
Abstract
Oropharyngeal stenosis (OPS) is a relatively rare long-term complication of tonsillectomy in children, resulting from the narrowing of the upper aerodigestive tract between the soft palate, pharyngeal sidewalls, and base of the tongue. This is the first reported case of OPS due to significant scar hyperplasia; however, whether it is as prone to recurrence as skin scar hypertrophy remains unknown. In this article, we present the case of a 5-year-old girl who presented to our otolaryngology clinic with sleep snoring and suffocation. Her medical history included tonsillectomy and adenoidectomy, performed 3 years prior to presentation. The patient underwent a combination of surgery and administration of triamcinolone injections, resulting in significant symptomatic improvement. To date, no signs of recurrence have been reported.
Introduction
Tonsillectomy is one of the most common surgical procedures with a relatively low incidence of complications. 1 Among these complications, oropharyngeal stenosis (OPS) is a rare but well-recognized complication, 2 which results from the narrowing of the upper aerodigestive tract between the soft palate, pharyngeal sidewalls, and base of the tongue. 3 The risk factors for OPS include excessive cauterization, significant bleeding, a scar-prone constitution, and deep dissection of the inferior tonsillar poles.4,5 In addition, oropharyngeal infection is a possible pathogenetic cause. The symptoms of OPS include dysphagia, sleep-disordered breathing, and inadequate velopharyngeal function; some patients may be asymptomatic. 5
Cases of OPS following tonsillectomy have occasionally been reported; however, to the best of our knowledge, this is the first reported case of OPS due to significant scar hyperplasia; whether it is as prone to recurrence as skin scar hypertrophy remains unknown. This case highlights the rare complication of OPS caused by significant scar hyperplasia after tonsillectomy, and discusses the current strategies for managing this condition and successfully restoring the morphology and function of the oropharynx.
Case Presentation
A 5-year-old girl presented to our otolaryngology clinic with sleep snoring and suffocation. Her medical history included tonsillectomy and adenoidectomy 3 years prior to presentation. On examination, the bilateral tonsils showed postoperative changes, with a 2.5 cm diameter of the left tonsillar fossa, with a smooth surface and tough new organisms, resulting in significant scar hyperplasia involving the soft palate and anterior tonsillar pillars. Endoscopic examination revealed no recurrence of the adenoids. There was no notable history of extraesophageal reflux. Thorough physical and laboratory examinations revealed no signs of connective tissue or rheumatological conditions such as scleroderma, rheumatoid arthritis, or systemic lupus erythematosus, which could potentially lead to healing irregularities. Radiofrequency ablation of the pharyngeal mass was planned for OPS treatment.
The surgeries were performed under general anesthesia, using a Davis retractor to ensure adequate exposure. The patient was positioned similarly to that in the standard tonsillectomy procedure. A plasma device (Gaoton Medical) was used to remove the pharyngeal mass located between the soft palate and tonsil fossa along the new biological base of the palatoglossal arch (Figure 1). Enlargement of the pharyngeal cavity was observed after resection (Figure 2).
