
Abstract
Introduction
Epistaxis is one of the common diseases in otorhinolaryngology. According to statistics, about 60% of the general population have experienced epistaxis. 1 Since the condition of the nasal mucosa is an important factor causing spontaneous epistaxis, and the condition of the nasal mucosa is usually affected by environmental and meteorological factors, it can be considered that environmental and meteorological factors may be an important factor causing spontaneous epistaxis.
Previous studies have shown that the occurrence of epistaxis is related to environmental and meteorological factors.2-6 Lu et al 3 found that epistaxis in children in Beijing was related to air pollutants. Ahn and Min 4 found that average relative humidity, minimum temperature, sunshine duration, SO2 concentration, and average wind speed were negatively correlated with the occurrence of epistaxis, while particulate matter (PM) 10 concentration and average temperature were positively correlated with epistaxis occurrence. Kim et al 5 discovered that the incidence of epistaxis was positively correlated with the average temperature, average wind speed, sunshine hours, and PM10 concentration in children. In adults, cloud cover and PM10 concentration were positively correlated with the incidence of epistaxis, while minimum temperature and average relative humidity were negatively correlated with the incidence of epistaxis. All the above studies indicate that environmental and meteorological factors are related to the occurrence of epistaxis, and the influencing factors of epistaxis in different age groups may be different.
In the past, our research found that the incidence of epistaxis in Yangzhou was significantly positively correlated with air pollutants. 6 Hence, we intend to classify epistaxis patients by age for a more detailed analysis of the association between environmental and meteorological factors and epistaxis across various age groups. It is one of the few studies on the relationship between epistaxis and environmental and meteorological factors in China, providing a reference for reducing and preventing epistaxis and rationally arranging medical and health resources.
Methods
Clinical Data
A retrospective study was conducted on patients with epistaxis who were treated in the outpatient and emergency Department of Otolaryngology, Head and Neck Surgery, Northern Jiangsu People’s Hospital of Jiangsu Province from January 1, 2016, to December 31, 2020.
Inclusive criteria: The diagnosis of epistaxis adhered to applicable diagnostic criteria. 6 Systematic collection of patient data, including age, sex, visit time, and diagnosis. The repeated visits of the same patient within 2 weeks were counted as a single case.
Exclusion criteria: Patients with secondary epistaxis caused by hematological disorders, oral anticoagulants, foreign bodies in the nose, history of trauma, nasal surgery, or tumors were excluded from the study.
Patients were divided into 4 groups based on their age at the time of the visit: age group 1 (0-17 years old), age group 2 (18-40 years old), age group 3 (41-60 years old), and age group 4 (over 60 years old).
Environmental Data Collection and Processing
The concentration data of 6 air pollutants [sulfur dioxide (SO2 μg/m3), ozone (O3 μg/m3), nitrogen dioxide (NO2 μg/m3), carbon monoxide (CO mg/m3), PM2.5 (μg/m3), and PM10 (μg/m3)] were sourced from the national urban air quality real-time publishing platform of China Environmental Monitoring Station (http://www.cnemc.cn/). Concentrations of CO, NO2, PM2.5, PM10, and SO2 represented 24-hour averages, while O3 concentration denoted daily maximum 8-hour moving averages. Meteorological data from the National Oceanic and Atmospheric Administration consist of the National Center for Environmental information (https://www.ncei.noaa.gov/data/global-summary-of-the-day/archive/), meteorological data, including temperature difference (°C), average temperature (°C), average humidity (%), average wind speed (m/second), and cumulative sunshine time (hour). Data were collected every 3 hours, and daily averages were computed.
Statistical Analysis
Statistical software SPSS 25 was used to analyze the data. Data with normal distribution were expressed as x ± s. A stepwise linear regression model was constructed based on the Akaike Information Criterion to identify factors related to epistaxis. The stepwise selection method was adopted to select and delete variables according to predefined statistical criteria (input P < .05, deletion variable P > .10). Variables were chosen based on their P-value at each step, and a P-value threshold of .05 was used to limit the total number of variables included in the final model. Both were two-sided tests, and P < .05 was considered statistically significant.
