
Abstract
Keratocystoma of the parotid gland is a rare benign salivary gland tumor. In 2022, the World Health Organization added keratocystoma to the classification of benign parotid tumors. Recently, our hospital encountered a case involving a 2-year-old child, making this the youngest patient reported to date. We excised part of the parotid gland and lesion under general anesthesia while preserving the facial nerve. There was no local recurrence during the 1-year follow-up period after surgery. Despite its rarity, it is essential to consider the possibility of keratocystoma and distinguish it from other benign neoplastic lesions of the parotid gland.
Introduction
Keratocystoma of the parotid gland is a relatively new reported solid tumor first described by Seifert et al (1999), 1 but they initially considered it to be a choristoma. The term keratocystoma was first proposed by Nagao et al (2002), 2 following a histological reassessment of the choristoma initially reported by Seifert et al (1999). In the revised 2022 World Health Organization (WHO) classification of head and neck tumors, keratocystoma was listed as a benign tumor for the first time. 3 Nevertheless, it remains rarely reported and not well understood in clinical practice. To our knowledge, only 13 cases of salivary gland keratocystoma have been published to date (11 literature reports in total). Herein, we present a case of a 2-year-old child who was successfully treated for keratocystoma of the parotid gland. The tumor was surgically resected, and the wound healed well with no adverse complications and no recurrence at the 1-year postoperative follow-up.
Case Presentation
A 2-year and 10-month-old female presented with a left parotid gland mass that had been present for 2 months. The mass had slowly increased in size without causing pain, numbness, growth fluctuations, or facial nerve paralysis, and the patient had no family history associated with this disease. Physical examination revealed a palpable mass under the left earlobe, approximately 2.5 × 2 cm in size, with clear borders. The mass was movable and had a tough texture, with no fluctuating sensation or tenderness. There was an absence of facial nerve paralysis. There was no noticeable redness or swelling at the parotid duct orifice, and clear fluid outflow was visible upon squeezing the mass. No swollen lymph nodes were found in the neck.
Consistently, an ultrasound of the parotid gland showed a hypoechoic mass in the left parotid gland with regular morphology and clear boundaries. A computed tomography scan of the parotid gland revealed a circular mass shadow in the left parotid gland, with a density similar to the surrounding soft tissue and a slightly lower density in the center. There were no apparent swollen lymph nodes in the neck (Figure 1).
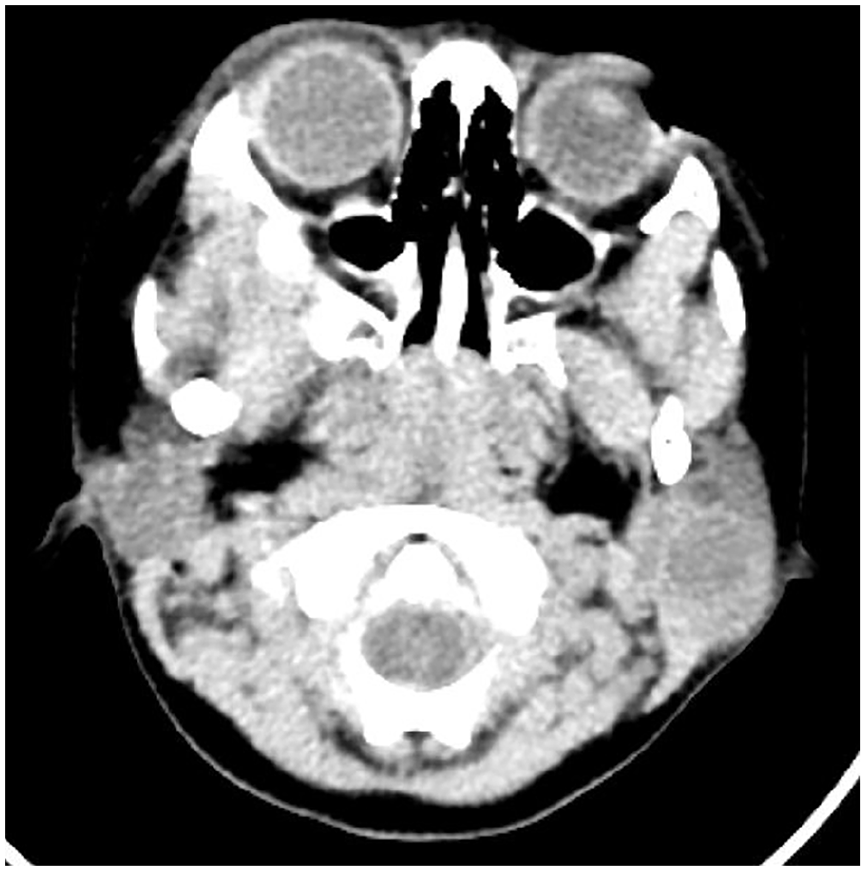
Radiologic view of the tumor in CT. Parotid CT imaging showing a low-density cystic mass in the left parotid region. CT, computed tomography.