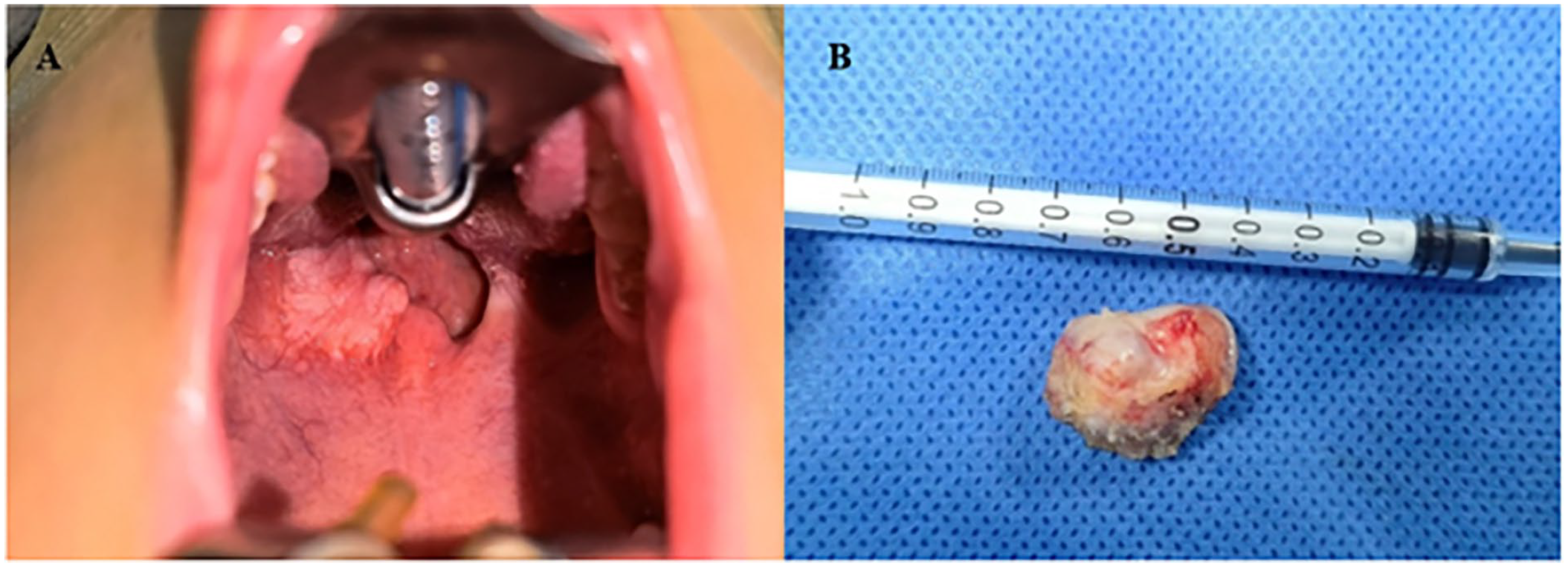
A: Intraoperative examination revealed significant scar hyperplasia in the oropharyngeal region, which obstructed the airway. B: Significant scar hyperplasia tissue specimen.
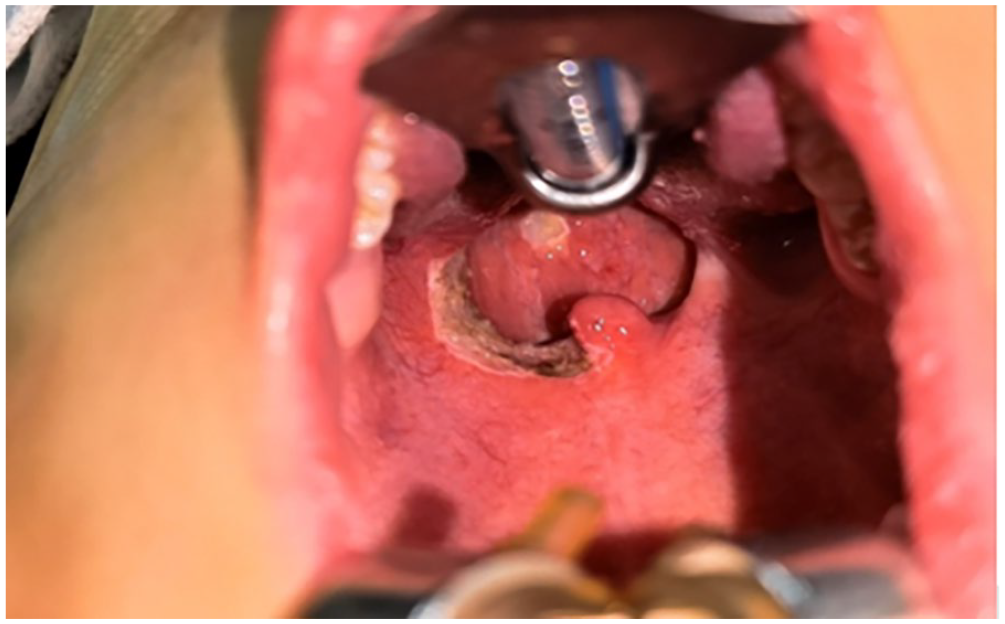
Pharyngeal presentation following the resection of significant scar hyperplasia.