Results
A total of 24,407 patients with epistaxis were included in this study, and predominantly male across all 4 age groups, with the largest number of patients in age group 1. The amount of epistaxis in age group 1 gradually increased from 2016 to 2019 and decreased in 2020. The amount of epistaxis in age groups 2, 3, and 4 gradually decreased from 2017 to 2020. The variation trend of epistaxis in age groups 1 and 2 was similar with month, and there were 2 peak periods (May and August) each year. The variation trend of epistaxis in age groups 3 and 4 was similar with month, and the peak period was in April and March, respectively (Figures 1 and 2). Annual average temperatures ranged from 3.39°C in January to 28.39°C in August, with the highest temperature difference in April (10.68°C) and the lowest in July (7.14°C). Pollutant concentrations varied, with significant fluctuations in PM2.5, PM10, and O3, while CO concentrations showed minimal change (Figure 3).
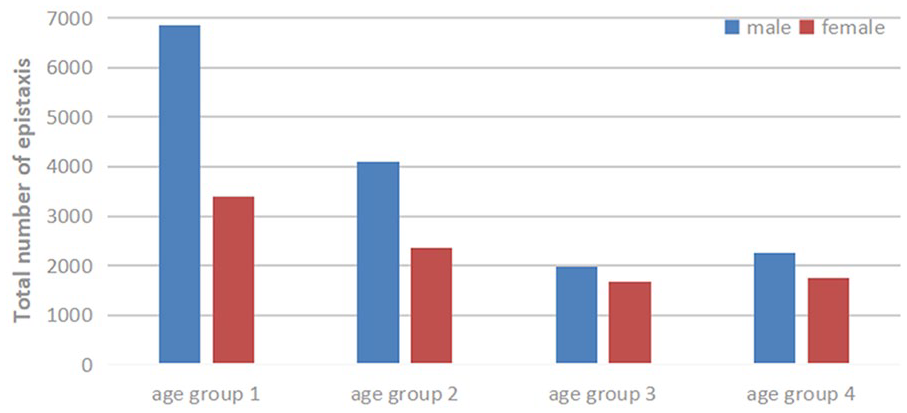
Gender and age distribution of epistaxis.
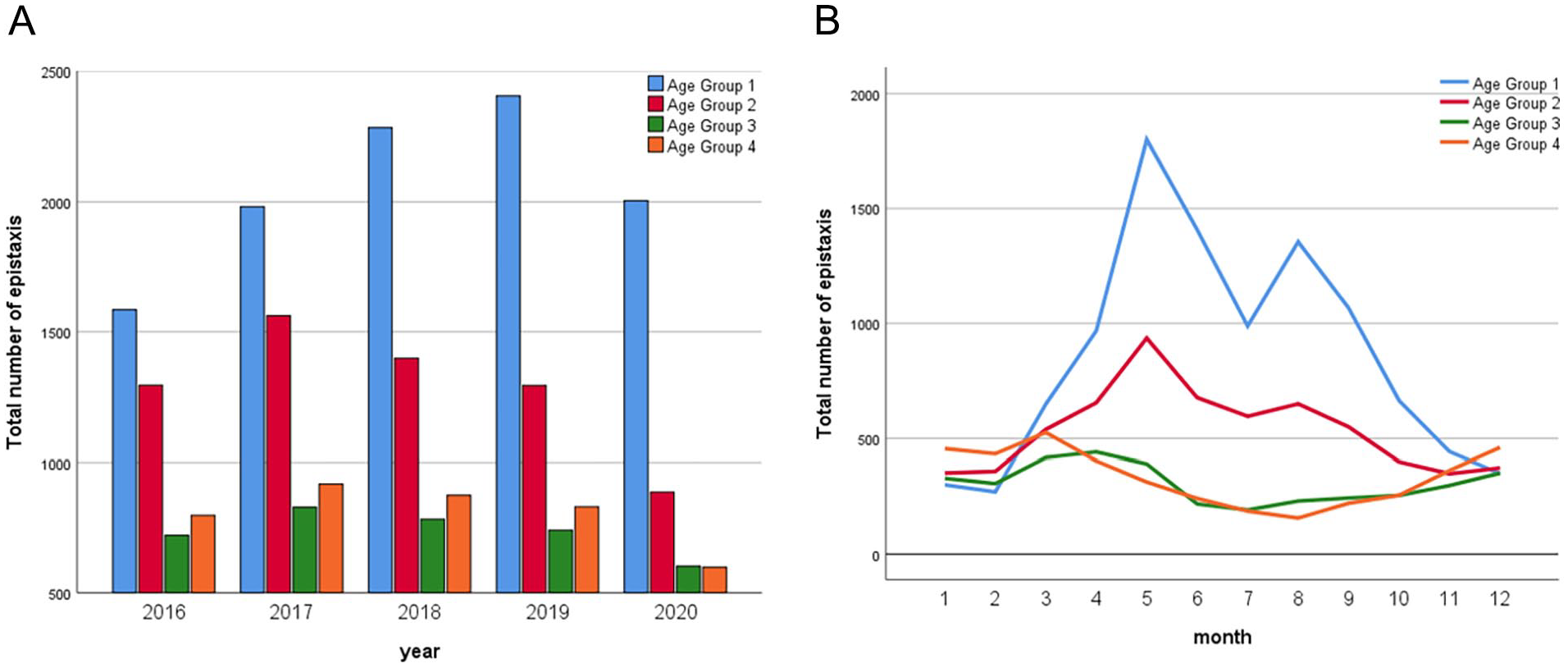
Total number of epistaxis from 2016 to 2020. (A) Yearly distribution of epistaxis. (B) Monthly distribution of epistaxis.
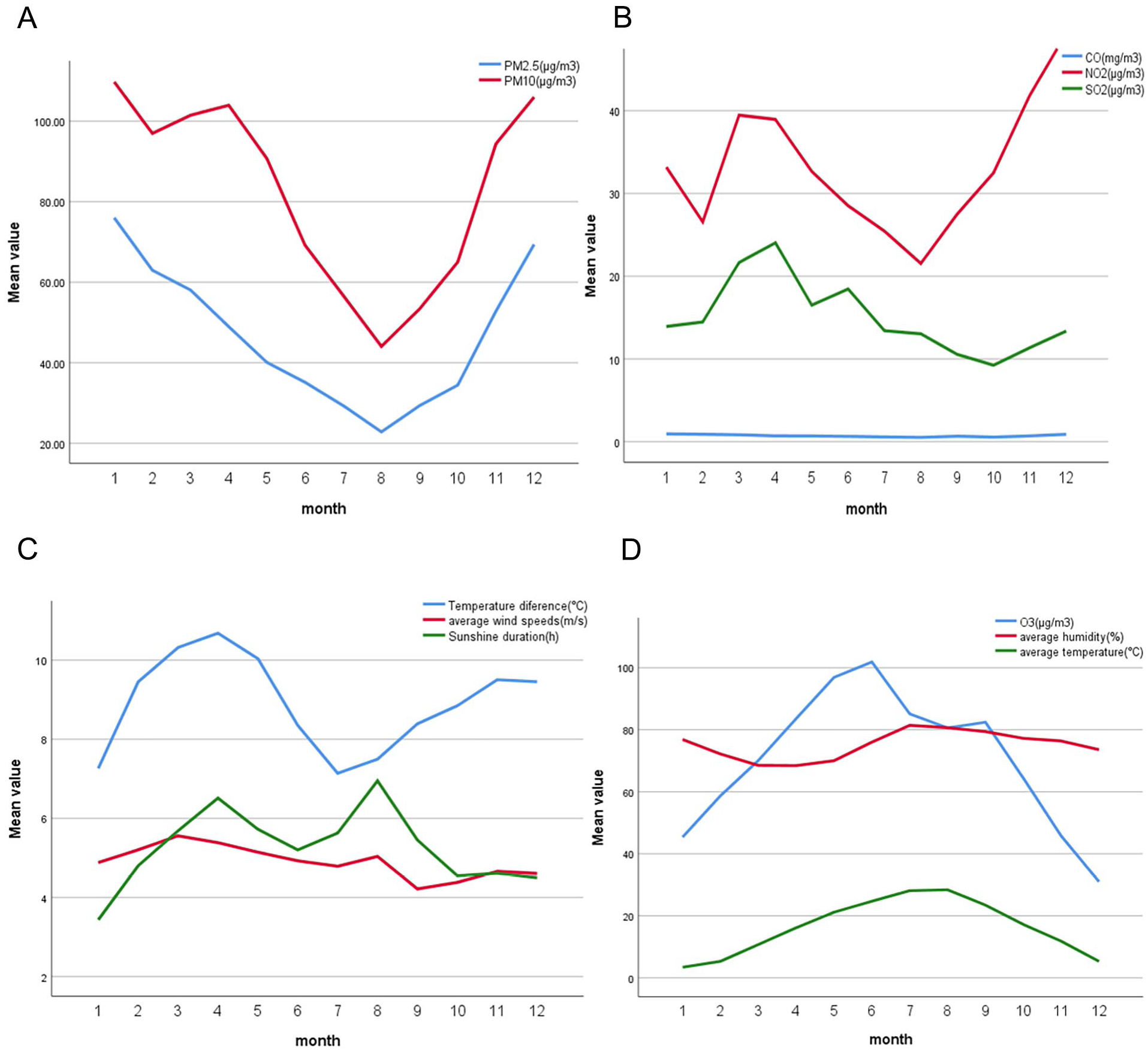
