
Abstract
Background
Epistaxis is one of the most common symptoms in otolaryngology, which can be caused by nasal disease or systemic disease. With the development of the economy, people have paid more attention to the problem of air pollution. As the first portal of respiratory defense, the nasal cavity is the first to be harmed by air pollutants. This study aimed to analyze the epidemiology of epistaxis in the Yangzhou population from 2017 to 2021 and to investigate the correlation between the incidence of epistaxis and local ambient air pollutants. The objectives were to elucidate the symptoms of epistaxis in this demographic and evaluate the effects of air pollution on these symptoms. The ultimate goal is to mitigate the incidence of epistaxis and optimize the allocation of healthcare resources.
Material and Methods
Subjects
Data of patients with epistaxis who were admitted to the outpatient and emergency department of otolaryngology, head and neck surgery, Northern Jiangsu People’s Hospital Affiliated to Yangzhou University from January 1, 2017, to December 31, 2021, were collected.
Inclusive criteria: The diagnosis of epistaxis adhered to applicable diagnostic criteria. 1 Systematic collection of patient data, including age, sex, visit time, and diagnosis. The repeated visits of the same patient within 2 weeks were calculated as 1 case.
Exclusion criteria: Patients with secondary epistaxis caused by hematological disorders, oral anticoagulants, foreign bodies in the nose, history of trauma, nasal surgery, or tumors were excluded from the study.
Air Pollution Data
The data of air quality index (AQI) and air pollutant concentration [carbon monoxide (CO), nitrogen dioxide (NO2), ozone (O3), particulate matter (PM2.5, PM10), sulfur dioxide (SO2)] are derived from the China Environmental Monitoring Station’s real-time publication platform of urban air quality (http://www.cnemc.cn/). The AQI, CO, NO2, PM2.5, PM10, and SO2 concentrations represent 24 hour averages, while the average concentration of O3 is based on the daily maximum 8 hour moving average. In addition, the concentration unit of CO is expressed in mg/m3, and the concentration unit of other pollutants is μg/m3. The AQI group: According to the AQI value, the patients with epistaxis in the Yangzhou area were divided into 3 groups according to the day: AQI ≤ 50 (excellent) group, 50 < AQI ≤ 100 (good) group, and AQI > 100 (polluted) group.
Statistical Analysis
Statistical analyses were performed using IBM SPSS for Windows, version 25.0. The measurement data were presented as mean ± standard deviation, and the counting data were expressed as n. The data conforming to the normal distribution were compared by the T test or ANOVA. Nonparametric test methods are used for data that did not conform to the normal distribution: Mann-Whitney U test or Kruskal-Wallis test. Spearman correlation analysis showed that there was a correlation between AQI, air pollutant concentration, and the number of epistaxis. Spearman correlation analysis was used to analyze the association between the concentrations of air pollutants on the treatment day and 14 days before treatment and the number of epistaxis on the day of onset, to evaluate the time lag effect. The data of all groups were statistically significant with P < .05.
Results
Patients With Epistaxis
From January 1, 2017, to December 31, 2021, 24,721 patients with epistaxis were enrolled in this study, including 15,391 males and 9330 females. There were 10,464 cases, including 6936 males and 3528 females, aged from 0 to 17 years. There were 6640 cases aged between 18 and 40 (4201 males and 2439 females), 3672 cases aged from 41 to 60 (1967 males and 1705 females), and 3945 cases aged over 60 (2287 males and 1658 females). Epistaxis was more common in men (62.26%), with a higher incidence in the 0 to 17 age group (42.33%), followed by the 18 to 40 age group (26.86%), the over 60-years-old (16%) and the 41 to 60 age group (14.9%; Figure 1).
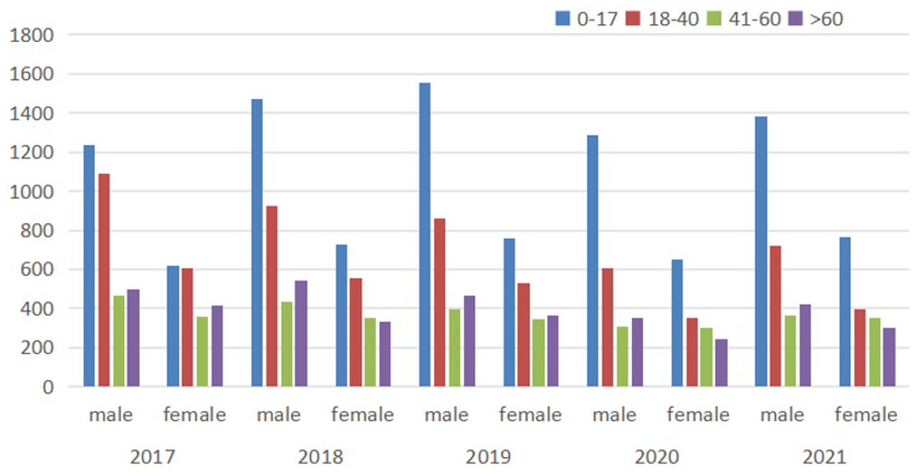
Annual sex and age distribution of patients with epistaxis.
