
Abstract
Objective
This study presents a novel classification of the anatomical subsites of the tonsillar fossa and discusses their associations with post-tonsillectomy hemorrhage (PTH) after extracapsular tonsillectomy.
Materials and Methods
Coblation tonsillectomy was performed on three adult cadavers and the anatomical subsites of the tonsillar fossa based on the distribution of the tonsillar feeding artery: the upper pole (subsite A), most of the tonsil body (subsite B), the inferior tonsil body (subsite C), and components of the lower pole (subsites D and E). Extracapsular tonsillectomy was prospectively performed using various surgical techniques and PTH was evaluated.
Results
A cadaveric study revealed that the intra- and extra-capsular vessel topographies were essentially identical. Although the demarcation lines varied either up or down by a few millimeters, the arterial vascular network was particularly dense at subsites D and E, and the vessel diameter at these subsites was significantly greater than at subsite C and also (especially) at subsite E. Of 680 patients who underwent tonsillectomy, PTH developed early in 13 (31.7%) and late in 28 (68.3%). Surgical interventions were required by 29/41 patients (70.7%). Subsites D and E were the most common subsites of late PTH and PTH that required intervention. Such intervention was rarely necessary when PTH developed at subsite A or B.
Conclusions
The new classification of the anatomical subsites of the tonsillar fossa aids inexperienced surgeons and provides an anatomical rationale for variation in surgical technique that minimizes vascular injury, thus improving safety.
Introduction
Post-tonsillectomy hemorrhage (PTH) is a major life-threatening complication of tonsillectomy and significantly increases the medical cost. Cold steel dissection was previously the main technique used for tonsillectomy, but it has gradually been replaced by diathermy due to the recent advancements in medical technology, including coblation and bipolar and monopolar electrocautery.1-3 However, despite advancements in technology, PTH remains a significant risk.4-13 Previous studies have identified the inferior tonsillar pole as the most common PTH site.8,9,12,13 However, the reason for the increased PTH risk at the inferior tonsillar pole is unclear. We speculated that PTH may be associated with certain anatomical subsites of the tonsillar bed and vessel topography. To the best of our knowledge, few previous studies have evaluated the association between tonsillar fossa subsites and PTH. This study employed endoscopic cadaveric dissection to develop a novel classification of the anatomical subsites of the tonsillar fossa and explored the relationships between such sites and PTH after extracapsular tonsillectomy.
Materials and Methods
Ethical considerations
The study protocol was approved by the Institutional Ethical Review Board of Yiwu Central Hospital, China. Informed consent was obtained from all participants or their parents.
Methods
The prospective design
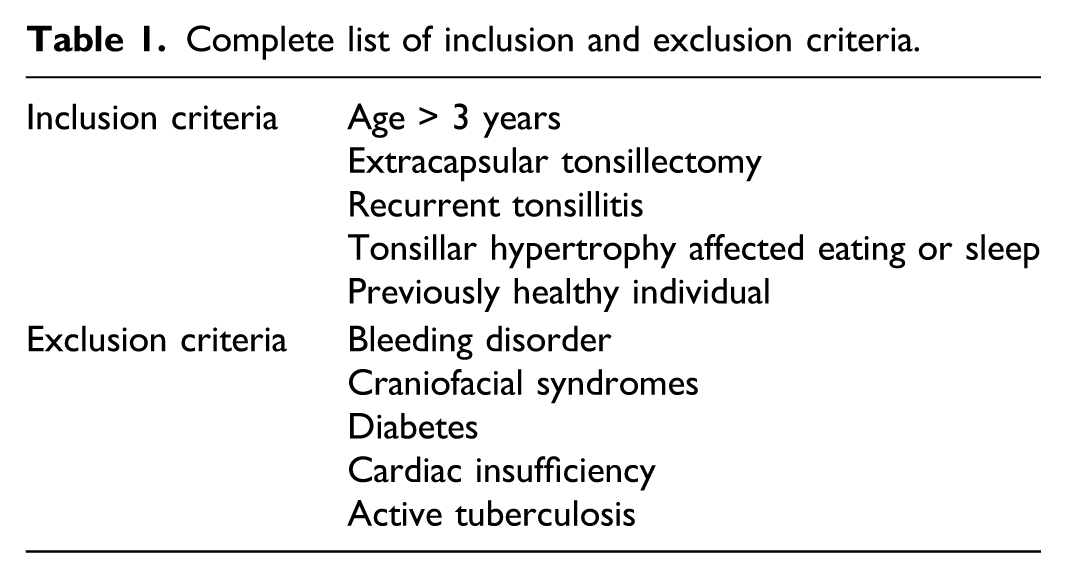
Complete list of inclusion and exclusion criteria.
