
Abstract
Background:
Rhinoplasty is one of the most popular procedures in facial plastic surgery. It is a technically demanding surgery with a long learning curve. The outcome may be very beneficial to the function of the nasal breathing as well as the patient’s social life but harbors many pitfalls and sequelae from minor to devastating. This grants a high demand on the knowledge of the nose’s anatomy and the implication of each conducted maneuver or grafting during the surgery both short and long term.
Methods and Results:
In the presented case report, we demonstrate the sequelae of a secondary rhinoplasty case, analyze the outcomes, present the revision surgery in detail, and show the follow-ups. Most negative outcomes of primary rhinoplasty may be led back to the particular techniques applied. Leading causes of revision surgery include loss of tip projection, inverted-V-deformity, axis deviation, dorsal irregularities, internal and external nasal valve collapse, damage to the soft tissue envelope, and many more.
Conclusions:
We believe that through such an illustrative case discussion, we may enhance the skills and critical appraisal of young surgeons in decision-making.
Keywords
Introduction
Septorhinoplasty is considered the most difficult common aesthetic procedure due to the wide variation in the patient’s anatomy and aesthetic desires. Mastering septorhinoplasty is a continuous learning process as each septorhinoplasty presents the surgeon with diversity of anatomy and proportions. This mandates a series of organized correlated surgical maneuvers which are individually tailored to fit the needs of each case.
That’s why decision-making about choosing and applying the right surgical technique is the most challenging problem encountered on the long learning curve of the septorhinoplasty. There are a plenty of techniques that can be used individually according to the case and how comfortable is the surgeon with this technique. Every technique has its benefits and risks. Other than that, the extent and detailed nuances of application of each technique play a crucial role as well. As over- or undertreatment could lead to unpleasant results even if the technique itself is suitable for the case. There is an increased evidence favoring techniques over others for certain deformities. Applying the most suitable technique for each case is a gradual learning process starting with knowing the indication and risks for each technique.
In this case, we enhance this learning process by simulating the whole surgery illustrating why we choose specific technique to address each deformity we encountered. Besides that, we highlighted possible underlying causes, we assume, which led to shortcoming in the previous surgeries.
Case Report
Presentation and Medical History
A 19-year-old female patient presented in our office for second opinion and possible revision surgery. She underwent 2 cosmetic rhinoplasties elsewhere before, one closed and one open approach, 2 and 3 years ago, respectively. Moreover, she’s had repeated postoperative hyaluronic acid (HA) injections to the nasal tip. She had no other medical conditions and she has never smoked.
Clinical examination showed a broad, short nose with pollybeak deformity and loss of tip projection and tip protection. There was poor tip definition and symmetry, a slight deviation of cartilaginous nose and the tip to the patient’s right side, columella retraction, and nostrils asymmetry. The eyebrow-nasal tip line was interrupted and irregular on inspection, irregularities of the dorsum on palpation, and an open roof deformity with a broad dorsum. Furthermore, there was alar pinching on the left side, external and internal valve collapse. The nasal septum was relatively straight with absence of perforation.
Notable, there was significant damage to the thick skin soft tissue envelope (SSTE), with discoloration of the nasal tip and dorsum as well as palpable subcutaneous scarring (Figure 1A-C).
