
Abstract
Accessory parotid gland (APG) tumors account for 1% to 7% of all parotid gland neoplasms but are more likely to be malignant than main parotid gland tumors. Management of APG neoplasms entails surgical excision. Four primary approaches to resection have been described in the literature with varying facial nerve outcomes. We report a case of a 4-cm APG pleomorphic adenoma utilizing a transoral approach for excision without postoperative facial nerve injury. A transoral approach is known to mitigate patients’ cosmetic concerns; however, prior reports utilized endoscopic assistance on patients with smaller tumors. We conclude that large APG tumors can be excised through a transoral approach without undue risk to the distal facial nerves, though this transoral approach ultimately may not be appropriate for malignant neoplasms or difficult dissections.
Keywords
Introduction
An accessory parotid gland (APG) represents separate parotid tissue anterior to the mandibular ramus and has a reported prevalence of 32% in the general population. 1 Accessory parotid gland tumors account for 1% to 7% of all primary parotid tumors. Similar to the main parotid gland, pleomorphic adenoma is the most common benign tumor, and mucoepidermoid carcinoma is the most common malignant tumor. 1 However, reports suggest the rate of malignancy is increased (26%-55%) compared to main parotid gland tumors. 1 -3
Diagnosis is based on history, imaging, and fine needle aspiration (FNA). Recommended treatment is surgical excision, with at least 4 incisional approaches described in the literature: direct transfacial, standard parotidectomy preauricular, endoscopic-assisted preauricular, and transoral. 2,3 Although all approaches present varying risks to the facial nerve, no consensus exists regarding facial nerve monitoring or the need for standard facial nerve dissection. 2,3 The purpose of this case report is to present the experience of transoral excision of a large APG tumor.