Age, sex, body mass index (BMI), and surgical indication, technique, and complications including PTH and bleeding site were recorded. PTH was defined as the need of compression hemostasis, medical treatment, surgical intervention, and/or blood transfusion. Any hemorrhage that required only clinical observation was excluded. Early PTH was defined as hemorrhage within 24 h of surgery, while late PTH was defined as hemorrhage after 24 h of surgery. BMI (kg/m2) was calculated as weight (kg)/height2 (m2) and categorized into underweight (low BMI), normal weight (normal BMI), overweight (elevated BMI), and obesity (high BMI), according to the revised Asia-Pacific BMI criteria by the World Health Organization. 14
Treatment allocation was performed by the principal investigator with the aid of a registered nurse using simple random sampling. Specifically, consecutive subjects who met the inclusion criteria and signed consent forms were assigned random numbers generated by SPSS for Windows software (ver. 19.0; SPSS Inc., Chicago, IL, USA) that allocated them into groups who underwent cold steel, monopolar diathermy, or coblation dissection. All surgeries were performed by (different) senior surgeons. Cadaveric dissections of halved head-and-neck regions and classification of tonsillar subsites preceded all surgeries.
Cadaveric dissection
Halved head-and-neck regions of three adult cadavers with no macroscopic pathologies were used. The bilateral tonsils were removed via coblation. Also, portions of the pharyngeal walls, thus from the soft palate to the tongue base, were removed. These included the upper poles of the tonsils, the tonsillar beds, the triangular folds, the pharyngeal muscle layers of the tonsillar beds lateral to the tonsillar capsules, the intact capsules, and the vessels exterior to the capsule. All cadavers were endoscopically examined by the same surgeon. The specimens were not sectioned, and the vessel calibers were not measured.