From 2017 to 2021, there were 5302, 5342, 5273, 4091, and 4713 epistaxis per year, respectively. Analysis of variance showed that there were no significant statistical differences in the number of epistaxis between 2017, 2018, 2019, and 2021 (P > .05), but there was a significant statistical difference between 2020 and the other 4 years (P < .05). The number of epistaxis visits in 2020 was significantly lower than that in previous years, and increased in 2021.
Results by Month
There were significant statistical differences in daily epistaxis visits in different months in Yangzhou (P < .05), among which the number of visits in April, May, and June was higher, while the number of visits in December, January, and February was lower (Table 1 and Figure 2), and the lowest value existed in February 2020 and August 2021.
The Daily Number of Epistaxis Visits and the Results of AQI and Air Pollutants in Each Month.
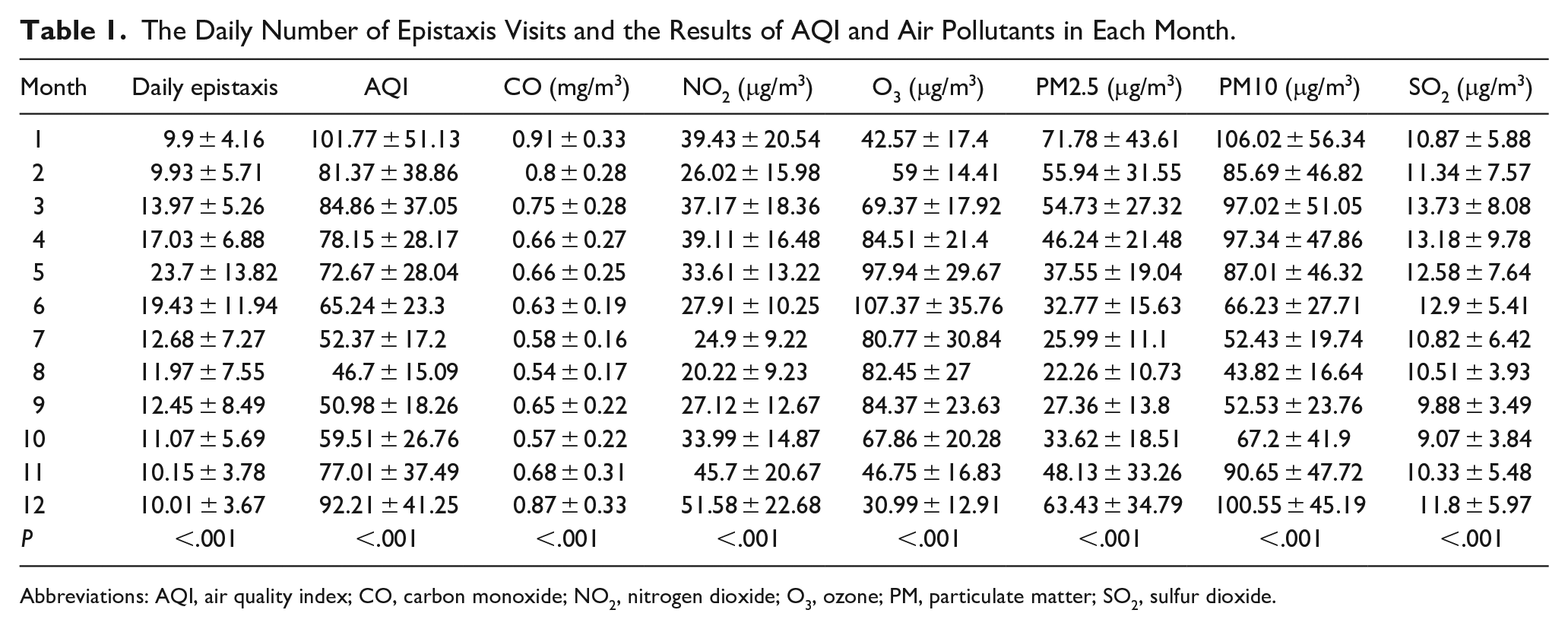
Abbreviations: AQI, air quality index; CO, carbon monoxide; NO2, nitrogen dioxide; O3, ozone; PM, particulate matter; SO2, sulfur dioxide.