The mean values of the meteorological factors and air pollutants from 2016 to 2020. (A) Monthly mean values of PM2.5 and PM10. (B) Monthly mean values of the CO, SO2, and NO2 concentrations. (C) Monthly mean values of temperature difference, average wind speeds, and sunshine duration. (D) Monthly mean values of the CO concentrations, average humidity, and average temperature.
Stepwise regression analysis evaluated the relationship between environmental and meteorological factors with epistaxis. The results showed that the regression model had significant statistical significance (P < .001). O3 concentrations, average humidity, average temperature, NO2 concentrations, sunshine duration, average wind speed, CO concentrations, and temperature difference had statistically significant effects on epistaxis (P < .05; Table 1).
Stepwise Regression Models of Air Pollution and Meteorological Factors in Different Age Groups.
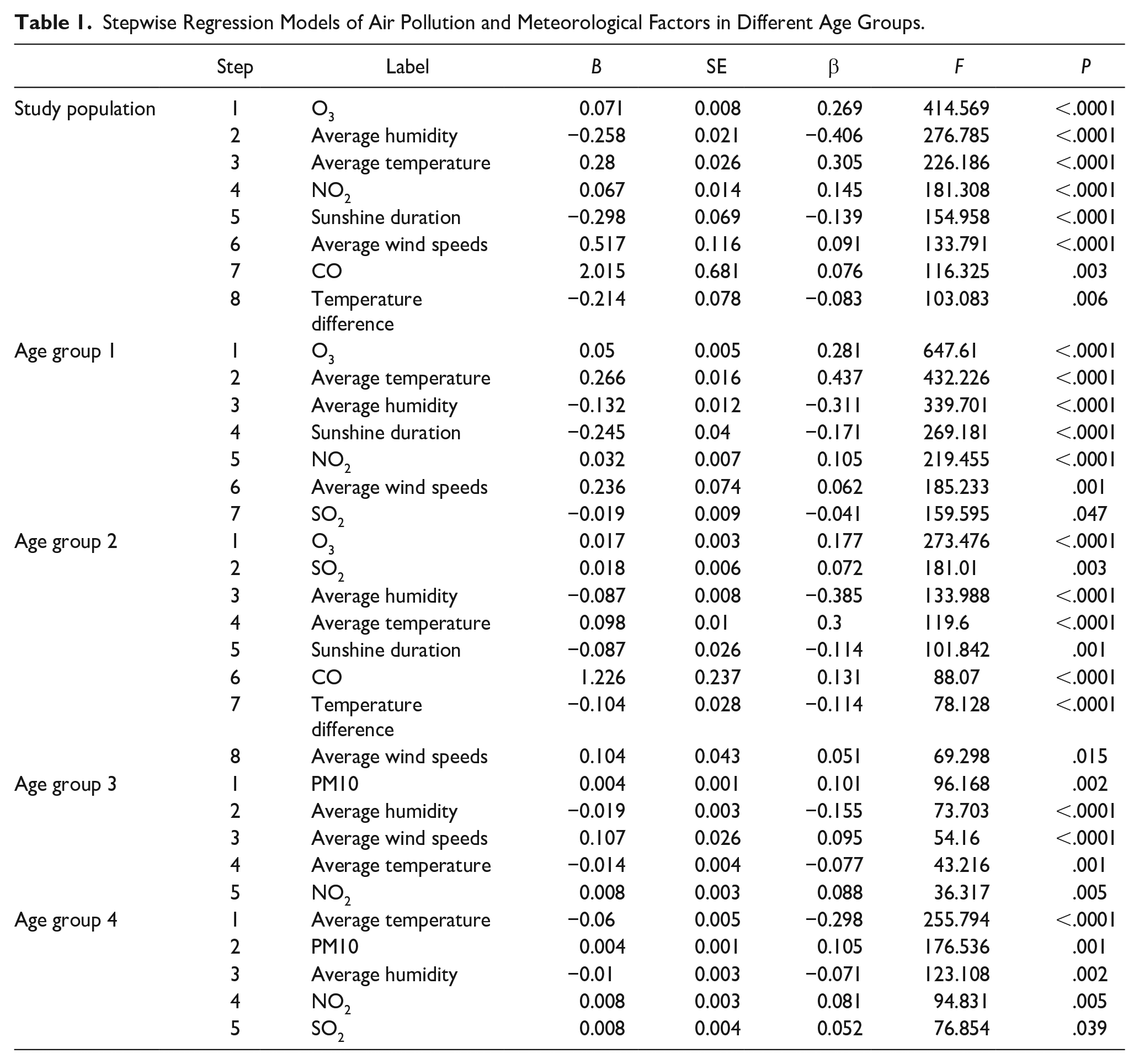
Stepwise regression analysis was performed for each age group, and the results showed that all 4 regression models had significant statistical significance (P < .001), but the association between environmental factors and epistaxis differed between the 4 age groups. In age group 1, O3 concentration, average temperature, average humidity, sunshine duration, NO2 concentration, average wind speed, and SO2 concentration had statistically significant effects on epistaxis (P < .05). In age group 2, O3 concentration, SO2 concentration, average humidity, average temperature, sunshine duration, CO concentration, temperature difference, and average wind speed had