Following the surgery, a 40 mg dose of triamcinolone was injected into the lateral pharyngeal tissues and base region, with approximately 0.1 to 0.2 mL injected at each location. The patient commenced a liquid diet on the first postoperative day, and experienced effective pain management, with no complications during hospitalization. Pathological examination of the pharyngeal mass revealed hyperplasia and degeneration of the submucosal fibrous tissue (Figure 3). Immunohistochemical findings were as follows: S-100 (−), SMA (−), MSA (−), SOX-10 (−), desmin (−), CD31 (vascular+), CD34 (vascular+), and Ki-67 (+, 1%). Direct laryngoscopy performed 1 month after surgery showed a well-healed oropharynx with improved stenosis. The injections were repeated once a month to prevent a recurrence. Patients were followed up monthly for 6 months after the aforementioned therapy, and there was no evidence of recurrence.
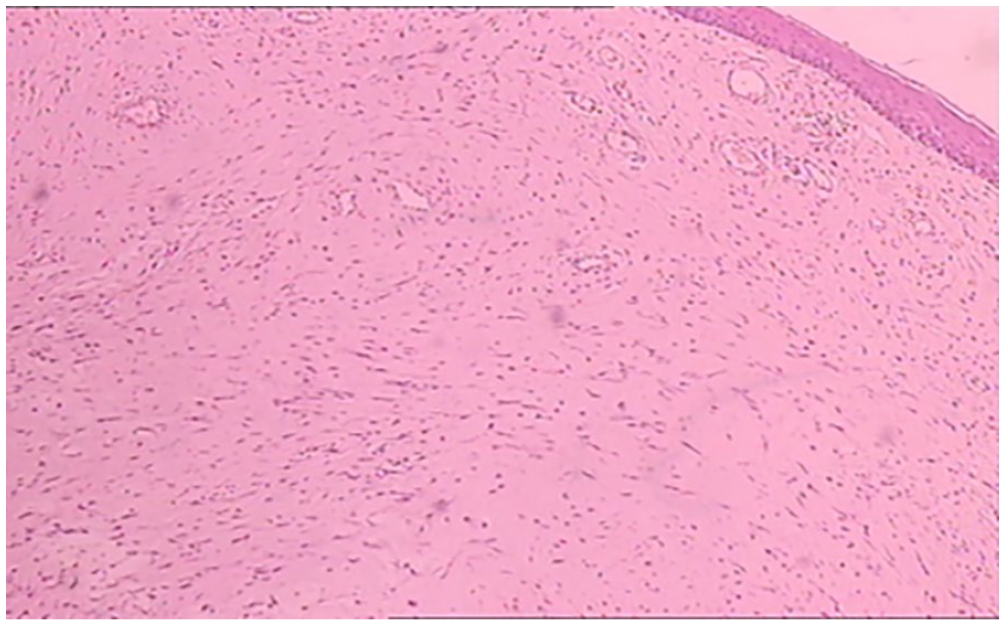
Pathological findings of the pharyngeal mass. The histopathological section reveals hyperplasia and degeneration of the submucosal fibrous tissue.
Polysomnography (PSG) performed before the initial tonsillectomy in 2020 revealed an apnea/hypopnea index (AHI) of 5.7 events/hour. Following tonsillectomy, PSG indicated a noteworthy reduction in AHI, with a reading of 1.9 events/hour. Given the relatively mild initial AHI and observed improvement reported by the patient and her family, PSG was not needed during the perioperative period.