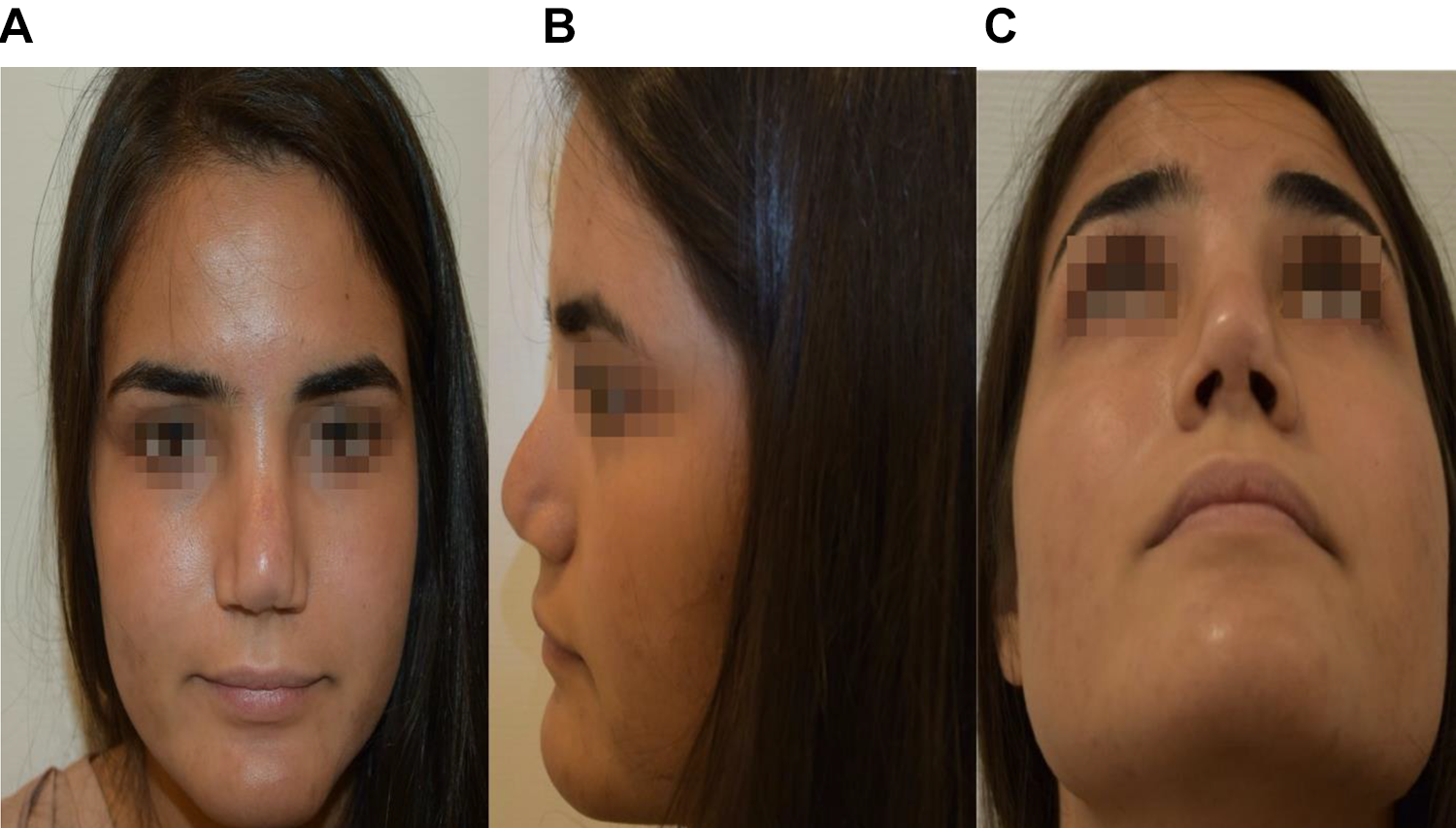
A, Preoperative frontal view shows clover leaf deformity of the tip, effacement of the tip defining points, effacement of the brow tip line on the left side and discontinuity of this line on the right side, too wide middle vault, and too wide Radix. Skin discoloration is seen. B, Preoperative lateral left view shows deprojected tip, short nose, pollybeak deformity over rotated tip, and alar pinching on the left side. C, Preoperative basal view shows clover leaf deformity, tip lobule impression, deviation of the tip to the right side, and nostrils asymmetry.
Presurgical Consultation
We discussed the complexity of the tertiary surgery with the patient and her relatives, the need to harvest rib cartilage to rebuild the nose cartilaginous framework and tip projection and the realistic expectation for aesthetic and functional results. Special emphasis was led on the existing damage and shrinkage of the SSTE and the difficulty to predict the effect of another intervention.
