
Abstract
Objectives:
It is extremely difficult to obtain ideal tip projection and nose lengthening by septal extension graft using only septal cartilage in Asians, because their nasal septal and alar cartilages are small and weak. Therefore, we introduce a new septal extension graft using a cartilage–bone complex with the vomer and the perpendicular plate of the ethmoid bone as well as cartilage to obtain optimal outcomes.
Methods:
Participants included 30 patients who underwent surgery by external approach. The septal cartilage, vomer, and perpendicular plate of the ethmoid bone harvested by septoplasty were used. There were 2 layers of cartilage on each side and bone in between to create a strong cartilage–bone complex for projection and lengthening. The bony portion was placed in the tip side, and the double-layered cartilage portion was placed in the inferior portion of the caudal septum of the L-strut to create powerful fixation.
Results:
There were statistically significant improvements in nasal length (4.71 ± 0.65 vs 5.15 ± 0.53 cm, P value <.0001), tip projection (2.66 ± 0.40 vs 3.18 ± 0.42, P value <.0001), and nasolabial angle (94.0° ± 9.3° vs 107.2° ± 9.6°, P value <.0001) postoperatively. All patients were subjectively satisfied, and 2 different surgeons had excellent or good opinions in 28 (94%) patients.
Conclusions:
The sandwich technique using cartilage and bone complex results in satisfactory outcomes with stronger tip support, especially in Asians with a weak nasal tip who desire ideal tip projection and dramatic change.
Introduction
Nasal tip height and length is a critical factor affecting the aesthetic quality of the nose. It is also one of the biggest concerns for plastic surgeons. It is a major challenge for surgeons in Asian patients with thick skin, fragile cartilage, and short noses to obtain ideal tip projection and nose lengthening without contracture. 1,2
Using autogenous tissue on rhinoplasty, nasal septal cartilage is the most ideal graft because it is flat and wide, enabling various shapes. 3 Unlike the nasal dorsum, it is difficult to use artificial grafts for tip surgery. Therefore, cartilage is the most useful. Nasal septal cartilage is more commonly used than conchal cartilage because of the shape and convenience that are possible in the same surgical field. However, there are many cases in which an Asian patient’s nasal septal cartilage is small and weak, making it difficult to use septal extension graft (SEG) for tip projection or nose lengthening. 4 When a spreader graft, columellar strut, onlay tip graft, and shield graft are done at the same time, the amount of nasal septal cartilage is often insufficient. In cases of SEG done with septal cartilage, insufficient projection and nose lengthening are often obtained and bent if weak septal cartilage is placed only at one side of the L-strut. 5 Therefore, various modified surgical techniques for SEG are a challenge for tip surgery or correction of short nose in Asian patients. 4,6 -13 We introduce a new surgical technique to give optimal outcomes of nasal tip support, projection, and lengthening using an SEG composed of a cartilage–bone complex using the vomer and perpendicular plate of the ethmoid.
Patients and Methods
Patients
A retrospective analysis was performed on 30 patients who underwent sandwich technique using cartilage and septal bone complex as a standard tip-plasty during septorhinoplasty, between March 1, 2016, and November 31, 2016, at the Fresh Nose Clinic by one surgeon. We included patients who underwent this new technique regardless of other dorsal augmentation techniques, osteotomy, and trauma history. We excluded patients who underwent combined other tip-plasty and whose follow-up period was less than 6 months. Patients’ photographs and charts were reviewed for increasing tip projection and lengthening of the nose postoperatively. This study was approved by the Institutional Investigational Review Board of Korea National Institute for Bioethics Policy.
