
Abstract
Introduction
Warthin tumor (WT) is a frequently reported benign tumor of the parotid gland and is the second most prevalent tumor following pleomorphic adenoma. 1 In recent times, a surge in the incidence of WT has been observed across the globe. Luers et al, in their investigations spanning over two and half decades, demonstrated the upward trend in the incidence of WT compared to pleomorphic adenomas. 13 Their findings indicate a remarkable escalation in the prevalence of WTs, with an increase from 24% of all parotid gland tumors in 1990 to 48% in 2014. 2 Although WT is benign in most cases, it has demonstrated the capability of malignant transformation.3,4 The occurrence of malignant transformation in WT is reported in up to 1% of cases with a higher incidence of squamous and mucoepidermoid carcinomas. 5 There are several synonyms for WT including papillary cystadenoma lymphomatosum, adenolymphoma, lymphomatous adenoma, and cystadenolymphoma. This pathological entity was initially characterized by Dr Aldred Scott Warthin in 1929 and accounts for a significant proportion (14%-30%) of neoplastic lesions that affect the parotid gland. 6 Around 12% to 20% of the WTs are multicenter whereas 5% to 14% of the patients have bilateral WTs. 7 The tumor is rarely diagnosed in patients aged below 40 years (<6%) and is mostly reported in middle-aged and elderly patients (>50 years). 8 Males have a higher predisposition for WT compared to females. It is generally located in the inferior pole of the parotid gland. 9
The diagnostic process for WTs generally involves a combination of physical examination, utilization of imaging modalities, and biopsy investigations. Ultrasound, computed tomography, and magnetic resonance imaging are frequently employed imaging modalities to determine the size and location of the tumor mass. 10 The biopsy is performed to rule out any other potential causes of the mass including cyst or abscess. Furthermore, multiple or bilateral tumors as well as a prior diagnosis of homo or contralateral WT are characteristic of this disease. Fine needle aspiration biopsy (FNAB) is a commonly used minimally invasive method for diagnosing WTs; however, there is controversy regarding its sensitivity and specificity.11,12 The reported sensitivity and specificity by So et al on FNAB were 95.8% and 97.2%, respectively. Surgical intervention is the standard and effective treatment option for the management of WT. The type of surgery may vary depending on the size and location of the tumor, as well as the patient’s age and overall health.13,14 In some cases, the affected salivary gland may need to be partially or completely removed. The adopted surgical methods can include limited resection (partial parotidectomy) or a more extensive approach (total parotidectomy). Although surgical intervention is the main treatment approach for WT, surgical procedure is associated with severe trauma and poorer cosmetic outcomes. The most common complication postsurgical intervention includes infection, salivary fistula, neurological complications, and hematoma. 15 Patients who are unable or unwilling to undergo surgical procedure due to cosmetic concerns or fear of complications can opt for nonsurgical options. WT is also known for its low rate of malignant transformation and recurrence. The aforementioned factors theoretically favor nonsurgical management among the majority of patients. Despite the fact that nonsurgical management has been used for decades for other types of neoplasms, there are few articles investigating similar modalities in patients with WT. With the scarcity of reports regarding nonsurgical management, it will be of great benefit to gather the current literature concerned with the considerations and outcomes of nonsurgical management of WT. Currently, there are several nonsurgical modalities including microwave ablation (MWA), radiofrequency ablation (RFA), and ethanol sclerotherapy for WT. This review will provide a clear view of the validity of conservative management and guide future clinical trials and addresses the following questions:
What is the safety and efficacy of different available nonsurgical treatment option for WT?
In what patient groups, the nonsurgical management options are suitable and can lead to successful outcomes?
Methods
The protocols for this review were devised in adherence to the guidelines prescribed by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). 16
Search Strategy and Data Sources
For this review, comprehensive research was conducted in several databases to find relevant studies that evaluated nonsurgical approaches to the management of WT. The systemic search was conducted in PubMed, Web of Science, Cochrane, and Embase libraries databases. The keyword included: Warthin tumor, adenolymphoma, cystadenolymphoma, papillary cystadenoma lymphomatosum, and lymphomatous adenoma. Furthermore, the search also included keywords indicative of conservative nonsurgical treatment such as MWA, RFA, and ethanol sclerotherapy. For the current search, case reports, case series, cohort, case control, and clinical trials were included. All the articles were inspected and filtered to include articles on nonsurgical management. All age groups of both genders and various demographic characteristics were included in the study. Studies including the comparison between surgical and nonsurgical modalities or reports of non-salivary gland neoplasms were included as well. Articles published before the year 2012, non-English, and mixed methodology articles were excluded from the systematic review. Nonsurgical approaches that were investigated included MWA, radiofrequency, ultrasound-guided ethanol sclerotherapy (UGES), and conservative management.