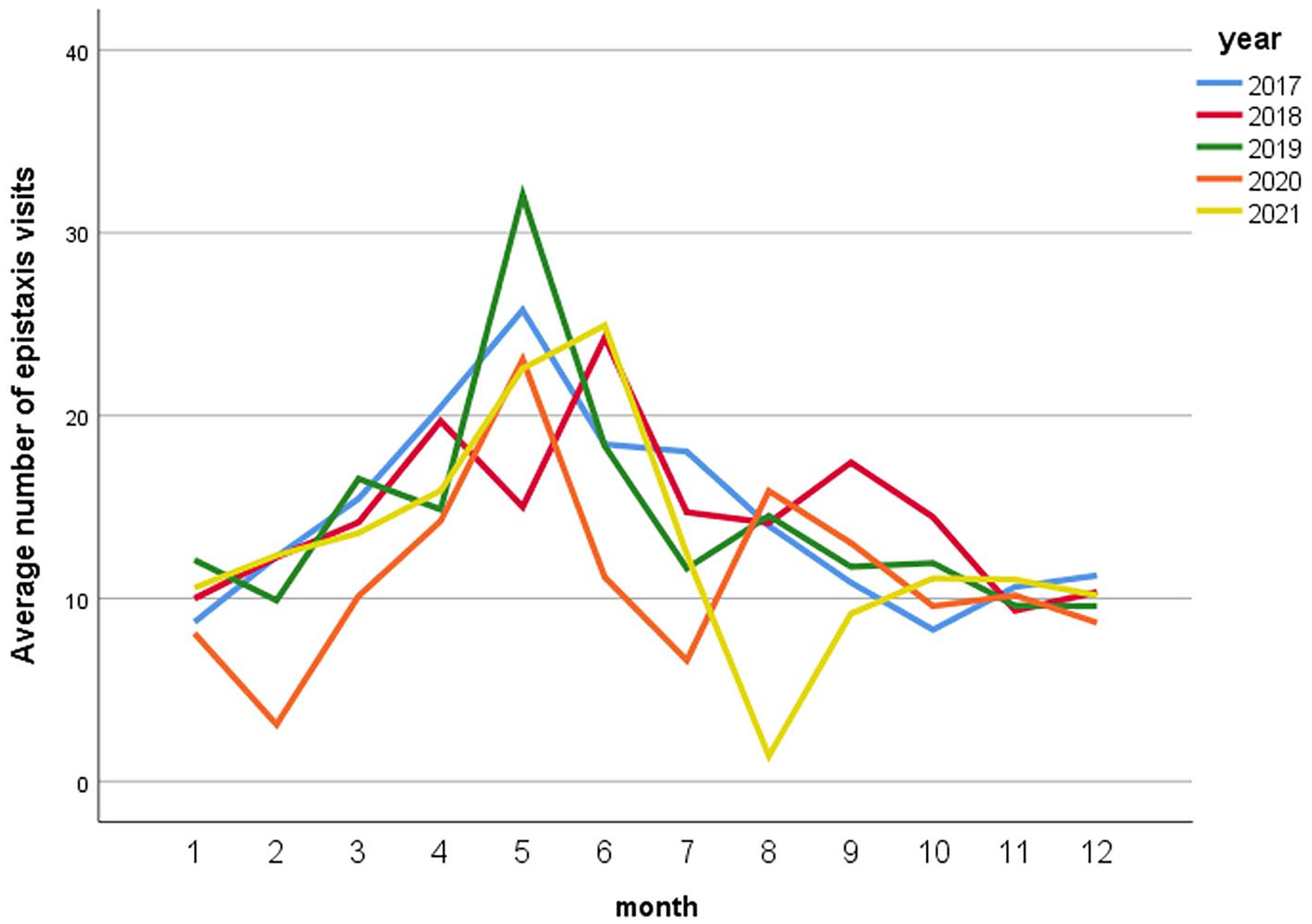
Average number of epistaxis visits per month.
There were significant statistical differences in AQI and the concentrations of 6 types of air pollutants in different months in Yangzhou (P < .05, Table 1 and Figure 3). The concentration changes of 6 kinds of air pollutants in Yangzhou from 2017 to 2021 are shown in Figure 4.