Surgical Technique and Management
All operations were done by an external approach under sedative anesthesia. The septal cartilage, vomer, and perpendicular plate of the ethmoid bone were carefully harvested by septoplasty technique. For strong SEG, we made a cartilage–bone complex and to distinguish it from other SEG techniques 14 using linked septal cartilage and bone, we call this technique the “sandwich technique” because the bone is inserted between 2 layers of cartilage (Figure 1). At first, we made a cartilage–bone complex that was sutured by 5-0 Nylon using the vomer and perpendicular plate of the ethmoid bone between 2 layers of cartilage (Figure 2). To consider the extent of projection and lengthening, the bony portion of the cartilage and bone complex was placed in the tip side to provide optimal projection and lengthening. A double layer of cartilage was inserted in the inferior portion of the caudal septum of the L-strut and strongly fixed by 5-0 nylon (Figure 3). Septal cartilage harvested by septoplasty was used, and if the patient had already previously undergone septoplasty or had insufficient septal cartilage, remained autologous rib cartilage after dorsal augmentation or donated rib cartilage was used. A hole was made in thin bone using an 18-G needle, and a small drill was used for thick bone to create the cartilage–bone complex. We used the aluminum external splint and silastic intranasal stent for 5 days and prescribed antibiotics for 7 days. We placed an alloplastic implant for dorsal augmentation from radix until upper lateral cartilage (ULC), so it did not affect tip outcome results.
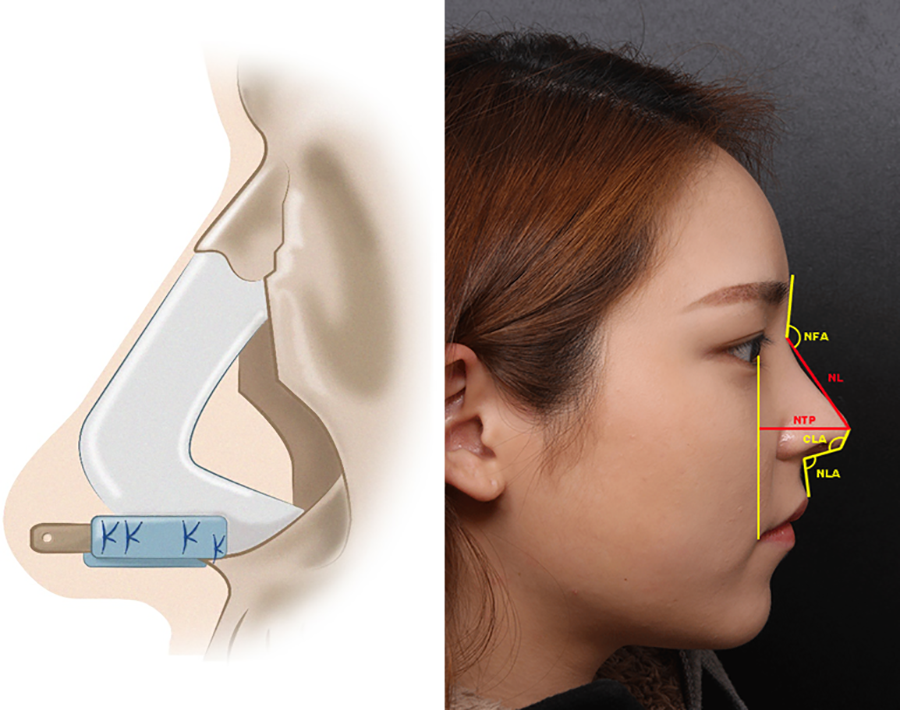
Surgical technique and anthropometric measurement. (Left) Illustration of cartilage and bone complex. (Right) Measurement points. NL indicates nasal length; NTP, nasal tip projection; NFA, nasofrontal angle; NLA, nasolabial angle; CLA, columella-lobular angle.
