
Abstract
Canalicular adenoma (CA) is a rare benign tumor of the salivary glands, predominantly affecting elderly females, with a strong predilection for the upper lip. While CA commonly arises in the minor salivary glands, its occurrence in the parotid gland is exceptionally rare. In this report, we present a unique case of CA in the parotid gland, adding to the scant literature with only 8 documented instances. The patient, a 57-year-old Asian male, presented with a painless swelling in the left parotid gland that had been persisting for 8 years. Clinical examination and imaging studies identified a lobulated mass, prompting surgical intervention. The patient underwent a superficial parotidectomy, and pathological examination of the excised tissue confirmed the diagnosis of CA, with no signs of malignancy. This case illustrates the diagnostic and management challenges associated with CA, particularly given its rare presentation in the parotid gland. Accurate diagnosis is reliant on surgical biopsy, and careful surgical planning is imperative, especially considering the proximity of the facial nerve. Our case underscores the need for heightened awareness of CA’s unique presentations, particularly within the Asian population. Given the potential for recurrence, long-term follow-up is essential. Further research is needed to elucidate the biological behavior of CA and to refine management strategies for optimal patient outcomes.
Introduction
Monomorphic adenoma, a benign neoplasm of the salivary glands, presents in 3 distinct histological patterns: canalicular, basal cell, and trabeculotubular. 1 Among these, canalicular adenoma (CA) is a notably rare entity, accounting for a mere 1% to 3% of all salivary gland tumors. 2 This subtype predominantly afflicts older women and is characterized by its asymptomatic, gradually enlarging mass, which may occasionally exhibit a multinodular appearance. 3 While CA is most frequently encountered in the minor salivary glands, with a predilection for the upper lip, instances in the buccal mucosa have been observed, albeit infrequently. 3 Its occurrence in the parotid gland is considered exceptionally rare. From a histological perspective, CA is distinguished by its well-encapsulated aggregation of columnar epithelial cells set within a matrix of loose connective tissue. 3 However, to conclusively differentiate CA from neoplasms with similar morphology, such as adenoid cystic carcinoma or low-grade adenocarcinoma, immunohistochemical analysis is often indispensable. 4 The standard approach to managing CA involves surgical excision, which generally yields favorable outcomes, although there is a potential for recurrence. 4 In this report, we detail an uncommon case of CA situated within the parotid gland. To the best of our knowledge, this represents only the eighth instance documented in contemporary literature. 5 Moreover, it appears to be the inaugural case reported within the Asian demographic. 7
Case Presentation
A 57-year-old white man presented at the ENT clinic with a painless swelling in his left parotid gland, persisting for 8 years without signs of inflammation. Six months after onset, he underwent surgical excision, though no surgical or pathological documentation was available. The lesion recurred at the same location a year later, progressively increasing in size but presenting no additional symptoms. His medical history was unremarkable except for this condition. Clinical examination revealed a 3 cm × 4 cm mass at the left mandibular angle, with deep fixation and mobile overlying skin. Facial nerve function remained intact. Ultrasound imaging exhibited a lobulated, heterogeneous heteroechogenity mass within the parotid tissue, measuring approximately 39 mm × 27 mm. Fine needle aspiration (FNA) yielded negative results for abnormal cells. Subsequent magnetic resonance imaging scans delineated a lobulated mass at the anterior border of left parotid gland, with low signal on T1-weighted and high signal on T2-weighted images, measured about 1.9 cm × 3.7 cm × 3.7 cm, alongside postsurgical changes anteriorly (Figure 1). Surgical excision of lesion was performed with superficial parotidectomy (Figure 2). The pathological examination showed complete replacement of normal structure with newly formed capillaries scattered without specific pattern, these newly formed structures were double lined by cuboidal cells, the ducts varied in sizes and contained in some areas eosin substance, the tumor was capsulated, the capsule was intact, neoplastic cells did not reach the capsule, with at least 8 mm free margins (Figure 3). No malignancy was detected, that is consistent with CA.