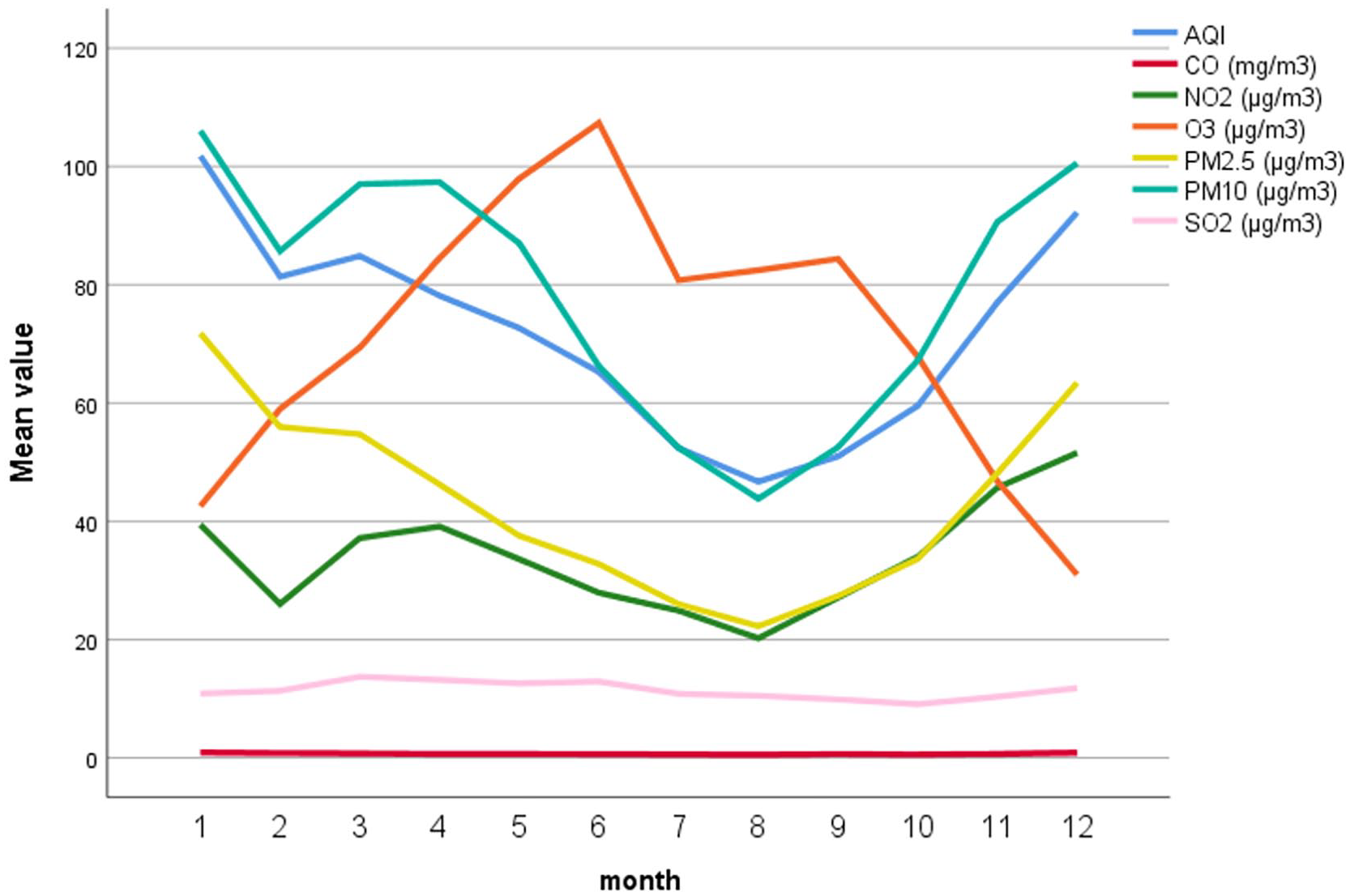
Line chart of AQI and air pollutants. AQI, air quality index.