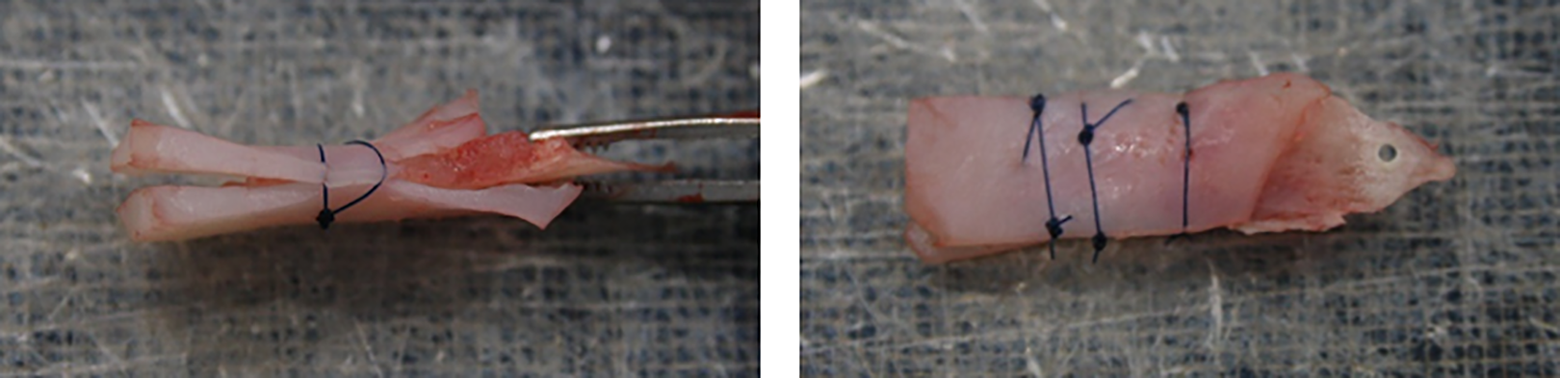
Intraoperative picture of cartilage and septal bone complex.
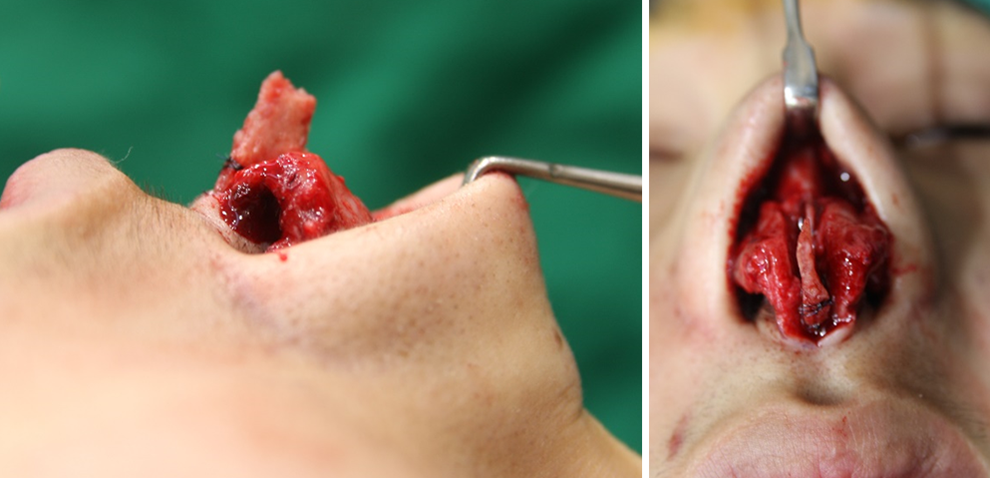
Intraoperative picture. Septal extension graft is placed in the lower caudal portion of the L-strut near maxillary crest. (Left) Lateral view. (Right) Caudal view.
Outcome Measurement
Anthropometric measurements were used as objective outcomes. Nasal length is the length from nasion to pronasale. Tip projection is the length between pronasale and alar line (perpendicular line between pupil and angular oris). Nasofrontal angle (NFA) is the angle between the lower forehead and nasal dorsum. Nasolabial angle (NLA) is the angle between the columella and the skin above the upper lip. Columella-lobular angle (CLA) is the angle between the columella and infratip lobule (Figure 1). For subjective outcome measurement, patient satisfaction regarding aesthetic outcome was assessed. Two specialists who did not participate in surgery analyzed aesthetic results by dividing cases into 4 grades of excellent, good, fair, or poor. Complications were also analyzed.
Statistical Analysis
SPSS version 21.0 software for Windows (SPSS, Inc, Chicago, Illinois) was used. Values are means ± standard deviations unless otherwise indicated. Preoperative and postoperative anthropometric measurements were compared with a paired t test. Differences were considered significance at P < .05.
Results
There were 30 consecutive patients (10 males and 20 females) who underwent septorhinoplasty, and all patients underwent sandwich technique using cartilage and bony septum complex. The patients’ average age was 31 ± 9 years. Primary septorhinoplasty was performed in 23 (77%) cases, and revision septorhinoplasty was performed in 7 (23%) cases. All of the cases were done by external approach, and septoturbinoplasty was performed at the same time. Other surgical techniques performed with tip-plasty included 21 (70%) cases of osteotomy, 10 (33%) cases of dorsal augmentation using silicon, 10 (33%) cases of dorsal augmentation using Alloderm, and 7 (23%) cases of paramaxillary augmentation (Table 1). The mean follow-up period was 7.9 ± 9.1 months and the range (6-14 months).