Discussion and Conclusion
Tonsillectomy is a frequently performed surgical procedure in otorhinolaryngology and the preferred treatment for pediatric obstructive sleep apnea (OSA). 6 The most common cause of OPS is uvulopalatopharyngoplasty, followed by lingual tonsillectomy, and oropharyngeal cancer radiotherapy or surgery.7-9 OPS is a relatively rare long-term complication of tonsillectomy in children. There have been some reports from abroad, such as cases in which fibrosis after tonsillectomy led to OPS, 10 or cases that occurred after transoral robotic surgery.11,12 However, the OPS reported in this case was caused by significant scar hyperplasia after tonsillectomy and is a relatively rare clinical case. Although the patient had a history of multilevel airway surgery, simultaneous nasopharyngeal stenosis was not observed. When further considering the possible causes of OPS in relevant surgeries, attention should be paid to the following points: fully understanding the surgical indications; actively controlling infection during the perioperative period; continuously improving surgical skills, including the correct and appropriate selection of energy instruments; dividing along anatomical gaps; reducing intraoperative bleeding; and paying attention to the surgical resection area. Patients should be encouraged to perform mouth rinsing, tongue extension, and mouth-opening exercises as soon as possible after surgery. It is crucial to reduce the destructive complications and associated comorbidities that patients may experience owing to OPS.
Many procedures have been proposed to alleviate OPS, including surgery and triamcinolone injections alone or in combination, postoperative laser vaporization, manual dilation, and pharyngeal stricture tissue expansion. 13 McLaughlin et al 5 concluded that triamcinolone injection alone could be an adequate treatment for OPS. They recommended horizontal-vertical pharyngoplasty for severe cases of OPS that did not show improvement with triamcinolone injection alone. Flap reconstruction is a viable alternative when wide resection is required to treat oropharyngeal stenoses. Local flaps such as Z-plasty repair and buccal mucosal or facial artery musculomucosal flaps are the first options available in cases of small to moderate defects.14-18
However, given the infrequency of such cases and the limited exposure of surgeons to this particular challenge, there is no widespread agreement regarding the optimal treatment for OPS caused by significant scar hyperplasia.
Given the large volume of keloids and recurrence of OSA symptoms, local excision of the keloids and multipoint injection of triamcinolone acetonide at the base of the keloids may restore airway patency and reduce the likelihood of recurrence. There are similar reports on related treatments; surgery combined with an injection of triamcinolone acetonide is better than surgery alone and achieves good results.2,5 This may be related to the direct inhibitory effect of triamcinolone acetonide on fibroblast DNA, which can inhibit granulation tissue formation, reduce collagen synthesis, reduce collagen inhibitor levels, and increase collagen degradation, thus exerting therapeutic and inhibitory effects on scars. 19 Some studies have reported that mitomycin C can be used as an adjuvant therapy for scar tissue and may also play a role in reducing scarring and recurrence. 20 However, further research is required in this area.
OPS is a rare but serious long-term complication of tonsilloscopy. We propose a simple and effective treatment for OPS caused by significant scar hyperplasia of the oropharynx. A combination of these strategies allows for the restoration of pharyngeal airway patency. We are cautiously optimistic regarding our current outcomes and will continue to follow our patients closely.
Footnotes
Author Contributions
ZTF and WXD conceived and wrote the report; XXW, TQ, and YTW organized the data; ZTF, JRL, and CBL revised the manuscript. All authors have read and approved the final version of the manuscript.
Data Availability
The data supporting the findings of this report are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Xingtai Science and Technology Plan Project [Grant Number 2018ZC199].
Ethics Approval
Approval was obtained from the Ethics Committee of the Hebei Eye Hospital (Approval Number: 2023LW06). This case was performed in accordance with the principles of the Declaration of Helsinki.
Informed Consent
Written informed consent was obtained from the patient’s guardians for the publication of this case report.