statistically significant effects on epistaxis (P < .05). In age group 3, the effects of PM10 concentration, mean humidity, mean wind speed mean temperature, and NO2 concentration on epistaxis were statistically significant (P < .05). In age group 4, the effects of mean temperature, PM10 concentration, mean humidity, NO2 concentration, and SO2 concentration on epistaxis were statistically significant (P < .05; Table 1).
Discussion
A total of 24,407 patients with epistaxis were included in this study. The number of epistaxis patients in age groups 1 and 2 showed a similar trend each month, with 2 peak periods per year (May and August). The number of epistaxis patientsin age groups 3 and 4 were similar month by month, with the peak in April and March, the amount of epistaxis was different in each age group, indicating that seasonal changes had different effects on the incidence of epistaxis in each age group.
In this study, it was found that the occurrence of epistaxis was negatively correlated with average humidity and temperature difference, whereas epistaxis was positively correlated with O3 concentration, average temperature, NO2 concentration, sunshine time, average wind speed, and CO concentration. This study categorized patients into 4 age groups and found that male patients are more common. However, age group analysis revealed that meteorological factors and air pollutants associated with epistaxis differed in each age group.
We discovered that the number of epistaxis in the 4 groups was negatively correlated with the average humidity, that the number of epistaxis in age groups 1 and 2 were positively correlated with the average temperature, and that the number of epistaxis in age groups 3 and 4 were negatively correlated with the average temperature. Matsumoto et al 7 found that the number of daily cases of epistaxis was significantly negatively correlated with the average daily relative humidity. Akdogoan et al 8 found that children’s epistaxis was negatively correlated with the daily mean humidity and the difference between daily maximum and minimum humidity. Similarly, Gatsounia et al 9 reported a statistically significant negative correlation between the incidence of epistaxis and the average relative humidity observed on a daily and weekly basis. Low air humidity may desiccate nasal mucosa, rendering it vulnerable to bleeding. Previous research on temperature’s impact on epistaxis yields conflicting results, with some studies suggesting a predisposition to spontaneous epistaxis at low temperatures.1,2,10,11 While others find no correlation between temperature and the incidence of epistaxis.9,12 This study proposes a correlation between temperature and epistaxis occurrences, with varying effects across distinct age groups. Additional research is required to ascertain the significant influence of temperature on epistaxis incidence.