Patient Characteristics, Surgical Techniques.a
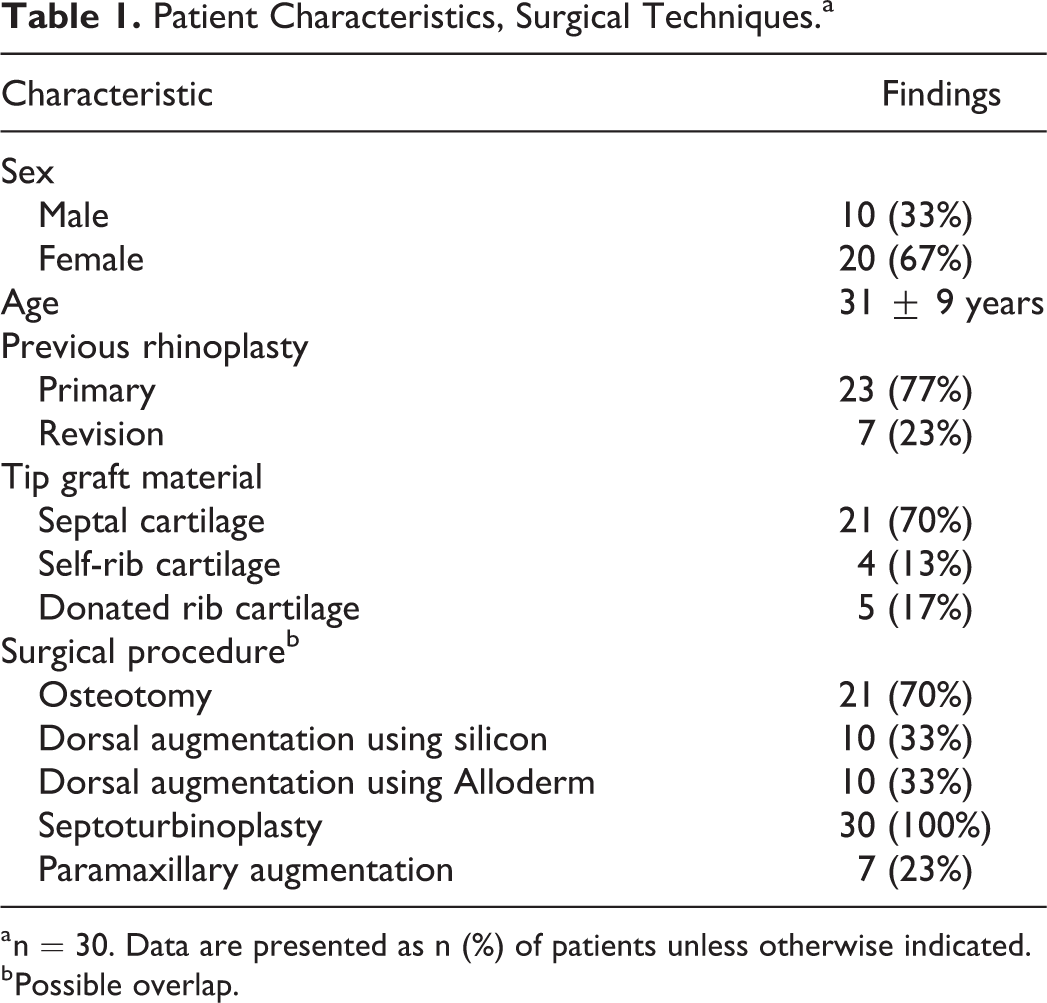
a n = 30. Data are presented as n (%) of patients unless otherwise indicated.
b Possible overlap.