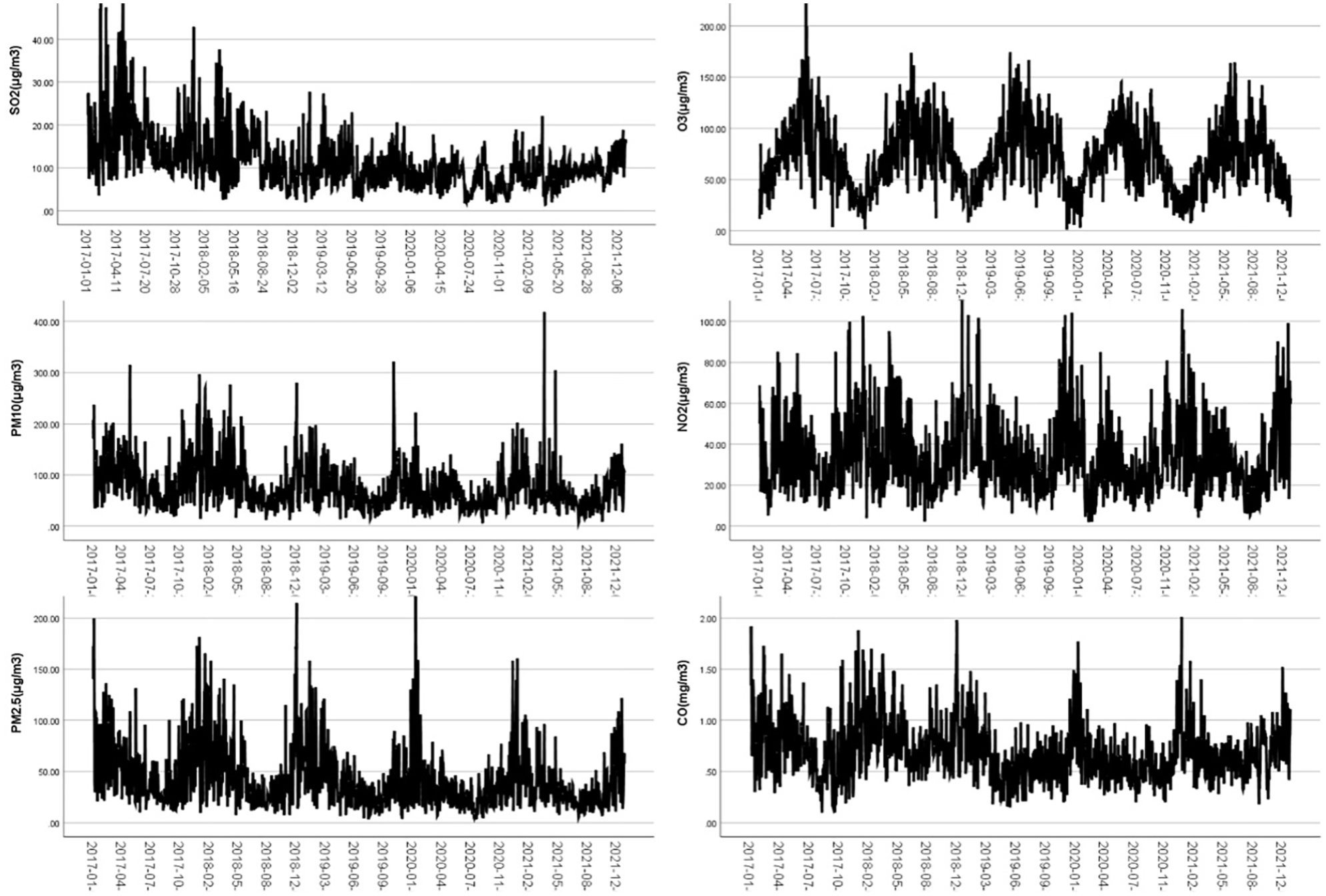
Concentration of Air pollutants in Yangzhou from 2017 to 2021.
Comparison of Different AQI Groups
There were significant statistical differences in the number of daily epistaxis visits between the excellent group and the other 2 groups (P < .05), but there were no significant statistical differences between the good group and the polluted group (P = .155, Table 2).
Comparison of Epistaxis Volume of Different AQI.

Abbreviation: AQI, air quality index.
Correlation Analysis of AQI, Air Pollutant Concentration, and Daily Epistaxis Visits
Analyzed the relationship between the number of visits for epistaxis and the AQI as well as the concentration of air pollutants on the day of visit and the preceding 14 days (Table 3). The results indicated a positive correlation between the AQI and the concentration of air pollutants on the same day (lag0), with the highest correlation coefficient observed for the current day. Moreover, both AQI and air pollutants concentrations showed no significant time lag effects on the number of epistaxis visits.
Time Lag Analysis Between the Number of Daily Visits and Environmental Factors for Epistaxis.