Anatomical classification of tonsillar subsites
The tonsils were divided into upper pole, middle, and inferior pole planes. The anatomical lines of the tonsils were defined as follows. Surgical subsites. (A): Demarcation of the surgical subsites of the tonsils. 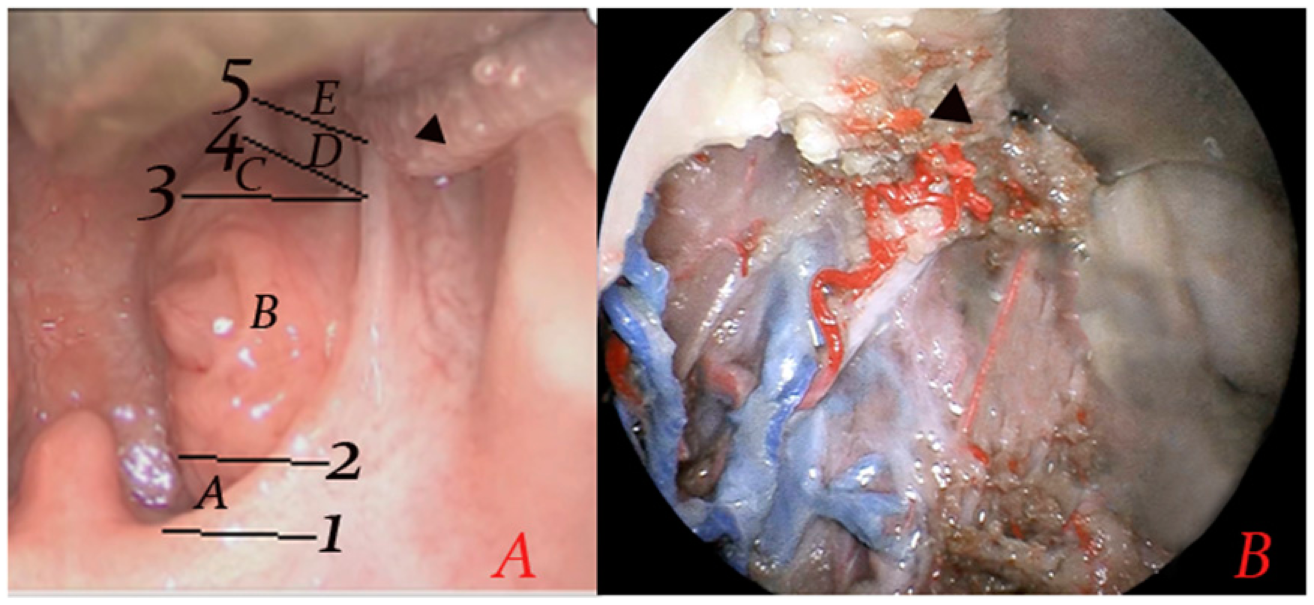
Surgical technique
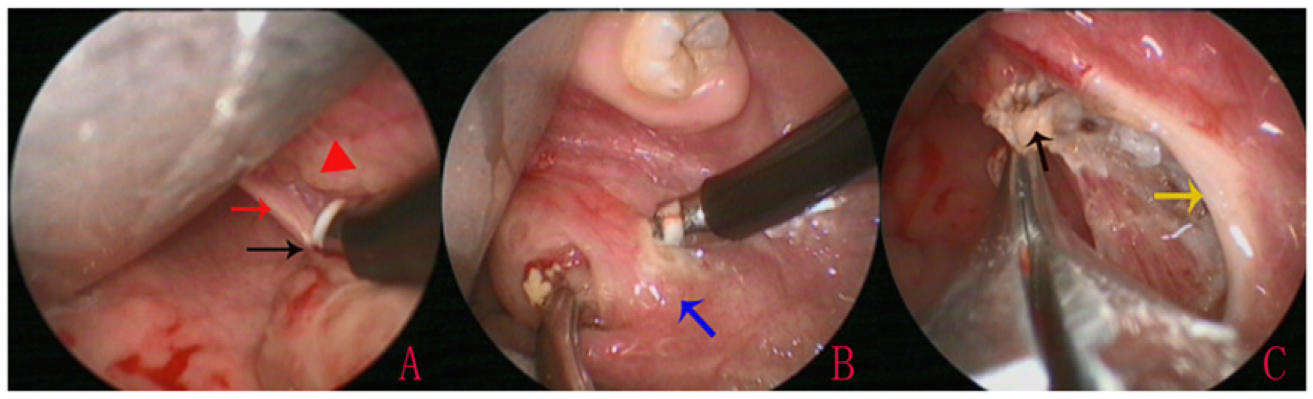
All surgeries were performed under general anesthesia. For all techniques, the peri-tonsillar space was dissected between the tonsillar capsule and the muscle wall. Tonsillectomy using the cold dissection technique was performed using Metzenbaum scissors. After the dissection was closed to the inferior pole and the bleeding arrested using ligatures, tonsil tissue was removed using snare wire. For electrocautery dissection, tonsillar dissection was performed using a monopolar diathermy instrument with suction and a needle tip Bovie (Figure 2); the coagulation was set to 20. For coblation dissection, we used the EVAC-70 handpiece (ENTec) probe with the standard settings of ablation at 7 and coagulation at 3 (Figure 3). For the monopolar and coblation techniques, dense connective tissue between the inferior pole capsule and tongue base were preserved (Figure 2). Patients received a liquid diet postoperatively. The patients were discharged at postoperative day 3 and followed up at postoperative days 7 and 14. Statistical analysis was performed using SPSS Statistics software (version 20.0; IBM Corp., Armonk, NY, USA). Quantitative variables were compared using ANOVA, and qualitative variables were compared using the χ2 test. P-value of < 0.05 was considered statistically significant. Left monopolar tonsillectomy. (A): Identification of inferior pole; (B): post-tonsillectomy. Black arrows indicate the inferior pole. Red triangle: Subsites D and E. Red arrows indicate needle tip Bovie. Coblation tonsillectomy. (A): Identification of the inferior pole; (B): identification of the upper pole; (C): complete dissection. Black arrows indicate the inferior pole. Red triangle: Subsites D and E. Red arrows indicate the posterior pillar; yellow arrows show the anterior pillar; and blue arrows show the top of the upper pole.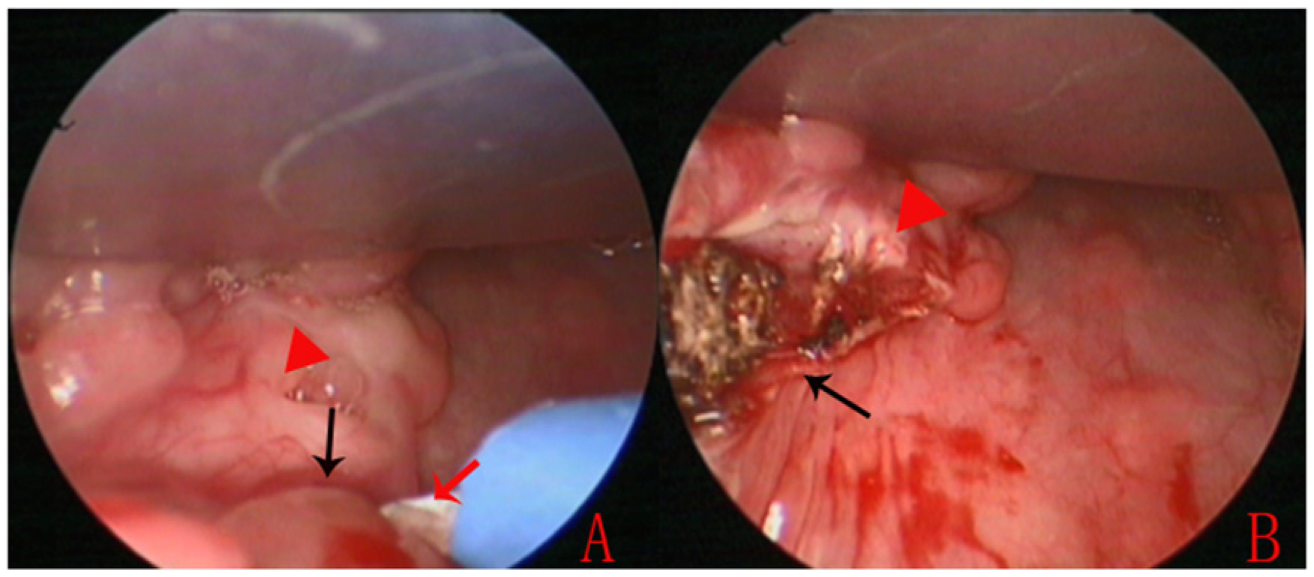