Treatment involved the resection of the partial parotid gland and mass while preserving the facial nerve under general anesthesia. The surgical incision healed well in the postoperative period, with no observed facial nerve paralysis. There was no recurrence noted during the 1-year follow-up period.
Macroscopically, the mass appeared as a multilocular cyst with clear borders and contained white sebaceous keratoid material. Histologically, the lesion exhibited a multilocular cystic structure lined with keratinized squamous epithelium. The epithelium showed well-differentiated features with a visible granular layer in some areas and mild cell morphology without obvious atypia. The cyst contents consisted of hierarchical keratins, with solid cell nests of varying sizes observed around the cyst cavity. Foreign-body giant cells and histiocytic reactions were observed in some areas, consistent with keratocystoma morphology. The surrounding salivary gland tissue exhibited chronic inflammation, with acinar atrophy and interstitial collagenization noted in certain areas (Figure 2A and B). Immunohistochemical findings revealed the following results: CK7 (−), Calponin (−), p53 (+, wild type), CK19 (−), p40 (+), and Ki-67 (low, with positivity limited to the parabasal layer of the cyst epithelium) (Figure 2C and D).
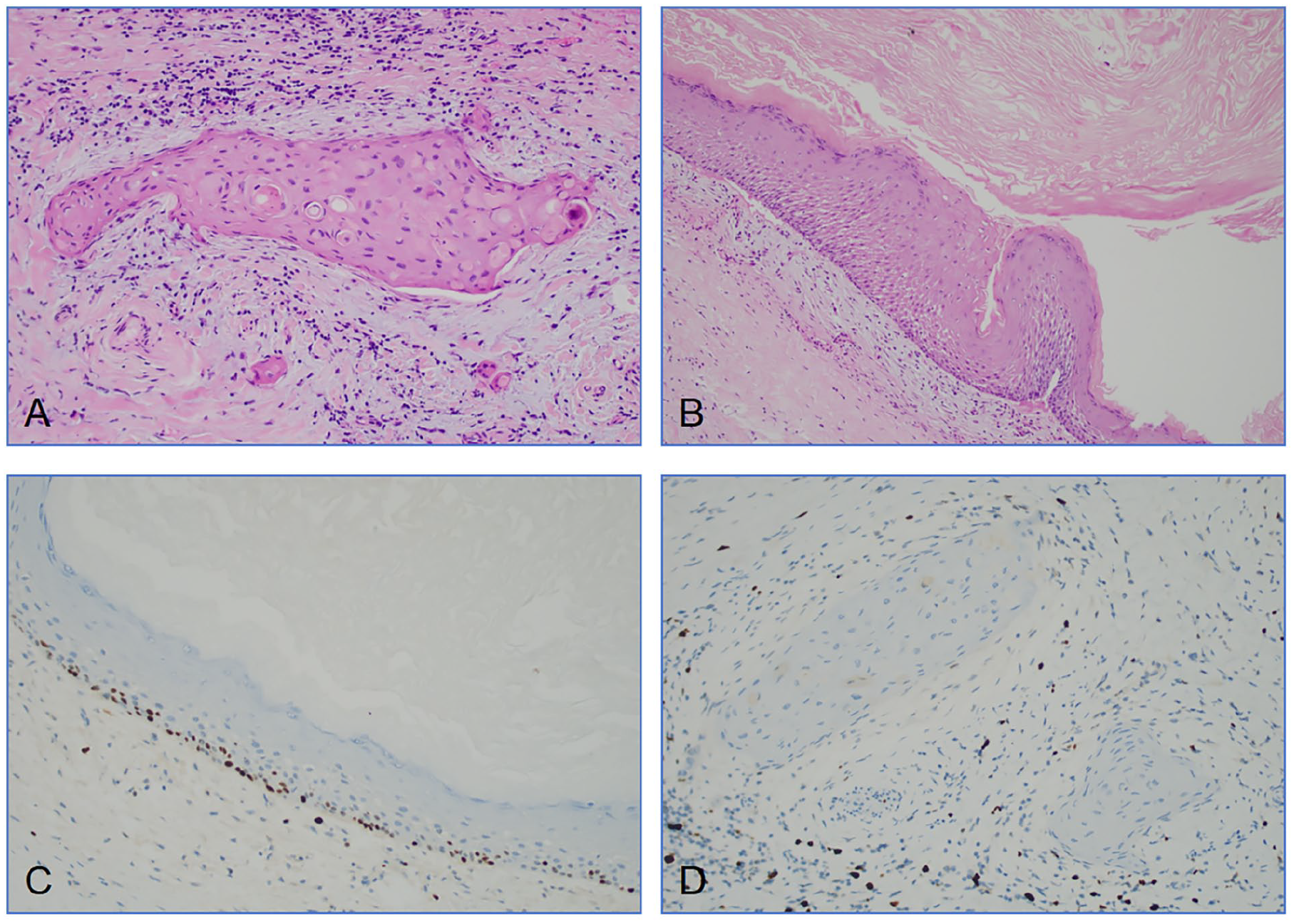