Data Collection Process
All the matched articles from database searches were transferred to the reference manager (EndNote, 20 Thomson Reuters) with the exclusion of duplicate and non-English titles. Thereafter, endnote file was transferred to Rayyan, a web base software to expedite the initial screening of the search results. 17 The further process was divided into 3 stages: (1) selection of studies based on title and abstract that was eligible for inclusion in the review; (2) thorough analysis of the eligible articles keeping in view the aim of the review; (3) further search was refined based on exclusion and inclusion criteria and data were obtained in form of notes regarding the intervention used in studies, the number of participants, and the methods used.
Flow Diagram
The study design adheres to the PRISMA flow diagram and protocol, 18 outlining the systematic approach from identifying relevant articles to selecting articles that meet the eligibility criteria for further analysis (Figure 1).
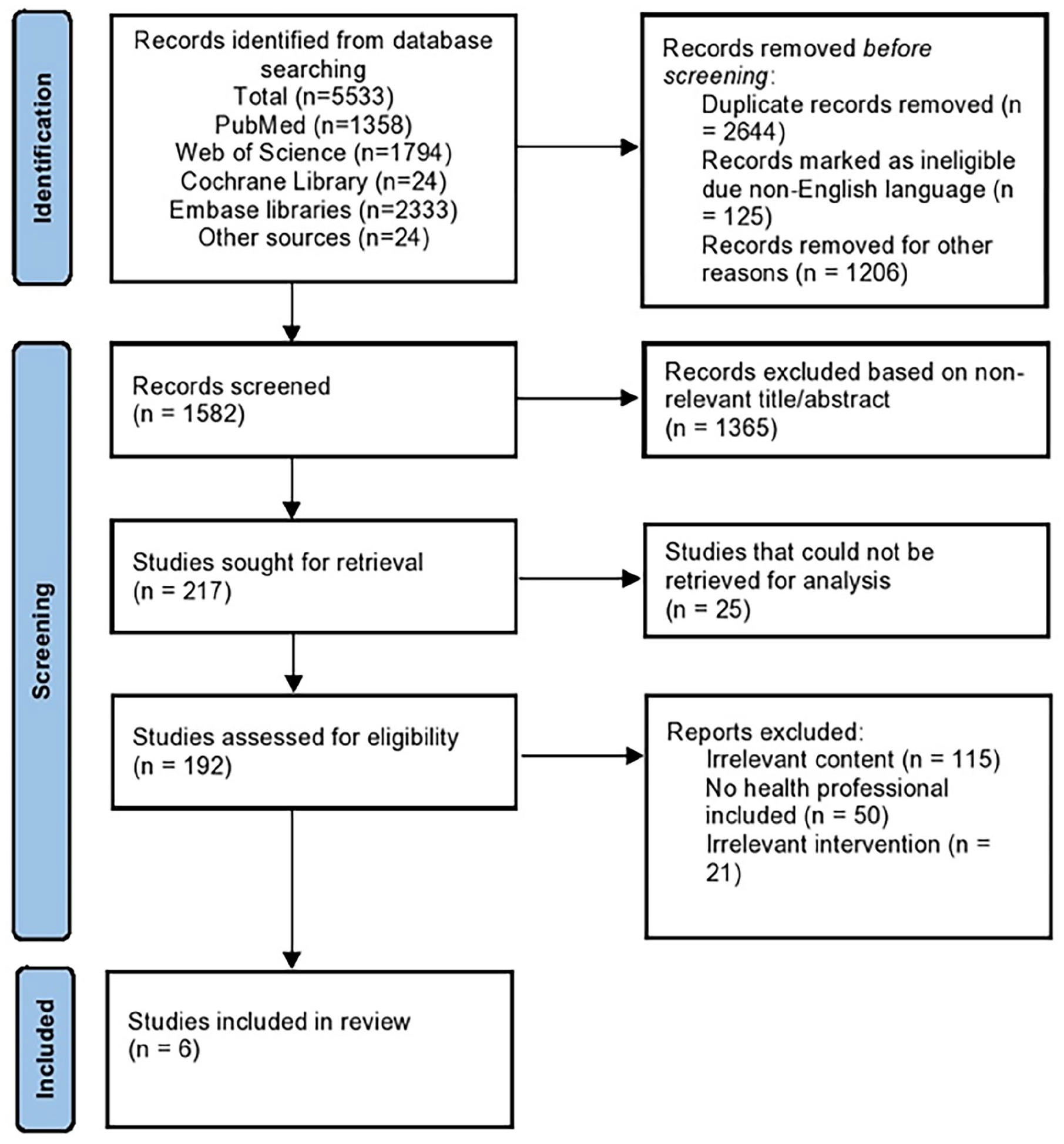
PRISMA flow diagram for systematic review. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Assessment of Methodological Quality
All included articles underwent assessment to ensure the quality of analysis aligned with the research methodology. Discrepancies in viewpoints were addressed through discussions or review by another evaluator. The Joanna Briggs Institute (JBI) critical appraisal tools19-21 were utilized as a dependable resource to assess different study designs such as randomized controle trials, systematic reviews, and observational studies. A summary of the comprehensive analysis results was compiled and presented in Table 1.
JBI Critical Appraisal Checklist.
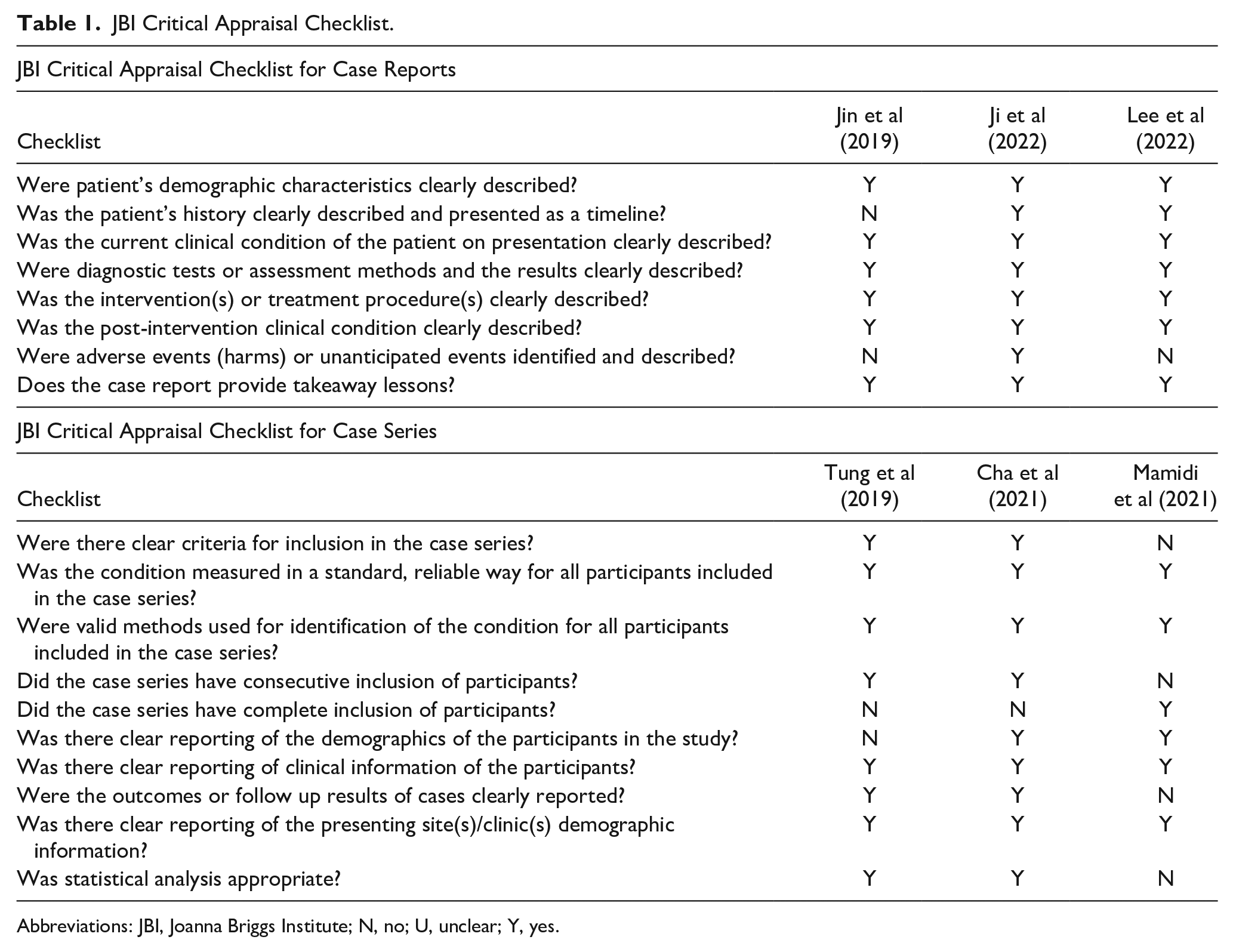
Abbreviations: JBI, Joanna Briggs Institute; N, no; U, unclear; Y, yes.
