. This suggests that septal extension grafts are more effective in maintaining tip rotation over time. This aspect might influence surgeons’ preferences for grafting techniques, contributing significantly to the overall success of the procedure.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not required.