Nasal measurements preoperatively were compared to measurements taken postoperatively at the last follow-up visit. There were statistically significant improvements in nasal length (4.71 ± 0.65 vs 5.15 ± 0.53 cm, P value <.0001), tip projection (2.66 ± 0.40 vs 3.18 ± 0.42, P value <.0001), and NLA (94.0° ± 9.3° vs 107.2° ± 9.6°, P value <.0001) postoperatively. However, there were no statistically significant improvements in NFA (145.7 ± 7.1 vs 147.3 ± 5.3, P value = .171) or CLA (131.2° ± 8.1° vs 133.3°±6.9°, P value = .186; Table 2).
Anthropometric Measurements.a
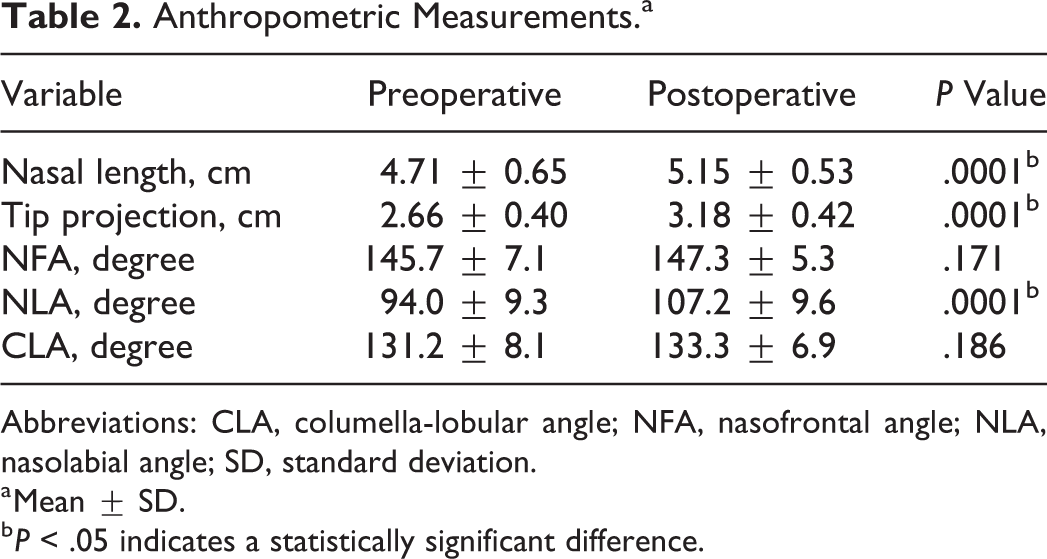
Abbreviations: CLA, columella-lobular angle; NFA, nasofrontal angle; NLA, nasolabial angle; SD, standard deviation.
a Mean ± SD.
b P < .05 indicates a statistically significant difference.
All patients were satisfied with surgery results (Figure 4). Specialist opinions indicated that 3 (10%) cases were excellent and 23 (77%) cases were good. Both excellent and good are considered successful surgery outcomes, and 26 (87%) cases were successful. Four (13%) cases were fair, and no cases were poor. There were no complications in 24 (80%) cases, notable transcolumellar scar in 3 cases, mild nostril asymmetry in 3 cases, and cartilage gauziness in 1 case (Table 3). There was no patient with infection, and no patient required reoperation within the study follow-up period.