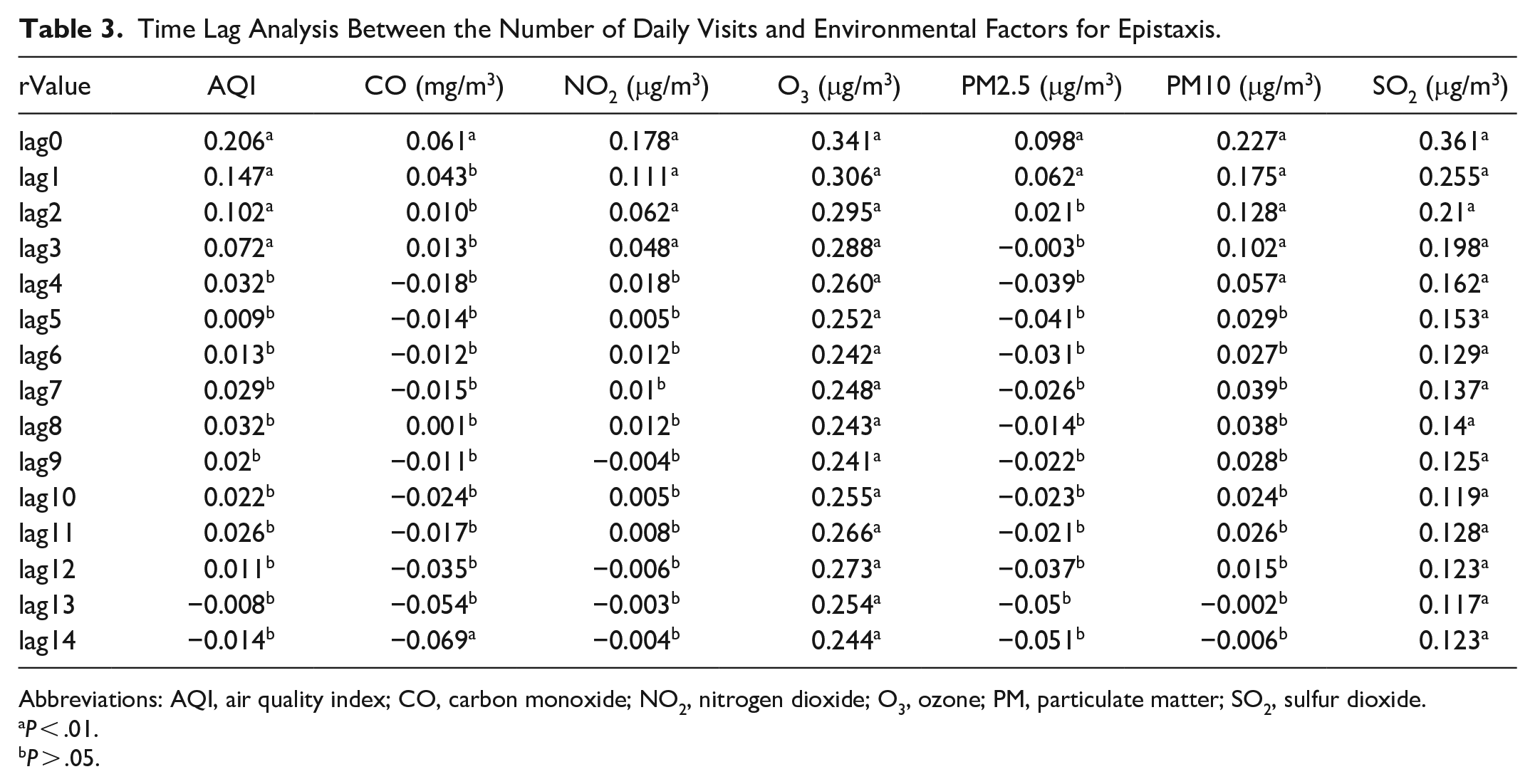
Abbreviations: AQI, air quality index; CO, carbon monoxide; NO2, nitrogen dioxide; O3, ozone; PM, particulate matter; SO2, sulfur dioxide.
P < .01.
P > .05.
Discussion
As one of the common emergencies in otolaryngology, epistaxis can manifest as minor mucous membrane bleeding or significant unilateral or bilateral nasal bleeding, in severe case, it may lead to simultaneous oral and nasal bleeding or even hemorrhagic shock. 2 In recent years, with the continuous development of industrialization and the gradual progress of urbanization in China, the government and even the people have paid more attention to the impact of air pollution on population health. Research have indicated that long-term exposure to air pollution can have adverse effects on human health, particularly exacerbating human respiratory diseases, which are more sensitive to changes in air quality and are seriously affected by air pollution.3,4 Despite this understanding, there remains limited and divergent investigation into the potential impact of air pollution on epistaxis. This article aims to understand the occurrences and regularity of epistaxis in Yangzhou from 2017 to 2021, and to explore the relationship between the number of patients and air pollutants during the same period.