Results
Participant characteristics
This study included 680 patients (225[33.1%], 228 [33.5%], and 227 [33.4%] in the cold dissection, monopolar, and coblation groups, respectively); there were 379 (55.7%) males and 301 (44.3%) females. A total of 71 (10.4%) patients underwent concurrent adenoidectomy. The average age was 17.9 ± 6.8 (range 3–51) years; 426 (62.6%), 161 (23.7%), and 93 (13.7%) were of normal weight, overweight, and obese, respectively.
Coblation tonsillar dissection of adult cadavers
Coblation tonsillar dissection of the adult cadaver showed loose connective tissue at the convergence of the anterior and posterior pillars in the upper pole. The inferior pole capsule was attached to the tongue base with dense connective tissue, with overlying pharyngeal and lingual extension of the lymphoid tissue. The primary feeding artery of the tonsil traversed the anterior pillar on the lower half of the tonsillar fossa to enter the dense connective tissue and establish a deep network of capillaries. A branch of these capillaries traversed the inferior pole capsule to reach the muscle layer of the tonsillar fossa. The diameter of vessels distal to the branching of the primary vessels was smaller than that of the primary vessels. The intra- and extra-capsular vessel topographies were essentially identical. Although the demarcation lines could move up or down by a few millimeters, the arterial vascular network was most dense at subsites D and E, and the vessel diameter at these subsites was significantly greater than those of subsites C and especially E (Fig. 1).
Incidence of PTH
Of the 680 patients who underwent tonsillectomy, 41 (6.0%) developed PTHs, which were early in 13 patients (13/41, 31.7%) and late in 28 (28/41, 68.3%).