Results
Included Studies
The literature search provided 5533 potentially relevant articles from PubMed (n = 1358), Web of Science (n = 1794), Cochrane Library (n = 24), and Embase (n = 2333) databases whereas 24 articles were selected from the references area of the relevant articles. After the exclusion of duplicate studies and non-English publications, only 1582 records were further analyzed. Based on keywords and abstracts, 1365 publications were removed from the scope of this review. Of the residual corpus of literature, a thorough assessment was performed to identify the 6 most relevant studies for inclusion in the scope of the current review.
Study Characteristics
In the review, a collective of 21 cases were analyzed from 6 case studies and series, all involving male individuals with an average age of 67. Two cases originated from China, 17 from Taiwan, and 3 from the United States. Among included studies, 2 studies investigated the efficacy of MWA,22,23 2 assessed the safety and efficacy of RFA,24,25 and 2 evaluated the safety and efficacy of UGES for WT management.26,27 The results of the extensive examination of the studies included were summarized and exhibited in Table 2.
Included Studies and Their Characteristics.
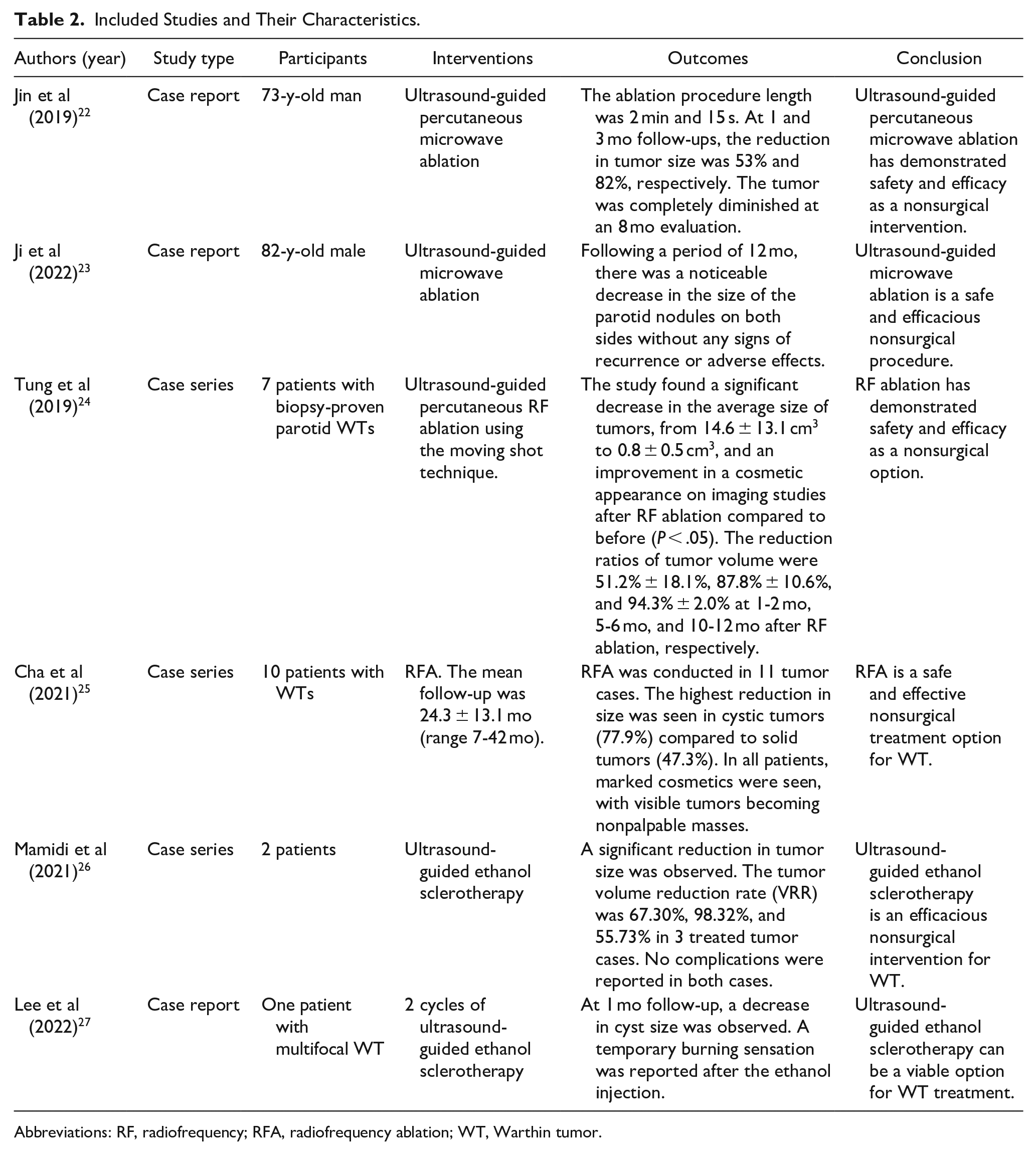
Abbreviations: RF, radiofrequency; RFA, radiofrequency ablation; WT, Warthin tumor.
Discussion
Microwave Ablation
Two studies were identified in the literature that discussed MWA for the treatment of WT.22,23 A study by Jin et al described the successful use of ultrasound-guided percutaneous MWA in the treatment of a parotid gland WT. MWA was carried out using a power output of 30 W, with the microwave antenna inserted into the parathyroid adenoma under ultrasound guidance. The moving-shot ablation technique, combined with ultrasound-guided stratified conformal ablation, was applied. The ablation area’s extent was determined by the echogenic alteration around the antenna, and the process continued until the tumor was completely encompassed by the vaporized region.