In this study, epistaxis exhibited a higher prevalence among men (62.26%), with the highest frequency observed in the age group of 0 to 17 years (42.33%). Previous studies have also found that men have a higher incidence of epistaxis.5,6 Fishpool and Tomkinson 7 investigated the age and gender distribution of patients with epistaxis admitted to National Health Service hospitals in Wales from April 1991 to December 2009, and found that female menarche seemed to be associated with a decrease in the admission rate of female epistaxis in the age group of 10 to 14 years to 15 to 19 years. The incidence of epistaxis among hospitalized women did not return to the level of 10 to 14 age group until the age of 45 to 49, and steadily increased with men after menopause. Therefore, some scholars suggest that the higher incidence of epistaxis in men may be related to the level of estrogen as estrogen may have a protective effect on the nasal vascular system.7,8 Some studies also believe that it is related to high blood pressure, drinking alcohol, and high blood lipid levels in men, especially middle-aged and elderly men. 9 Contrary to some common beliefs, research indicated no significant correlation between epistaxis and the use of anticoagulants, smoking, diabetes, cardiovascular, and cerebrovascular diseases, instead, it is more closely associated with hypertension, atherosclerosis, and vascular malformation.9–11 This article does not record whether the patients with epistaxis were complicated with hypertension, hyperlipidemia, drinking, etc, which has certain limitations and we can further explore it the later research stage. The prevalence of epistaxis in minors may be related to factors such as low immunity, inadequate diet, nasal and sinus inflammation leading to local mucosal dryness and congestion, capillary dilatation, and mucosal erosion. This study identified noticeable seasonal variations in the incidence of epistaxis in Yangzhou. The number of daily epistaxis visits was the highest in spring, the highest in May, and the lowest in January, and this trend was particularly significant in 2019. The lowest values were observed in February 2020 and August 2021, which were considered to be the COVID-19 epidemic period in Yangzhou. Some studies proposed that winter has the highest incidence of epistaxis, because cold weather leads to the recurrent of respiratory infections, and indoor heating easily cause dry air that affects the nasal mucosa. 12 However, another study showed that the frequency of epistaxis was the same in all seasons. 13 We believe that the seasonal differences are related to local climate and environmental factors.
In this study, there was no significant statistical difference in the number of epistaxis visits in 2017, 2018, 2019, and 2021 (P > .05), but there was a significant statistical difference between the number of epistaxis visits in 2020 and the other 4 years (P < .05). The number of epistaxis visits decreased in 2020 and gradually increased in 2021. We analyze that the decrease in the number of epistaxis visits may be caused by a variety of factors, such as strict containment management in 2020 to restrict the flow of people, strict classification of medical treatment to reduce the number of patients in tertiary hospitals, increased nasal humidity caused by wearing masks, and reduced upper respiratory tract infections to reduce nasal mucosal damage.
The AQI is an important index that can fully reflect the air quality of a region. A larger index indicates poor local air quality and more pollutants in the air, and the calculation of this indicator takes into account many major pollutants such as PM2.5, PM10, SO2, NO2, O3, and CO. 14 AQI is a dimensionless index that is determined by taking the maximum values for air quality subindexes of PM10, PM2.5, SO2, NO2, O3, and CO from the Technical Regulation on Ambient Air Quality Index of China (NO: HJ633-2012) and the calculation method is more complicated.15,16 In this study, the data of daily average AQI are derived from the China Environmental Monitoring Station’s real-time publication platform of urban air quality.
We conducted an analysis of the AQI and air pollutant concentrations in Yangzhou across different months, revealing similar change curves of AQI, PM2.5, PM10, and NO2 concentrations. Among them, SO2 concentration peaked in March, CO concentration reached its peak in January, and O3 concentration in June. The AQI is an index that describes the comprehensive status of urban air quality. According to the value of AQI, the 1826 days can be divided into 3 groups (excellent, good, and polluted), among which the number of days with excellent AQI was the highest, and the number of days with AQI pollution was the least, indicating that AQI in Yangzhou region was predominantly categorized as excellent and good. Statistical analysis showed that there was a statistically significant difference between the excellent group and the other 2 groups in the average daily number of epistaxis visits (P < .05), but there was no statistically significant difference between the good group and the polluted group (P = .155). The average daily number of epistaxis visits in the excellent group was less than in the other 2 groups, suggesting that AQI was related to the amount of epistaxis, and the occurrence of epistaxis when the air quality was good was lower than that in the polluted group. Li et al 17 categorized the number of emergency department patients with epistaxis into otolaryngology departments of hospitals in Hebei and Beijing regions based on AQI values. They analyzed the relationship between AQI values and epistaxis, then discovered that the increased AQI value was a health risk factor for epistaxis. Li et al 18 collected data from emergency department visits for epistaxis in Zhangjiakou City throughout the year 2019, the entire dataset was categorized into 3 levels based on AQI values (AQI ≤ 100, 100 < AQI ≤ 200, AQI > 200), and the study compared the incidence of epistaxis across these AQI levels and observed a significant increase in the occurrence rate of epistaxis with higher AQI values. The aforementioned evidence shows that there is a certain correlation between AQI values and epistaxis, but there is a lack of multicenter research data.