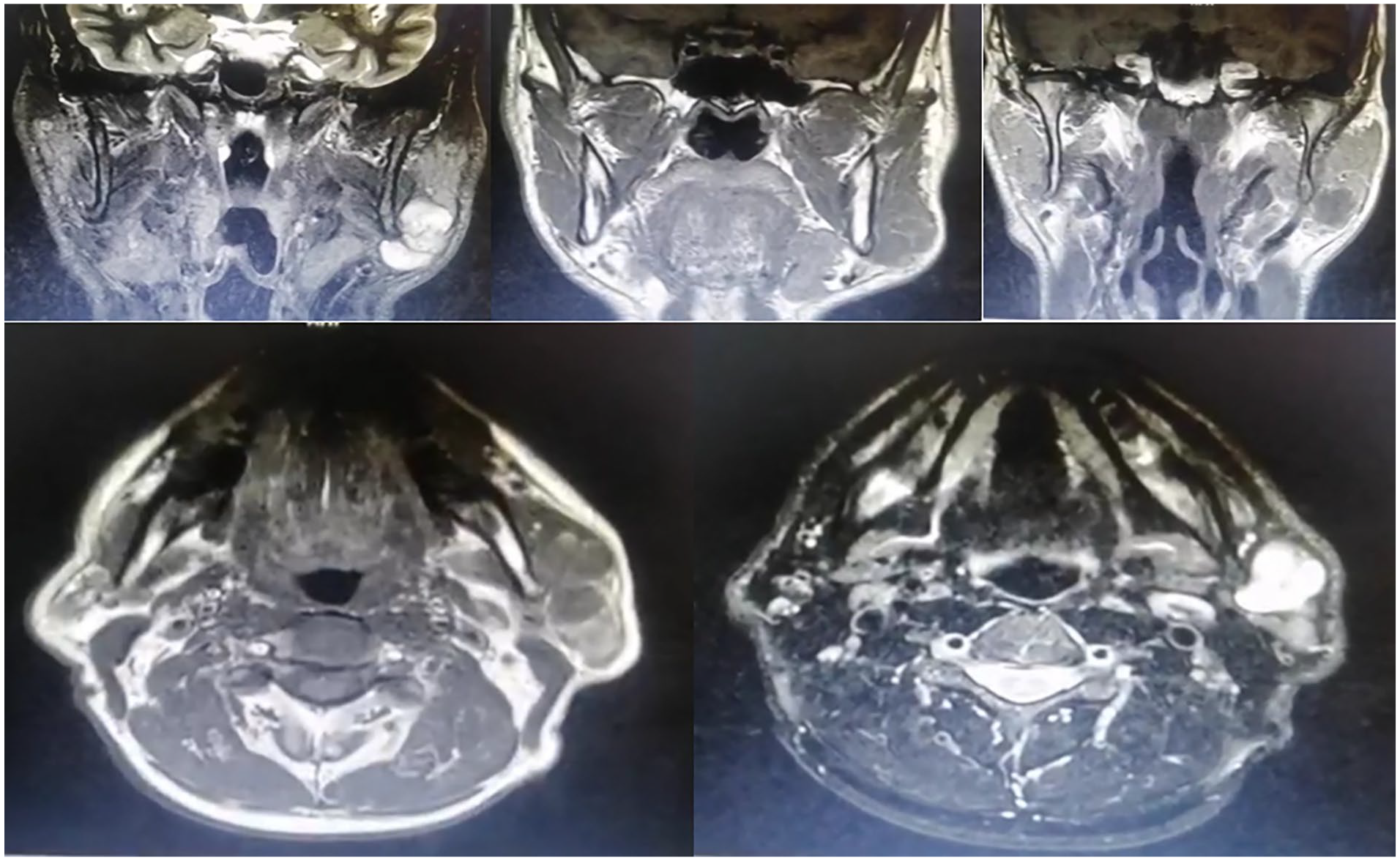
MRI, with coronal and axial planes, shows a lesion on the anterior border of the left parotid, which appears low signal on T1-weighted and high signal on T2-weighted images. MRI, magnetic resonance imaging.