During the MWA procedure, there is a potential risk of harming crucial structures in the parotid gland and its surroundings, including the facial nerve, parotid duct, and skin, which could lead to postoperative complications like facial palsy, salivary fistula, gustatory sweating syndrome, insensible earlobe, and skin burns. To address these concerns, they implemented strategies such as injecting saline around the tumor to safeguard adjacent tissues, consistently applying ice saline at the puncture site to prevent skin burns. Moreover, they utilized a moving-shot ablation technique alongside ultrasound-guided stratified conformal ablation to target the tumor effectively while minimizing harm to surrounding healthy tissues. The procedure was performed without any complications and resulted in a significant reduction in tumor volume at both 1 and 3 month follow-ups, with complete resolution of the tumor at 8 months and no recurrence at 2 years. Based on these findings, the authors concluded that MWA is a viable nonsurgical option in patients for which surgery is not a suitable option. 22 Similarly, Ji et al also reported a case of walnut-sized WT in an 82-year-old male patient. The tumor was confirmed by core-needle biopsy as adenolymphoma. The patient underwent ultrasound-guided MWA. At the 12 month evaluation, the volume of WT was significantly reduced without any observable complications. 23 The literature search revealed that MWA can be an option in patients who are older and have multiple underlying comorbidities such as cirrhosis and renal insufficiency. The findings of both case reports are promising; however, further investigation of this approach in larger patient cohorts is required to establish its efficacy and safety profile.