This study aims to explore the relationship between air pollutants and the number of epistaxis visits. Simultaneously, it seeks to determine whether the impact of air pollutants on the epistaxis exhibits a time lag effect. We analyzed the correlation between the number of epistaxis visits from the day of treatment to the previous 14 days and the AQI values, as well as the concentration of air pollutants (Table 3). The results indicated that the number of epistaxis cases on the day of visit (lag0) was significantly positively correlated with AQI and the concentration of air pollutants (CO, NO2, O3, PM2.5, PM10, SO2), with the absolute maximum value of r (r was .206, .061, .178, .341, .098, .227, .361) occurring on the day of visit (lag0). We concluded that daily epistaxis visits in Yangzhou were positively correlated with AQI, CO, NO2, O3, PM2.5, PM10, and SO2. Among them, the concentrations of O3, PM10, and SO2 were highly correlated with the number of daily epistaxis visits. Bray et al 19 analyzed the emergency department visits for epistaxis at St George Hospital during a 5 year period from January 1997 to January 2002, and the study identified a correlation between the increase in occurrences of epistaxis at the hospital and elevated levels of particulate matter and ozone concentration in the air. Li et al 18 showed that the number of emergency epistaxis visits in Zhangjiakou City was positively correlated with the concentrations of PM2.5, PM10, SO2, CO, and NO2, with respective correlation coefficients of .646, .567, .564, .654, and .756, and positively correlated with the concentrations of PM2.5, CO, and NO2, but significantly negatively correlated with the concentrations of O3 (r = −.593). Furthermore, Lu et al 20 collected data from the Department of Otolaryngology of the Capital Institute of Pediatrics from 2014 to 2017, and they conducted a correlation analysis between the number of pediatric patients diagnosed with epistaxis and concurrent concentration of urban air pollutants. They found that children with epistaxis in Beijing differed significantly with age and seasons, and that air pollutants had a certain correlation with the occurrence of epistaxis in children. Kim et al 21 still reviewed the data of 2273 epistaxis cases in a hospital in South Korea during the 1557 days from January 2015 to December 2019 and found that the increase in PM10 concentration in both children and adults were associated with an increase in the number of daily cases of epistaxis. Szyszkowicz et al 22 conducted an analysis of the association between ambient air pollutants with a lag of 0 to 4 days and emergency department visits for epistaxis in Canada. The study revealed that exposure to air pollutants, particularly ozone and PM10, may be associated with the frequency of emergency department visits for epistaxis. The aforementioned evidence collectively suggests a correlation between epistaxis and air pollution, indicating that elevated air pollution levels may contribute to an increased risk of epistaxis.
Particulate matter consists of minute particles in the air, including inhalable particulate matter (PM10) and fine particulate matter (PM2.5), primarily originating from industrial emissions, traffic exhaust, agricultural activities, construction sites, and biomass combustion. Among them, SO2 and NO2 are mainly gases released from the combustion of fossil fuels. CO primarily results from incomplete combustion, such as vehicle exhaust, residential heating, and industrial processes, while O3 is mainly generated through the chemical reaction of nitrogen oxides and volatile organic compounds under sunlight, mainly from vehicle emissions and industrial activities. The mechanisms of epistaxis caused by air pollutants are complex and varied in nature. For example, Calderón-Garcidueñas et al 23 observed that the nasal mucosa of children exposed to air pollutants (such as PM10) for a long time showed basal cell hyperplasia, reduced number of ciliated cells and goblet cells, neutrophil epithelial infiltration, squamous metaplasia, and mild dysplasia. These direct effects on the nasal mucosa are postulated to be associated with the occurrence of epistaxis. The mechanism of air pollution leading to epistaxis may be the following reasons. First, pollutants may directly come into contact with the nasal mucosa, causing irritation. Particularly, larger particulate matter may carry harmful substances, such as chemicals and heavy metals, which can stimulate the nasal mucosa, thereby increasing the risk of epistaxis. Second, pollutants entering the nasal cavity may trigger inflammatory responses, leading to congestion and swelling of the nasal mucosa, thus increasing the possibility of epistaxis. For sensitive individuals, it may also provoke allergic reactions and exacerbate nasal symptoms.24,25 Third, air pollutants may initiate oxidative stress reactions, resulting in cellular damage, mitochondrial damage, and increased vascular permeability, consequently elevating the risk of epistaxis.26,27
The effects of epistaxis involve a variety of local and systemic factors; thus, this study has some limitations. First, our study did not incorporate statistical data from all Yangzhou hospitals, and the results of diverse medical institutions may be different from ours. Second, the exclusion criteria only accounted for patients with nasal trauma, tumor, foreign bodies, oral anticoagulants, and nasal surgery history, but the effects of systemic diseases (such as hypertension, diabetes, arteriosclerosis), upper respiratory tract infection, allergic rhinitis, and other factors on epistaxis were not been analyzed. Third, certain research suggests meteorological factors such as air humidity and temperature are risk factors for epistaxis,5,9,28 and the influence of meteorological factors on epistaxis was not included in this study.
Therefore, by reducing the AQI in daily life, reducing the concentration of environmental pollutants in the air can achieve the purpose of preventing and reducing the incidence of epistaxis to a certain extent.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received the following financial support for the research, authorship, and/or publication of this article. This study was financially supported by Jiangsu Province Natural Science Foundation (BK20201220).