The incidences of early bleeding were 3.1% (7/225) in the cold steel group, 1.8% (4/228) in the monopolar group, and 0.9% (2/227) in the coblation group. The incidences of late bleeding were 1.3% (3/225), 3.9% (9/228), and 7.0% (16/227), respectively, being significantly higher in the coblation group than in the cold steel group (P < 0.01).
Observation or compression hemostasis alone was adequate in 12/41 (29.3%) patients exhibiting venous oozing, but surgical intervention was required in 29/41 (70.7%) with pulsatile arterial bleeding. Of PTHs requiring surgical intervention, 4 (4/13, 30.8%) were early (including 3 [3/13, 23.1%] in the cold steel group and 1 [1/13, 7.7%] in the monopolar group) and 25 were late (25/28, 96.4%) (including 1[1/28, 3.6%] in the cold steel group, 9 [9/28, 32.1%] in the monopolar group, and 15 [15/28, 53.6%] in the coblation group).
Associations between PTHs requiring surgical intervention and clinical variables
Comparison of PTH requiring surgical intervention of different variables.
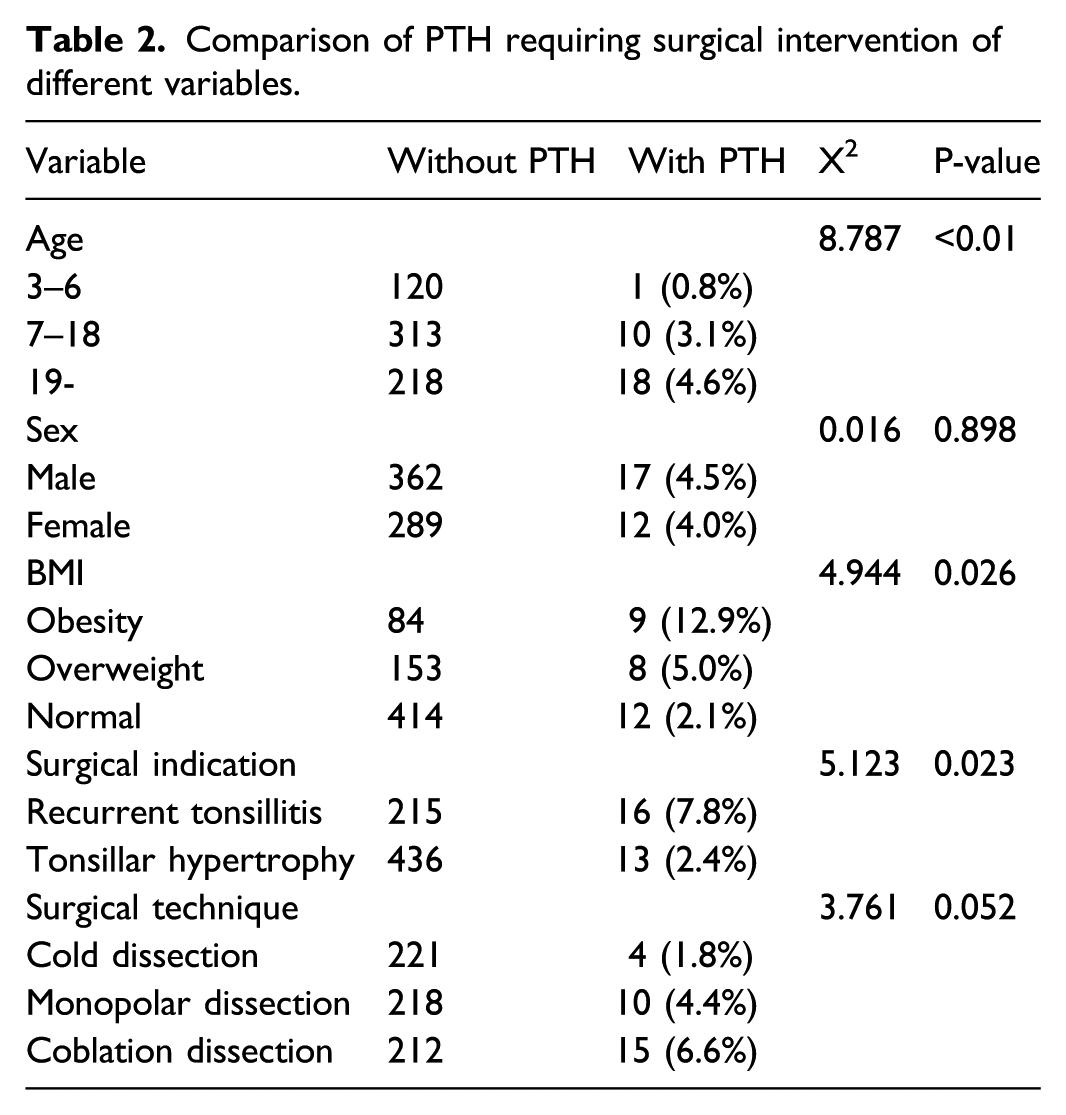
Next, the pediatric cohort (age ≤ 18 years) and adult cohort (age >18 years) were analyzed separately. For the pediatric cohort, no significant correlation was found between PTH and sex (P = 0.656), BMI (P = 0.464), surgical indication (P = 0.883), or surgical technique (P = 0.613). For the adult cohort, no significant correlation was found between PTH and sex (P = 0.854), surgical indication (P = 0.138), or surgical technique (P = 0.230), but the PTH incidence did correlate with the BMI (P = 0.016).