Surgical Procedure
We started the surgery by harvesting a 4 cm part of the cartilaginous right sixth rib through a 3-cm inframammary incision. The cartilage was carved into 1.5 mm oblique slices to sit in saline with gentamicin to anticipate warping during the course of surgery. Furthermore, several cubic centimeteres of macroscopic deep subcutaneous fatty tissue were excised with scissors.
The costal cartilage graft was then cut to form caudal septal extension graft (CSEG), 2 spreader grafts (SGs), a shield graft (SiG), a small butress graft, 2 articulated alar rim grafts (AARG), and diced cartilage.
We chose the open transcolumellar approach with inverted-v-shaped incision using the preexisting scar. The dissection took a place in the plane underneath the superficial muscular aponeurotic system (SMAS). As expected, there was significant scarring and especially in the nasal tip and supratip area, where HA has been injected repeatedly. We continued the dissection of the SSTE over the cartilaginous and bony dorsum cranially to the radix and laterally to the piriform aperture and nasofacial grove. Bony irregularities were smoothened with hand rasp. After injection of local anesthetics, we performed transcutaneous transverse and lateral low–low osteotomies with a 2-mm osteotome to close the open roof deformity. We split the extremely scarred lower lateral cartilages (LLCs) and created an upper bilateral septal tunnel, the upper lateral cartilages were only scarified remnants. The next maneuver was the carving and insertion of bilateral extended SGs from rib cartilage. They were fixed to the septum with 5-0 PDS sutures to achieve symmetry of the middle vault and open the internal nasal valve.

A, One-year postoperative frontal view shows the improvement in the aesthetic dorsal line as well as the improved skin quality and coloration. B, One-year postoperative lateral view shows an improved projection and rotation of the tip, restauration of the profile, and elongation of the nose. C, One-year postopertative basal view shows improvement in the alar base symmetry and light reflexes through better tip definition.
We addressed the deprojected and overrotated tip with a septal extension graft which was sutured end to end to the septal remnant and fixed to the extended SGs on both sides and the anterior nasal spine (Figures 3 and 4). The domes were reconstructed with interdomal and intradomal suturing after moderate lateral crus steal. Furthermore, the lateral crura (LC) were strengthened by the insertion of AARGs which were sutured to the tip (Figure 4a). The nasal tip was still underprojected; therefore, a SiG was used and sutured in place, to secure its position a small buttress graft was sutured behind the SiG (Figures 3 and 4). The pollybeak deformity was caused by abundant soft scar tissue; therefore, a precise but significant SMAS-ectomy and scar-ectomy in the supratip area was done using Stevens scissors. Finally, the harvested fat tissue was minced into 1-mm pieces with scissors and cleaned from debris. It was put as a free transplant on the nasal dorsum and tip area with syringe before wound closure. After closure of all incisions internal and external splinting was used as well as a metal cast. Patient was discharged after uneventful hospital stay after 2 days. Pain medication included nonsteroidal anti-inflammatory drugs and oral opioids as well as broad-spectrum antibiotics for 1 week.
Follow-Up
Regular follow-up at 1, 2, 4 weeks, 6 and 12 months (Figure 2) showed an improved aesthetic result of the patient regarding nasal profile and skin quality. Nasal breathing was found to be better on both sides.