Report of Case
A 37-year-old male smoker with severe facial and axial furunculosis presented with a 9-year history of a slowly enlarging right facial mass. Noncontrast magnetic resonance imaging (MRI) identified a 4 × 3 cm, well-circumscribed mass 3 cm anterior to the posterior edge of the masseter muscle (Figure 1A and B). Fine needle aspiration diagnosed pleomorphic adenoma.
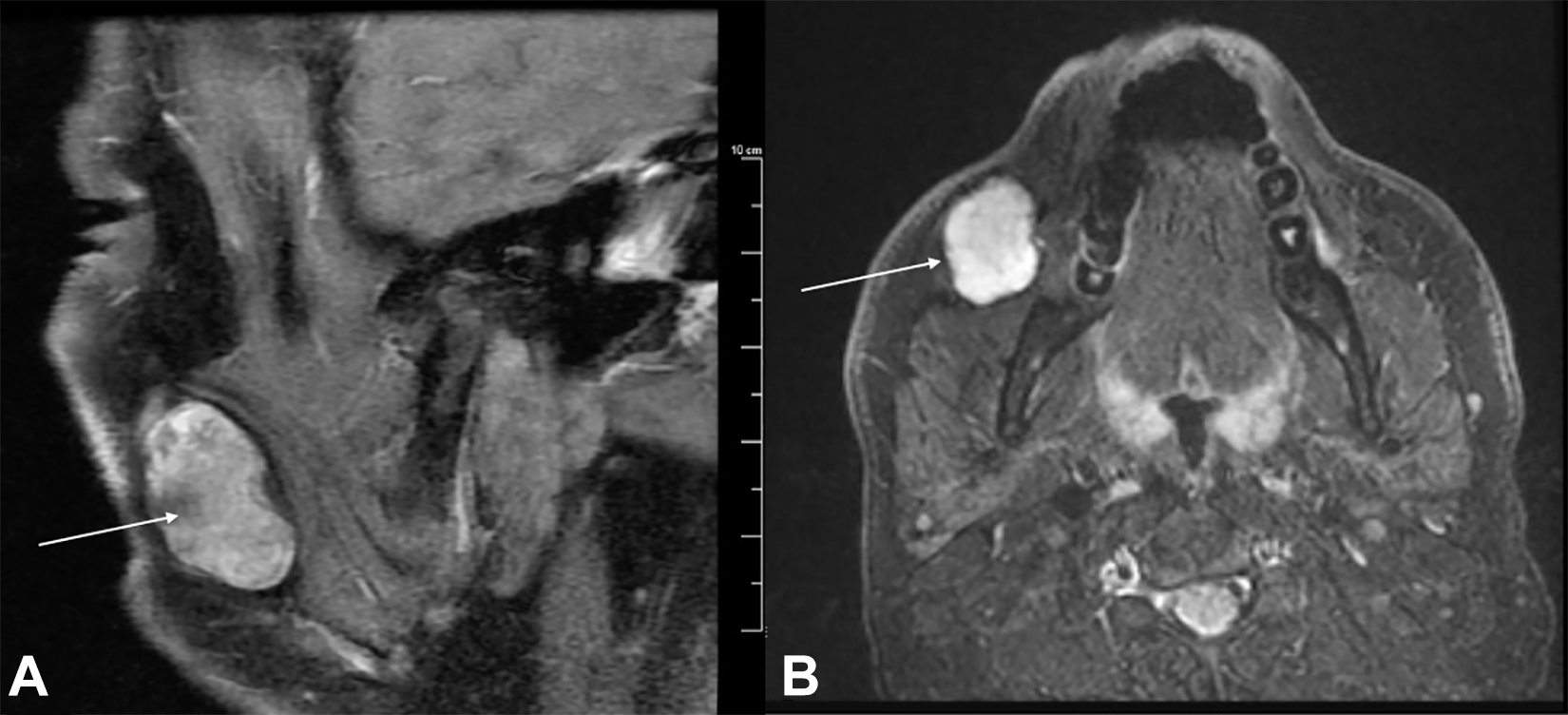
Noncontrast magnetic resonance imaging (MRI) imaging of accessory parotid gland mass (A and B) sagittal and axial MRI sections demonstrate a 4 × 3 cm size buccal mass diagnosed initially by fine needle aspiration (FNA) and confirmed on final pathology to be pleomorphic adenoma.
Transoral incision was made anterior to the right Stensen’s duct papilla and extended inferiorly and superiorly in the buccal mucosa (Figure 2). Following similar division of the buccinator muscle, the mass was immediately identified. As the tumor was dissected free of surrounding tissue, muscle, and the parotid duct, distal branches of the marginal mandibular, and buccal nerves were identified macroscopically and easily preserved. The tumor was pedicled to a region close to an area of stricture in the midportion of the right Stensen’s duct requiring sialodochoplasty upon extirpation. The patient was discharged same day and had an uneventful recovery. Facial nerve function was intact immediately postoperatively and at 2-week follow-up. Final pathology confirmed pleomorphic adenoma (Figure 3).
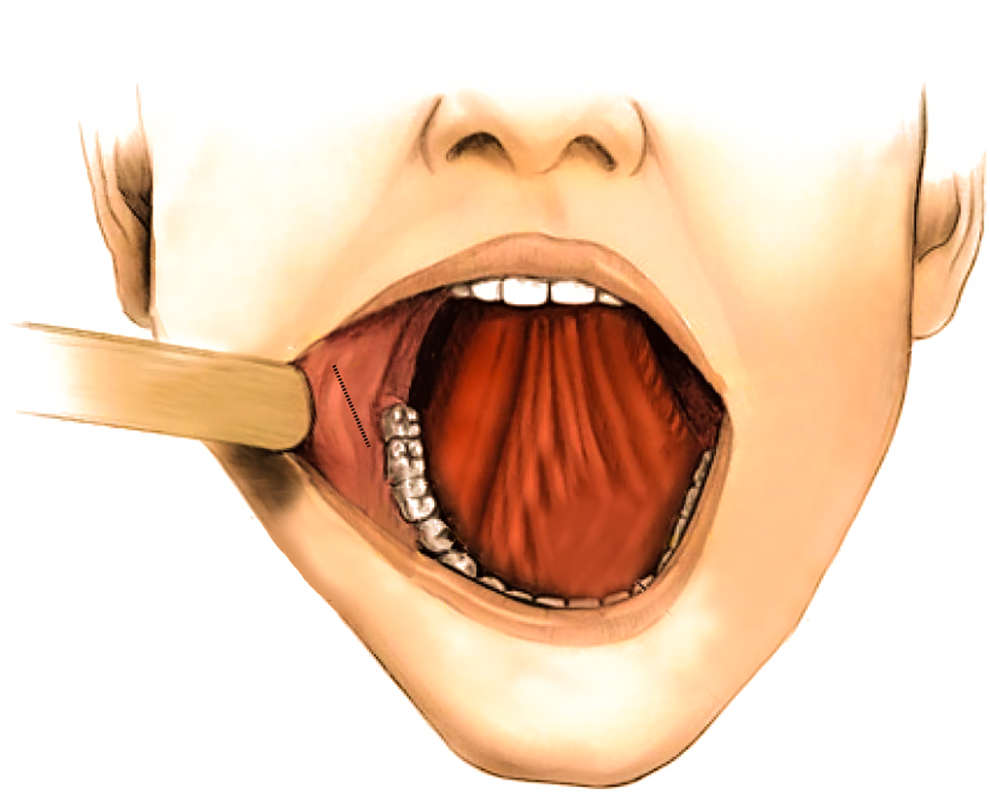
Illustration of transoral approach and exposure the transoral approach offers adequate exposure and visualization for surgical excision of benign parotid gland masses.