Radiofrequency Ablation
RFA is a minimally invasive medical procedure used to treat a range of pathological conditions by using high-frequency alternating current to generate thermal energy to destroy targeted tissue. 28 This technique utilizes radiofrequency waves to create a field of high-energy electrical current that is delivered via a small, specialized electrode to the affected area. The electrical current causes the tissue to heat up rapidly, leading to cellular destruction through coagulation necrosis which ultimately results in the eradication of abnormal tissue without the need for invasive surgical procedures. 29 The procedure is typically performed under local anesthesia and requires only a small incision to allow the insertion of the electrode into the target tissue. Two case series were found in the literature search.24,25 Tung et al reported a case series of 7 patients with biopsy-confirmed parotid WTs who underwent ultrasound-guided percutaneous RFA under local anesthesia where an electrode was inserted through the posterior-inferior aspect of the mandibular angle, parallel to the maximum diameter axis of the WT. The tumor was divided into several ablation units, with each unit being sequentially treated by moving the electrode tip back and forth, from bottom to top. The ablated area’s size was gauged by the echogenic alterations surrounding the electrode. The ablation process ceased once the entire tumor compartment displayed transient hyperechoic zones. The procedures were completed without any adverse events or complications. Only one patient experienced parotitis with hematoma 12 days after the RFA procedure. Ablation was limited to the tumor capsule without extending into the surrounding parotid gland tissue. Focusing on ablating tissue within the tumor capsule as extensively as possible can aid in reducing tumor size and lowering the risk of facial nerve damage. In addition, the RFA procedure was performed with patients awake, allowing the operator to promptly address any discomfort or paresthesia by adjusting the needle’s position. These factors likely contributed to the absence of facial palsy in the study participants. At 10 to 12 months after RFA, all tumors showed significant reduction, with a mean volume reduction of 94.3% ± 2.0%. 24 In another case series, Cha et al investigated the long-term efficacy of RFA in WTs. They followed up 10 patients for 24 ± 13.1 months. Their findings showed that cystic tumors demonstrated a higher reduction rate in tumor size compared to solid tumors at 1 month (77.9% vs 47.3%) and at 6 months (95.1% vs 80.6%). In their study, all residual tumors were located in the superficial lobes and depicted no increase in size. 25
Ultrasound-Guided Ethanol Sclerotherapy
UGES is a minimally invasive therapeutic technique that involves the injection of ethanol into targeted blood vessels under the guidance of real-time ultrasound imaging. 30 The ethanol injection causes sclerosis of the blood vessel, leading to its permanent closure and subsequent resolution of the associated symptoms. The use of ethanol as a sclerosing agent in this technique has several advantages, including its rapid and complete absorption by the body, low cost, and wide availability. 31 Mamidi et al assessed the efficacy of UGES for the management of WT. They reported that their 2 cases demonstrated a significantly reduced size of WTs including 67.30%, 98.32%, and 55.73% in 3 WT masses. No complication was observed during the management of the patients. 23 In another case study by Lee et al, they represent a case of WT that was managed with partial parotidectomy and 2 cycles of UGES. At 1 month follow-up, a decrease in cyst size was observed; however, temporary burning sensation was reported after ethanol injection. 27
Conclusion
WT is a benign tumor of the parotid gland which has demonstrated the rare possibility of malignant transformation. The tumor is slow-growing, painless, and noninvasive. Diagnosis generally involves a physical examination, imaging modalities, and biopsy investigations. FNAB is a commonly used minimally invasive method for diagnosing WTs, although there is controversy regarding its sensitivity and specificity. Surgical intervention is the standard and effective treatment option for the management of WT. The type of surgery used may vary depending on factors such as the size and location of the tumor, as well as the patient’s age and overall health. The surgical methods can include limited resection (partial parotidectomy) or a more extensive approach (total parotidectomy). However, several minimally invasive techniques such as MWA, RFA, and UGES have shown promising results in the management of WT. These procedures offer a safe and effective alternative to surgery in cases where surgery may not be suitable or preferred by the patient. These techniques offer several advantages, including reduced morbidity, improved cosmetic outcomes, and shortened recovery times. Patients who are unwilling to undergo surgical procedure, older age, and underlying comorbidities are several considerations for nonsurgical treatment modalities. However, further studies are needed to determine the long-term efficacy and safety profile of these techniques in larger patient cohorts. Overall, these minimally invasive techniques provide alternative options for patients who are not candidates for surgical interventions or prefer less invasive treatments.
Footnotes
Acknowledgements
We acknowledge all those who reviewed this study for their valuable insights.
Data Availability Statement
Additional supporting information and search strategy are available for your request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Where applicable, all studies included in this review received ethical approval from relevant institutional review boards or ethics committees, ensuring that research was conducted in accordance with ethical guidelines.