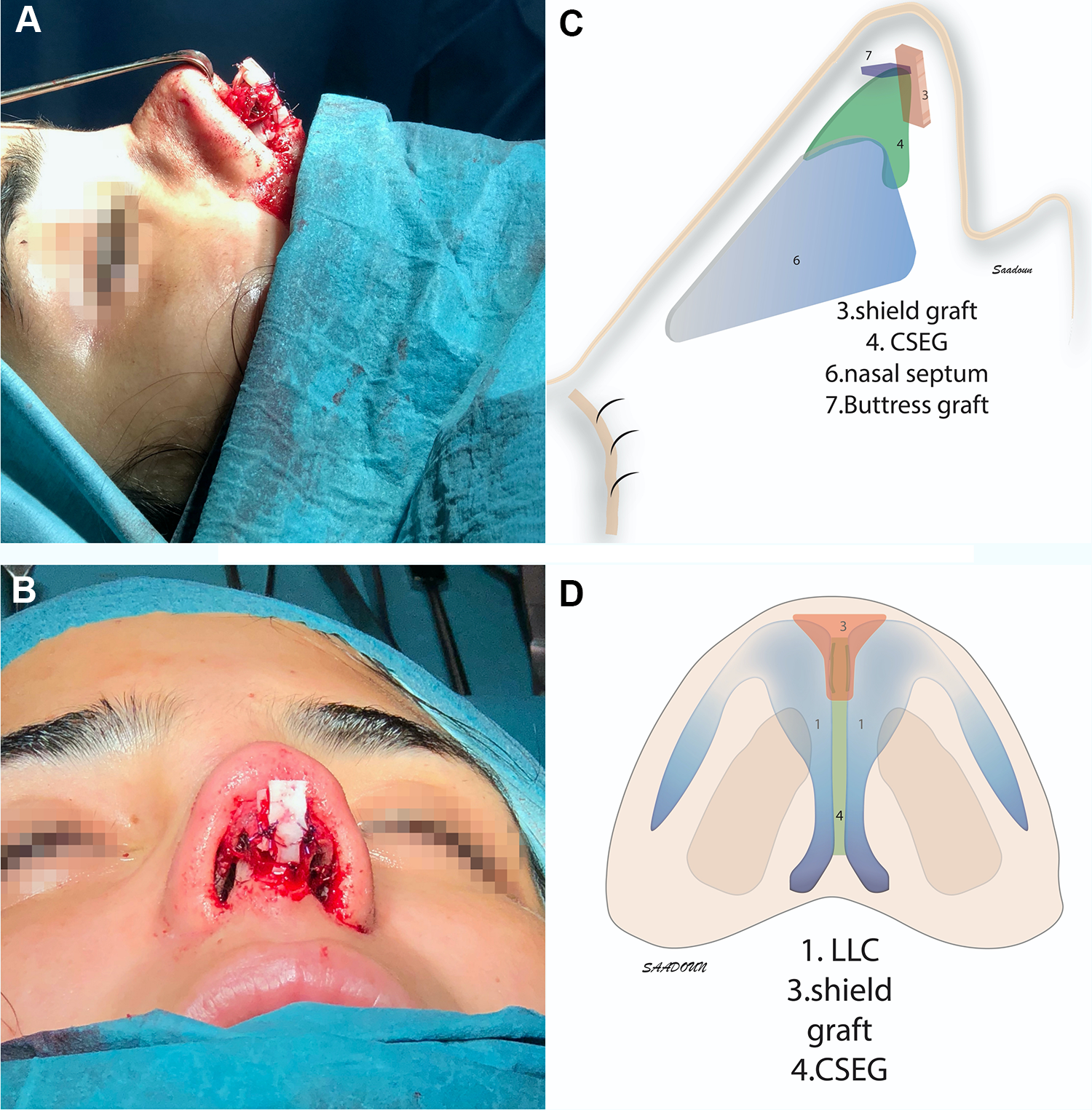
A, Intraoperative lateral view of the shield graft (SiG) and buttress grafts. B, The SiG from the basal view. C, Schematic depiction of the caudal septal extension graft (CSEG), SiG, and buttress grafts from the lateral view. D, Schematic depiction of the SiG and CSEG from the basal view.