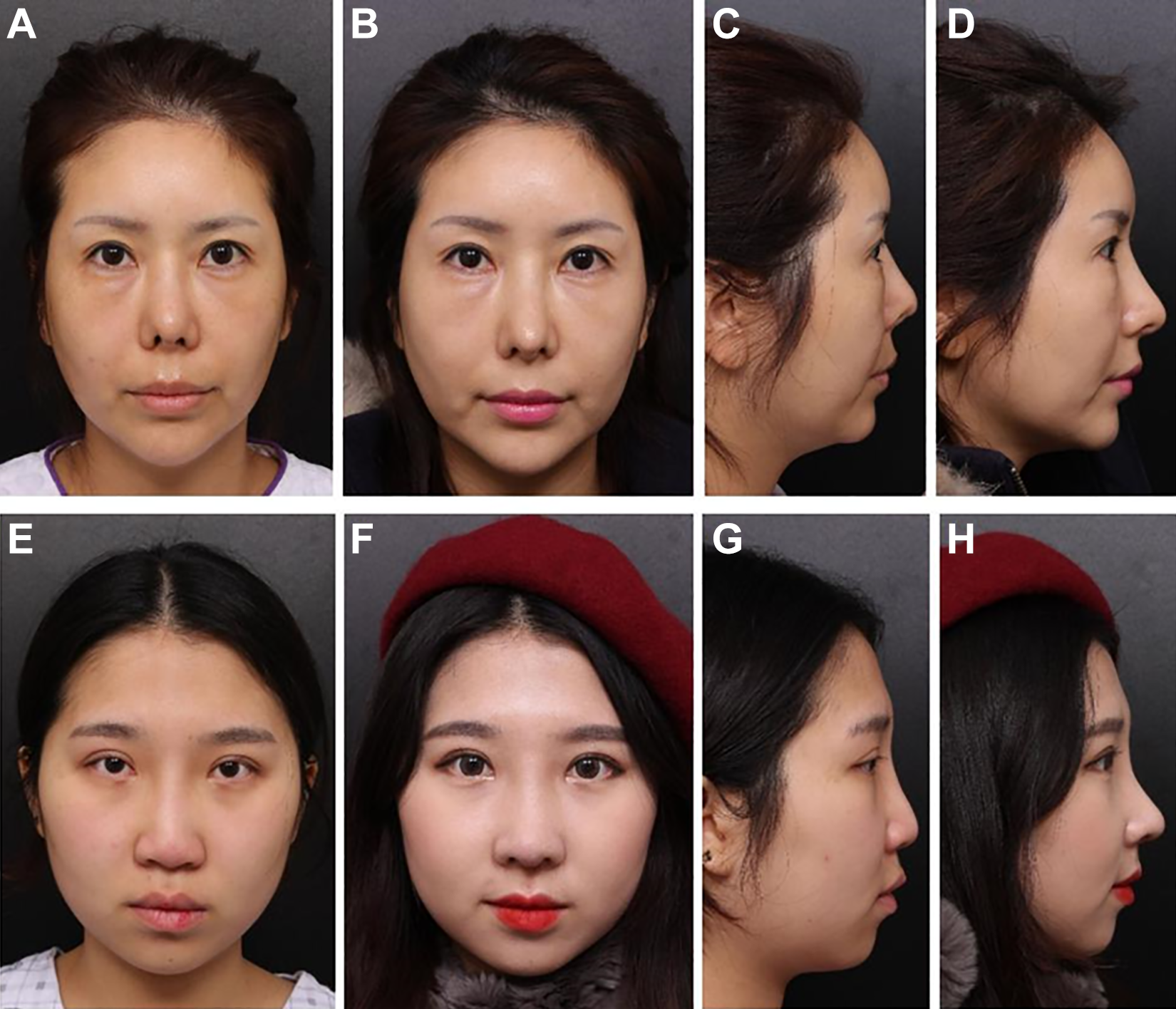
Facial photographs obtained preoperatively (A and C, E and G); 10 months (B and D); and 12 months (F and H) postoperatively.
Aesthetic Outcomes and Complications.a
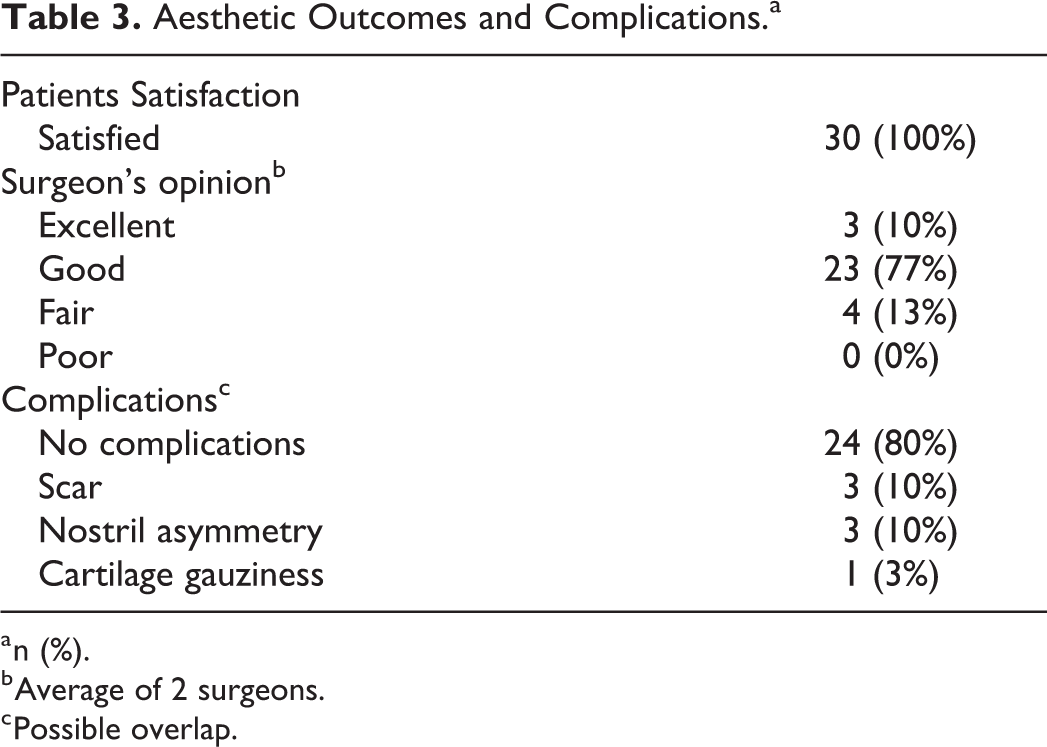
a n (%).
b Average of 2 surgeons.
c Possible overlap.
Discussion
In Asian rhinoplasty, especially, nasal tip-plasty, creating a desirable and attractive shape of nasal tip is important factor in determining patient satisfaction with surgery. However, due to anatomic characteristics of Asian patients such as weak cartilage and thick soft tissue of nasal tip, many plastic surgeons have difficulty achieving these goals in Asian patients. In addition, because of obvious postoperative scar of Asian patients, many patients hesitate when they need a donor site to harvest materials for graft such as auricular cartilage and costal cartilage.
L-type silicone had been used to improve nasal tip shape, but the risks of protrusion and infection are high when there is excessive tension. Therefore, autologous conchal and rib cartilage has been used to improve the shape of nasal tip and septal cartilage. However, the septal cartilage of most Asian patients is weak and small. It is difficult to obtain as much projection as the patient wants, and nose contracture frequently occurs when a surgeon operates by tip-plasty only with this weak cartilage and suture technique.
In the 1990s, SEG was introduced and developed into various modified techniques. Septal extension graft is recognized as a gold standard tip-plasty technique. 12,15 However, SEG has associated limitations and complications, such as hardness, loss of projection, and nasal tip deviation. 5 In particular, the remaining weak L-strut or implanted cartilage can twist and bend to one side. This phenomenon can occur when overlapped harvested septal cartilage is only sutured to the remaining L-strut with thread, and the weak remaining nasal septum can move back or bend to one side with tension. Also, surgical thread used to fix cartilage can carve the cartilage, so the nasal tip can drop. Absorption can occur when the implanted SEG is used with only weak harvested cartilage, a phenomenon that can occur with conchal cartilage or rib cartilage. Rib cartilage used for SEG is stronger than harvested septal cartilage, but its strength cannot increase because strength depends on the remaining L-strut, which is a weaker tissue. 16 Problems such as warping, donor site morbidity, and difficulty in carving can occur. 17 Autologous rib cartilage or irradiated homologous rib cartilage can be used. 18 Rib cartilage used for SEG is stronger than septal cartilage. However, there are some risks or disadvantages associated with using rib cartilage for tip plasty. The most important factor is warping, and the warping is more obvious when rib cartilage is cut into several pieces for grafting. This is the reason why the septal cartilage is the first choice for SEG, because rib cartilage