The pathological views of the tumor. (A) Solid cell nests of varying sizes around the cyst cavity, with mild cell morphology and no atypia, unlike squamous cell carcinoma (H&E stain, ×200). (B) The cyst is lined with mature stratified squamous epithelium, with a visible granular layer in some areas. The contents of the cyst consist of hierarchical keratins (H&E stain, ×100). (C, D) The proliferation index marker Ki-67 was low, with positivity limited to the basal layer of the cyst epithelium (immunohistochemical findings of specimen, ×200).
Literature Review
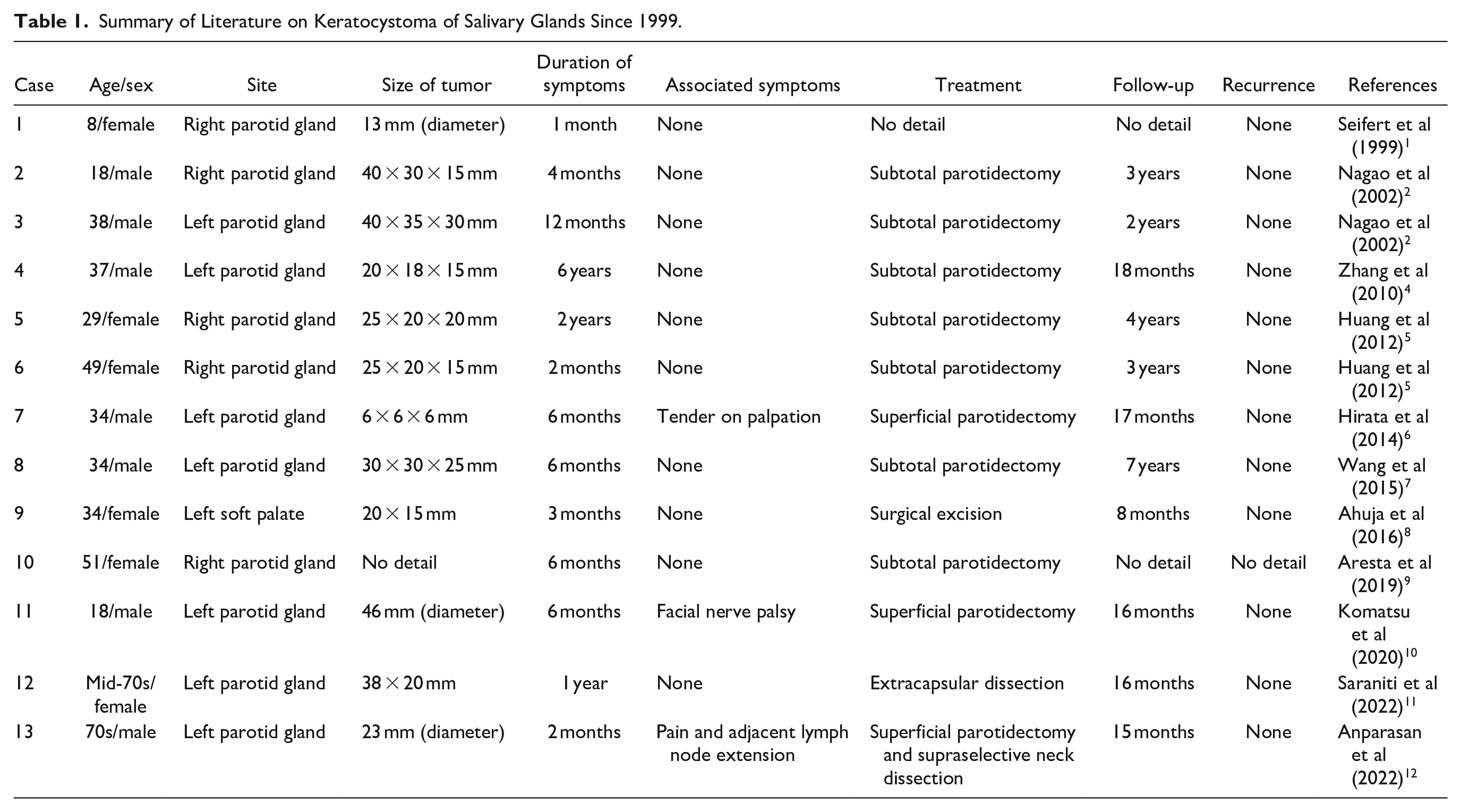
A total of 13 patients with keratocystoma have been reported in the literature to date: 7 males (age range: 18-70 years old) and 6 females (age range: 8-70 years old). The onset sites included 7 cases in the left parotid gland, 5 in the right parotid gland, and 1 in the soft palate (Table 1). All patients underwent surgical resection, and follow-up ranged from 8 months to 7 years, with no reports of recurrence or malignant transformation observed during this period. It is noteworthy that among the reported cases, one patient presented with pain before surgery, another exhibited facial nerve paralysis, and a third experienced pain and swollen adjacent lymph nodes, leading to suspicion of malignant tumors. However, postoperative pathology did not reveal any malignant features in these cases. Notably, the current case involving a 2-year-old child represents the youngest reported occurrence, expanding the recognized age range for diagnosis of this disease beyond previous understanding.
Summary of Literature on Keratocystoma of Salivary Glands Since 1999.
Discussion
Keratocystoma is a rare benign salivary gland tumor, with the parotid gland being the most commonly affected site. 3 Our literature review identified that keratocystoma presents nonspecific clinical and radiographic features, leading to difficulty in differentiating it from other diseases in clinical practice. Its pathology is characterized by a keratinized squamous epithelium lacking granular layers, 2 and its differential diagnosis primarily relies on histopathology. It is crucial to distinguish keratocystoma from well-differentiated squamous cell carcinoma and mucoepidermoid carcinoma, which are malignant tumors. Because once misdiagnosed as a malignant tumor, it may cause serious damage to patients due to radical surgery. Keratocystoma lacks evidence of cytological atypia or squamous cells with abnormal mitotic activity. Furthermore, its low Ki-67 index restricted to the basal layer of the cyst’s inner epithelium and mild cytological morphology differentiate it from squamous cell carcinoma. The absence of concomitant mucinous cells and the presence of extensive keratinization are essential distinguishing features from mucoepidermoid carcinoma.