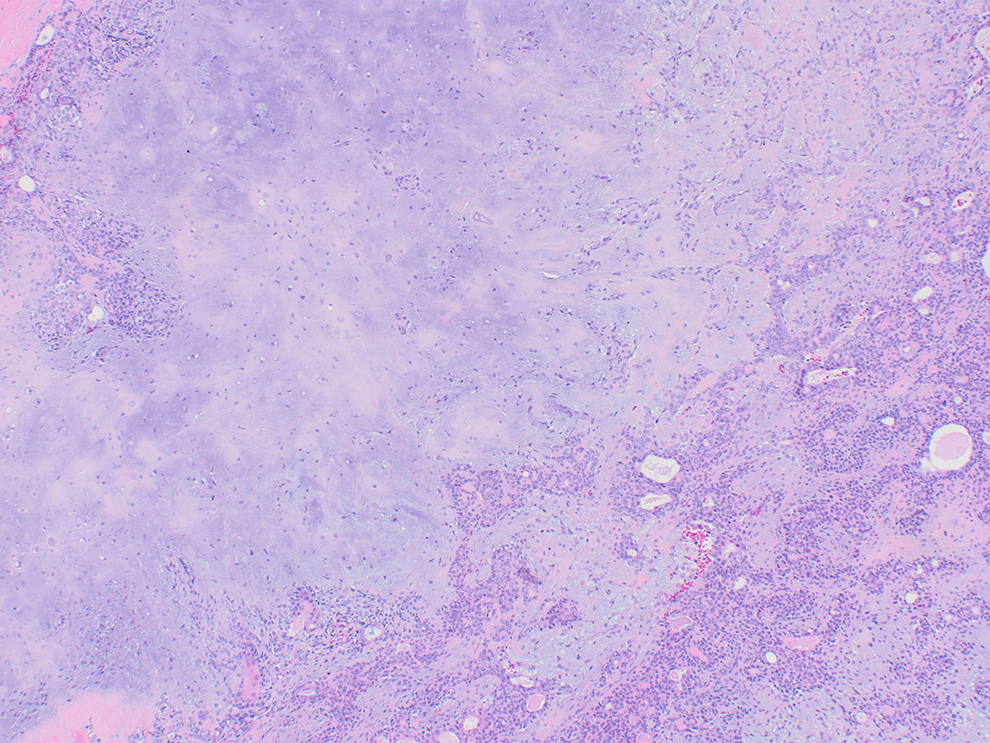
Hematoxylin and eosin stains show ductal structures and anastomosing islands of epithelial cells and myoepithelial cells admixed with myxoid and chondroid areas.
Discussion
Accessory parotid glands are commonly found between and medial to the zygomatic and buccal branches of the facial nerve. 2 In our case, the large tumor size likely propagated a progressive migration inferior to the buccal rami, as evident by duct stenosis. A direct incisional approach over the tumor is reported to have a facial nerve injury incidence of up to 40%, compared to 7% with preauricular incision with or without superficial parotidectomy. 4 Kaneko and Kanai suggest that APGs located on the anterior portion of the masseter can safely be excised transorally without overt risk to the facial nerve. 5
Other concerns include cosmesis and oncological resection. Transcutaneous approaches result in visible scars and tend to leave behind areas of depression from tumor excision, which is obviated with a transoral approach. However, it is unclear if a transoral incision allows for a proper oncological resection as it is common to require endoscopic assistance. 4 Given the benign pathology diagnosed on FNA, the senior author felt the benefit of a transoral approach was significant and counseled the patient appropriately.
Conclusion
In summary, large APG tumors can be excised through a transoral approach without undue risk to the distal facial nerves. In the setting of benign pathology, a transoral incision offers improved cosmetic results but may not be appropriate for malignant neoplasms or difficult dissections.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.