can tend to warp or change shape. In addition, harvesting rib cartilage also has some disadvantages, including donor site morbidities such as vessel damage or iatrogenic pneumothorax during the harvest, chest wall deformities, persistent postoperation pain, and additional scarring in the chest wall. But the rib cartilage can be more useful when a strong strut is required due to contracture from previous surgeries or accidents, when tip projection is required, when the septal and auricular cartilage cannot be used due to a previous surgery, or when a large amount of autologous cartilage is needed. Because conchal cartilage is not flat, it is hard to use as a support. Therefore, conchal cartilage is generally used as the onlay graft. 19 In the patients in our study, more septal cartilage should be preserved as an L-strut for the stability of the nasal tip projection. This is the reason why the bony portion of nasal septum is considered as a component of complex graft. It is strong and flat enough to be a supporting strut for tip projection with 2 pieces of cartilage grafts. The bony septum such as perpendicular plate of ethmoid or vomer belongs to membranous bone. Membranous bone, such as the calvarium and facial bones, forms by direct condensation from mesenchyme. Peer reported in 1950 that membranous bone grafts survived better than endochondral bone graft when transplanted into soft tissue sites. 20 He believed that membranous bone grafts survived better because they do not require functional stress at the site of grafting to maintain volume, whereas endochondral bone grafts do require functional stress to prevent resorption. Gibson also showed that endochondral bone grafts are often resorbed when grafted into soft tissue sites when there is no apposition, while membranous bone grafts do not require bony contact to survive. 21
Some surgeons use artificial plates such as porous high-density polyethylene sheets for SEG, 9 but artificial implants introduce major problems such as stiff tip, infection, or exposure. 22 There are some studies about safe and effective SEG using polydioxanone absorbable plates. However, the authors conclude that absorbable plates are only used to secure grafts while autologous grafts contribute to stabilization of projection, length, and structure over time. Also, the follow-up period is too short to predict long-term results. 8
The most important point in SEG is preventing collapse or deviation to one side of a remnant weak L-strut after implantation of SEG. In our sandwich technique, double cartilage is placed at the lower part of the L-strut to prevent deviation and create maxillary crest support to secure L-strut stability and prevent collapse. This is the same reason why some surgeons use L-shaped columellar struts to stabilize weak septum. 23 Research on SEG performed with only nasal septal bone showed strong constructs for tip surgery, but nasal tip stiffness can occur. 10 In our sandwich technique, elasticity is maintained up to a certain point by placing cartilage at the lower portion. In addition, the sandwich technique provides more stability by placing cartilage on both sides of the L-strut rather than on only one side.