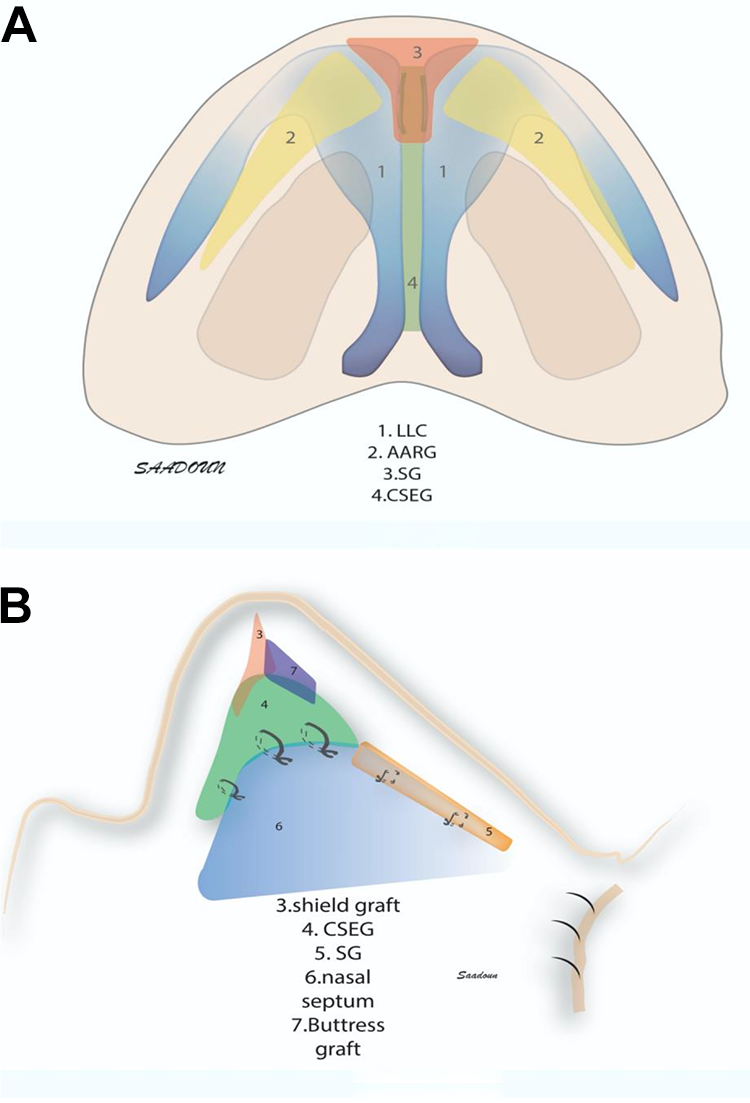
A, Schematic depiction of the applied method from the basal view shows the shield graft (SiG), caudal septal extension graft (CSEG), articulated alar rim grafts (AARG), and lower lateral cartilage (LLC). B, Schematic depiction of the applied method from the lateral view shows the SiG, CSEG, SG, buttress graft, and nasal septal cartilage.
Discussion
Outcomes of primary and revision rhinoplasty may vary significantly, even in the hand of the same surgeon. There is a great variety of possible techniques and variations available, each harboring chances and pitfalls. In the following, we are going to discuss the pre- and intraoperative findings of the presented case, their possible causes and the applied surgical (salvage) techniques.
In the preoperative consultation, we discussed the necessity of rib cartilage harvesting due to the depletion of the septal cartilage after 2 previous rhinoplasties with the patient. According to the findings of the physical examination, we were anticipating the need for significant structural grafting, such as 2 SG, 1 CSEG, 2 AARG, SiG, and possibly more. All of these grafts should be straight and should be stable enough to carry the weight of the SSTE and resist the recoil forces.1,2
For forming all these grafts, rib cartilage seems much more suitable than the conchal ear cartilage as it offers abundant straight grafting material and more stability. The risk of unwanted warping may be minimized by use of oblique cutting technique and storage in saline solution for more than an hour. 3
We chose to perform an open approach due to the severity of the case and the need for perfect visualization and exposure of the underlying deformities. Other surgeons may as well have preferred the closed approach for this revision case, but in our hands, we preferred the optimal visualization.
For didactic purposes, we will classify the findings into 3 different anatomical groups: tip complex and alar base, middle and bony vault, and SSTE.
Tip Complex and Alar Base
The clinical examination of the tip complex and alar base showed a short nose with cloverleaf of the tip and pollybeak deformity of the profile, effacement of the tip defining points, axis deviation, columella retraction, nostrils asymmetry, deprojected tip, overrotated tip, lack of tip support, alar pinching on the left side, and external valve collapse.