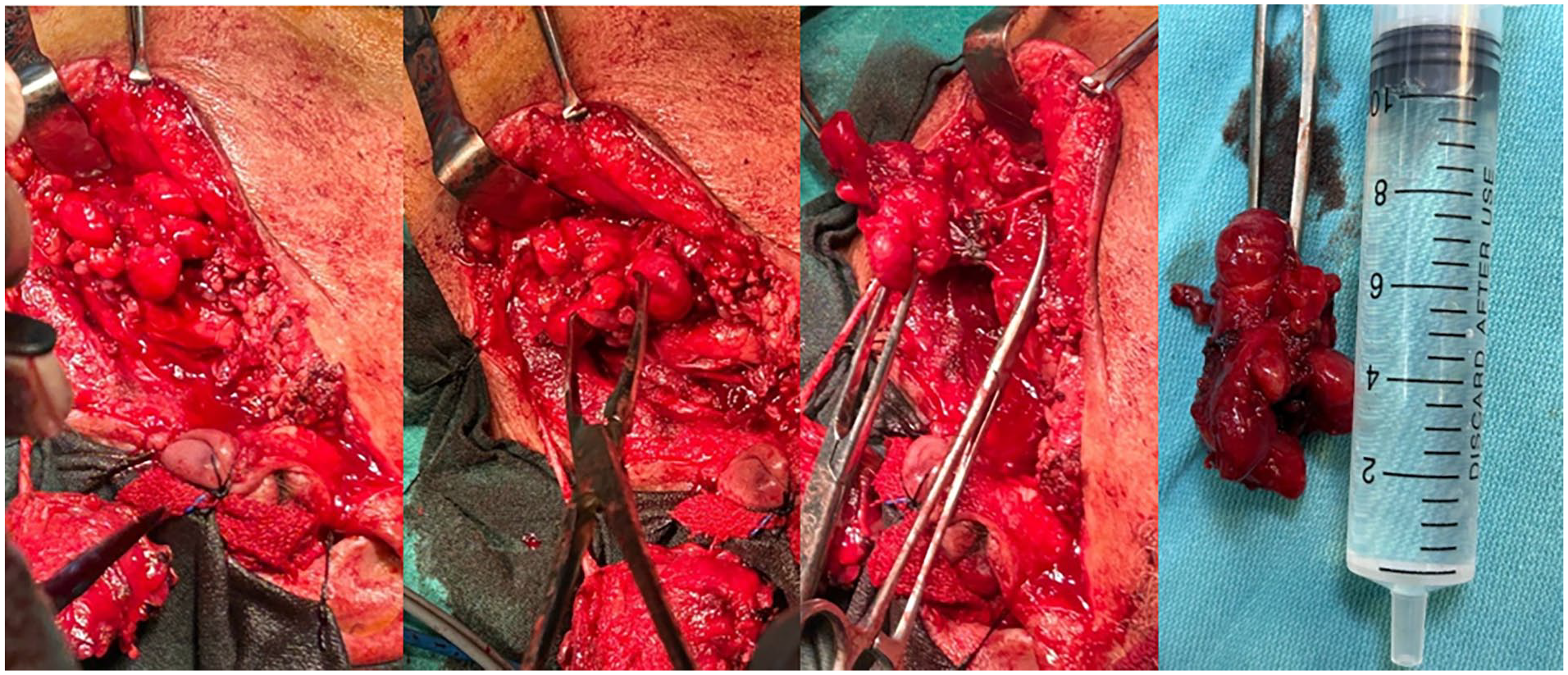
View during and after excision of the lesion.
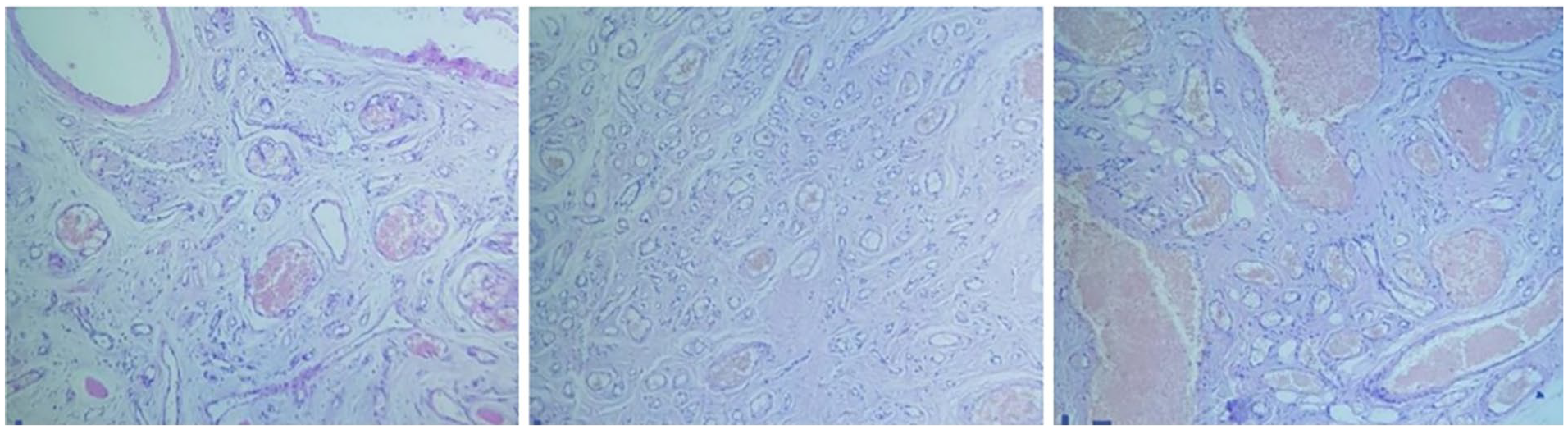
Histological study: where it appears, complete replacement of normal structure with newly formed capillaries scattered without specific pattern, with lined by cuboidal cells, and the ducts varied in sizes and contained in some areas eosin substance.