The impacts of other meteorological factors differ across age groups. In this study, sunshine duration, average wind speed, and temperature difference all had certain effects on the epistaxis in different groups. For example, the regression coefficients of average wind speed in age group 1, 2, and 3 were 0.062, 0.051, and 0.095, respectively. The regression coefficients of sunshine duration in age groups 1 and 2 were −0.171 and −0.114, respectively. The regression coefficient of temperature difference in age group 2 was −0.114. These results indicate that the effects of various meteorological factors on epistaxis differ in different age groups.
As the nasal cavity is the first part of the respiratory tract to come into contact with the environment, the nasal epithelium may be damaged by environmental pollutants in the air, resulting in epistaxis.13-15 This study found that air pollution indicators except PM2.5 concentration are associated with epistaxis in different age groups. O3 and PM10 concentration affect multiple groups. O3 concentration is positively correlated with age groups 1 and 2. PM10 concentration was positively correlated with age groups 3 and 4. NO2, SO2, and CO concentrations are also positively correlated with different age groups. At present, most studies have found that PM10 is positively correlated with the occurrence of epistaxis,4,5,16 but studies on children with epistaxis have found that PM10 is negatively correlated with the occurrence of epistaxis. 3 According to the relationship between epistaxis and PM10 concentration in children of different age groups, it is found that PM10 concentration is associated with the occurrence of epistaxis in young children (0-5 years old), but PM10 is not a significant risk factor in older children (6-18 years old). 16 According to the results of our study, the effects of air pollutants on epistaxis in different age groups are different, and further detailed studies are needed.
Previous studies have shown that allergic rhinitis is related to the occurrence of environmental meteorology and epistaxis.17-22 Chen et al 18 found that the risk of allergic rhinitis significantly increases at higher temperatures (19.8°C). However, as humidity increases, the number of clinic visits for allergic rhinitis decreases, suggesting that high humidity has a protective effect. 23 Additionally, increases of 10 μg/m³ in atmospheric pollutants O3, SO2, and PM10 correlate with an increase in clinic visits for allergic rhinitis, indicating that air pollution heightens the risk of allergic rhinitis attacks. Children diagnosed with allergic rhinitis are 2.4 times more likely to experience epistaxis.21,22 Therefore, changes in environmental and meteorological conditions may exacerbate allergic rhinitis symptoms, leading to increased nasal mucosal congestion, edema, and erosion, which can cause the rupture of small blood vessels in the nasal cavity, triggering epistaxis. However, we could not exclude the interference of allergic rhinitis in the study results, which is also the direction of our future research.
As we all know, there is a difference between indoor and outdoor environmental meteorology, 24 especially in winter and summer. More time spent indoors may lead to less exposure to outdoor weather factors and allergens, leading to a lower incidence of epistaxis. 16 In the future, we can further study the influence of indoor and outdoor environmental differences on the occurrence of epistaxis.
The causes of epistaxis include local and systemic factors, so this study has some limitations. First, the data of all medical institutions in Yangzhou were not included. Second, this study only excluded patients with nasal trauma, tumors, foreign bodies, surgery, and blood diseases, and did not analyze the influence of systemic diseases (such as hypertension, diabetes, arteriosclerosis, upper respiratory tract infection, allergic rhinitis, etc.) on epistaxis.
Conclusion
This study showed that the environmental and meteorological factors were related to the occurrence of epistaxis in Yangzhou, among which average humidity and temperature difference are negatively correlated with the occurrence of epistaxis, while O3, average temperature, NO2, sunshine duration, average wind speed, and CO are positively correlated with epistaxis occurrence. However, the impact of these environmental and meteorological factors varies in different age groups. In the future, we need further research and in-depth discussion.
Footnotes
Data Availability Statement
Some or all data, models, or code generated or used during the study are available from the corresponding author by request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Jiangsu Province natural science Foundation project (BK20201220).
Ethical Standards
According to the Ethics Committee of Northern Jiangsu People’s Hospital, this research has no harm to human body, does not involve sensitive personal information or commercial interests, and can be exempted from ethical review.