All of the abovementioned findings are probably attributable to an (asymmetric) overresection of the LLCs as well as to severe injury and weakening of the of the tip support mechanism, including Pitanguy ligament, interdomal ligaments, membranous septum, and scroll ligaments. The aggressive cephalic trim of the LCs led to weakening of the lateral support and collapse of the internal nasal valve. The columella retraction was caused by shortening of the caudal septum and scarry retraction.
A flat nose, cloverleaf, deprojected, and short nose with alar base and columella irregularities represent a proper indication for the usage of CSEG, TG maneuvers in combination with AARG or lateral crural extension grafts. 1 The CSEG will address the shortened nose and columella retraction. Furthermore, it creates a stable central pillar for reprojection of the deprojected flat and pinched nose and nasal tip1,4 (Figures 3 and 4). The AARGs will address the alar base irregularities (pinching, retraction, asymmetries, cloverleaf, alar furrow) and stabilize the external valve collapse 1 . Additionally, we used a tip SiG with buttress graft elongate the nose even more and add more projection to the tip.5,6
We preferred using AARGs to lateral crural strut grafts as the last need more cartilaginous material. 1 Furthermore, AARGs with CSEG in combination have been established to be a great indication for the external valve obstruction with cloverleaf flat nose.1,7
Middle Vault Findings and Bony Pyramid
We suggest that the wide middle vault with open-roof deformity and inverted-V-deformity with collapse of the internal nasal valves in this case is strongly related to the overresection of the nasal dorsal hump with insufficient reconstruction of the middle vault and incomplete osteotomies. 2 To address this issue, we reconstructed the middle vault with bilateral extended SGs to reconstruct and align the brow-tip defining points aesthetic line and reconstruct the internal nasal valve.2,8 The completion of transverse and lateral osteotomies was done first to narrow the bony pyramid and to close the open roof.
Pollybeak Deformity
This deformity typically results from an overresection of the bony dorsum, in combination with insufficient cartilaginous dorsal resection and unwanted tip support injury and tip ptosis. It may be resolved by completion of cartilaginous dorsal resection and tip reprojection as explained above. 5
Skin and Soft Tissue Envelope
Skin and soft tissue damage may be found short- and long-term after rhinoplasty.9,10 A certain (temporary) damage will be observed after any intervention, seen as hematoma, bruising, ecchymosis, or edema. Factors increasing the risk for long-term damage include surgical dissection within a too superficial plane. Current publications suggest a supraperichondrial dissection or even subperichondrial dissection for a maximum preservation of blood vessels, nerves, and soft tissue.9,10 Iatrogenic soft tissue damage may—in cases of thin-skinned patients—lead to discolorations and unpredictable scar formation. 9
There are limited data on skin rejuvenation and restoration in the nasal area but publications on free fat transfer yield evidence that adipocytic stem cells—which are found in harvested fatty tissue—may help to partially restore surrounding tissues. 11
One factor that may have attributed to the soft tissue pollybeak is the inadvertent dissection of the deep Pitanguy ligament which then lead to a loss of tip support, a supratip soft tissue bulge and the formation of soft tissue in this area.
Lastly, SSTE damage was at least partially caused by the repeated postoperative HA injection used to camouflage aesthetic flaws. From anatomic dissections, experiences with the so-called “liquid rhinoplasties” and case reports from the literature, it is known that HA injections in the nasal area harbor a significant risk for blood vessel obstruction leading to atrophic skin damage or even necrosis, blindness, or ischemic insult. 12 The risk is especially elevated in revision cases that have had surgery before. 12 It is our recommendation to be very reluctant with the use of HA fillers in such scenarios and to leave this to extremely experienced injectors.
Conclusion
Rhinoplasty remains a highly sophisticated operation bearing the potential of great outcomes but also devastating aesthetic and functional results. Modern surgical techniques offer technical solutions for most aesthetic and functional challenges. Especially, the management of the soft tissue envelope gains more and more attention. Detailed analysis of revision rhinoplasty cases helps to achieve a better understanding of the short- and long-term effects of different techniques to avoid unpredictable and unwanted outcomes for patients and doctors.
Footnotes
Authors’ Note
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.