Due to its rarity, the exact pathogenesis of keratocystoma remains unknown. It has been hypothesized that the tumor may originate from squamous metaplasia of salivary gland ducts. 2 Necrotizing sialometaplasia is a benign inflammatory lesion of the salivary gland that is typically self-limiting and rarely occurs in the parotid gland. 13 Both keratocystoma and necrotizing sialometaplasia share several characteristics: (1) mild nuclear morphology of squamous cells, (2) concurrent metaplasia of ducts and acini, and (3) prominent presence of granulation tissue and inflammatory components. However, keratocystoma lacks lobular infarction or necrosis and does not exhibit typical lobular morphology. Warthin’s tumors may also occasionally present with squamous metaplasia, such as in metaplastic Warthin’s tumors. 14 Nevertheless, keratocystoma lacks glandular epithelium and a large amount of lymphoid stroma, making it distinguishable from Warthin’s tumors. Squamous metaplasia can also occur in pleomorphic adenomas, but keratocystomas lack glandular epithelium, myoepithelial tissue, or mucoid or chondroid stroma, which are distinct features that differentiate them from pleomorphic adenomas.
The absence of granular layers and skin appendages within the cysts are critical criteria distinguishing keratocystomas from benign lesions like epidermoid and dermoid cysts. Other lesions, such as first branchial cleft cysts, can also involve the parotid gland. These cysts typically have walls lined with stratified squamous epithelium, occasionally pseudostratified columnar epithelium, and sometimes a mixture of both. In addition, the fibrocystic wall often contains abundant lymphoid tissue and forms lymphatic follicles. But the first branchial cleft cysts may lack significant lymphoid tissue in the cyst wall. These features help to distinguish them from keratocystomas.
Interestingly, the term keratocystoma can be easily confused with odontogenic keratocyst (OKC). OKC is a common benign cystic lesion of odontogenic origin in the jaw, more frequently found in the upper and lower jaws and rarely occurring in soft tissues. It was first reported by Philipsen in 1956. In 2005, the WHO referred to it as a keratocystic odontogenic tumor, suggesting a potentially tumorous nature for the lesion. However, due to insufficient evidence to classify it definitively as a tumor, the name was reverted to OKC in 2017. The typical histological features of OKC include a connective tissue cyst wall structure lined with an incomplete keratinized stratified squamous epithelium, exhibiting uniform epithelial thickness and lacking epithelial spikes. The basal cell layer is distinctly demarcated, composed of cubic or columnar cells arranged in a palisade-like manner. The spinous layer is thin and poorly differentiated, while the epithelial surface is wavy and often shows incomplete keratinization. 15
A limitation of this report is the relatively short postoperative follow-up period. Despite being a benign tumor, long-term follow-up with clinical and radiological evaluations is recommended to monitor for any potential recurrence or new developments due to its clinical rarity.
Conclusion
In summary, we present a case of keratocystoma originating from the parotid gland of a 2-year-old girl. Keratocystoma of the parotid gland is a rare benign tumor of the salivary gland that can be easily misdiagnosed as other neoplastic lesions. Diagnosis primarily relies on histopathology. Surgical resection is highly effective, with low recurrence rates. This case underscores the importance of considering keratocystoma as a differential diagnosis for cystic neoplastic lesions of the parotid gland to ensure optimal treatment planning for patients.
Footnotes
Author Contributions
L.L.: Case Curation and Original Draft; H.X.: Writing – Original Draft; Y.R.: Writing – Original Draft; X.Z.: Writing – Original Draft; L.B.: Writing – Review & Editing.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
The studies involving human participants were reviewed and approved by the ethics committee of the Affiliated Hospital of Qingdao University. The patient’s legally authorized representatives provided their written informed consent to participate in this study.
Informed Consent
The patient’s legally authorized representatives have informed me and agreed to my surgery and radiographic images in place picture.