In Asians, it is not enough to perform SEG with only harvested septal cartilage due to a weak and small amount of septal cartilage. Especially, when lengthening the nasal septum of an Asian patient, dead space can form at the end of the ULC because of ULC weakness. With time, the dead space may become infected and fill with pus, so it is important to support the end of the ULC. The sandwich technique is preferable to performing SEG with weak and small septal cartilage. The septal bone has guaranteed strength and can powerfully lengthen the tip of the nose. Fixation of lower lateral cartilage to implanted nasal bone causes definite projection and nasal lengthening and decreases the possibility of dead space at the ULC.
Sometimes, the septal bone is used as a spreader graft to reinforce the end of upper cartilage and prevent movement back in short noses. Previously, septal cartilage and bone complexes have been used for SEG, which is completely different from our technique. Previous techniques harvested septal cartilage and bone together to increase the amount of material, while we harvest them separately and reinforce them using doubled cartilage. 14
The gap between the nasal septal angle and the sandwich SEG is supported by the lower lateral cartilage by fixing the lower lateral cartilage to the hole of sandwich SEG, so that the gap between them becomes fibrous and maintains firmness over time.
Our sandwich technique using cartilage and septal bone complex has some potential drawbacks. Aggressive graft may hamper proper closure of the transcolumellar incision, and this may result in a visible scar and a mild nostril asymmetry postoperatively. Two-layered cartilage graft may give a result of wide columella base, but as time goes on, some of them can be absorbed. Although this technique has been used for several years with satisfactory results, due to the limitation of short-term follow-up, longer period of follow-ups are needed for evaluation of long-term results.
However, despite the potential drawbacks, we found that the technique resulted in positive outcomes in most of the patients in this study. If this procedure is applied in selective patients who have definitely thick skin and in situation of patients refusing additional donor sites, our sandwich technique using cartilage and septal bone complex will be useful option for tip-plasty.
In conclusion, when strong tip support and nose lengthening is required for ideal tip projection and dramatic changes in weak tips in Asian patients, the sandwich technique provides good results with few complications. This sandwich technique uses a cartilage and bone complex made of cartilage, vomer, and the perpendicular plate of the ethmoid bone.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.