Discussion
CA accounts for 16.4% of all benign tumors and 9.2% of both benign and malignant intraoral minor salivary gland tumors. It has a female-to-male ratio of 3:2 and rarely presents with cystic features. This tumor predominantly affects the upper lip, followed by the buccal mucosa and palate. 6
Unlike literature in otolaryngology, oral pathology and oncology have extensively covered CA as a benign neoplasm. It predominantly affects elderly women, often involving the upper lip as single or multiple, circumscribed, or lobulated masses. The size typically ranges from 0.2 to 3 cm, with a mean of 1.2 cm, and originates from the luminal cells of the intercalated duct. 2 Notably, there have been no reported cases in the Asian population. 7
Differentiating between benign and malignant salivary gland tumors can be challenging due to their clinical similarities. While FNA and imaging can aid in diagnosis, surgical biopsy remains the gold standard for accurate diagnosis. Detailed examination and immunohistochemistry are crucial, as they can reveal neoplasm infiltration into the parenchyma indicating malignancy, and identify cell types that aid in differential diagnosis.
The parotid gland, distinguished by serous secretory cells and adipose tissue, is unique among salivary glands. The anatomical delineation between the superficial and deep lobes is defined by the facial nerve and its branches. Thus, precise anatomical location is critical for surgical planning. For benign neoplasms in the deep lobe, careful dissection to avoid damage to the facial nerve is essential, underscoring the importance of a meticulous surgical approach and appropriate timing of surgery.
The histopathological features of CA include a bilayered lining of cuboidal to columnar cells adjacent to a single layer of basement membranes, with some eosinophilic cytoplasm and numerous thin-walled blood vessels of varying sizes. In contrast, basal cell adenoma is characterized by hyaline droplets and a thick basal membrane. 8
Our case report presents several distinctive features concerning size, location, race, and comprehensive management documentation. The tumor, measuring 60 mm × 39 mm × 25 mm, was located in the anterior deep lobe of the parotid gland, necessitating a superficial parotidectomy for adequate exposure. The patient, a white Asian male, adds a unique demographic context to this case. Notably, the surgical depictions and biopsies lacked immunohistochemistry, providing a detailed illustration of the management stages without reliance on advanced staining techniques.
Conclusion
This case report highlights the clinical and pathological distinctiveness of CA in the parotid gland, a rare presentation both in terms of tumor type and location. The patient’s clinical course, from the initial appearance of the lesion to its recurrence after surgery and subsequent treatment, underscores the indolent nature of CA and the associated challenges in its clinical management. Despite its benign nature, CA’s potential for recurrence necessitates vigilant long-term follow-up. The successful surgical outcome in this case, marked by the absence of malignancy and preservation of facial nerve function, underscores the importance of meticulous surgical planning and execution. In addition, this report provides valuable insights into the behavior of CA within the Asian population, a demographic that is underrepresented in the existing literature. Future research should aim to expand our understanding of CA’s biological behavior, recurrence patterns, and optimal management strategies to improve patient outcomes.
Footnotes
Data Availability Statements
The data that support the findings of this study are available from the author or corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases. Written informed consent was obtained from the patient for publication of this article.