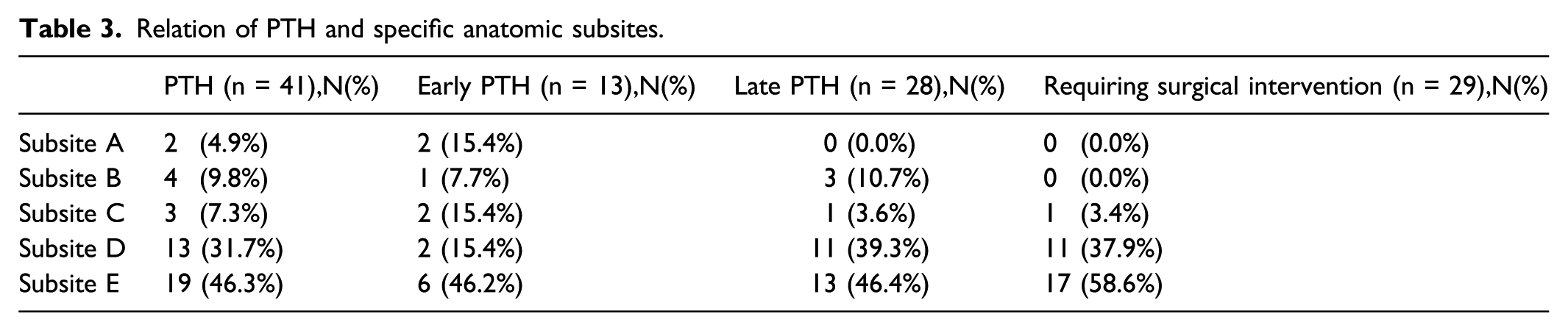
Associations between PTH and specific anatomical subsites
Relation of PTH and specific anatomic subsites.
Discussion
Although the factors that affect PTH risk are well described, limited studies have been performed on the distribution of the vessels located in the surgical dissection plane of tonsillectomy. 15 The arterial blood supply to the tonsils primarily enters at the lower pole. 16 In the present study, the cadaveric specimens showed that the tonsillar feeding artery forms a network of capillaries within the deep dense connective tissue at the lower pole and the lingual extension of the lymphoid tissue. A branch of the capillaries traverses the inferior pole capsule and enters into the muscle layer of the tonsillar fossa.
This study presents a novel classification of the anatomical subsites of the tonsillar fossa based on the distribution of the tonsillar feeding artery. We found that, although the entry points of the tonsillar vessels differed slightly among the three cadaveric specimens, the intra- and extra-capsular vessel topographies were essentially identical. Although precise demarcation of anatomical subsites is difficult and the demarcation lines could move up or down by a few millimeters, the arterial vascular network was dense at subsites D and E, and the vessel diameters at these subsites were significantly greater than at subsite C and especially subsite E, as previously reported. 16 Thus, subsites D and E are the “danger zones” of extracapsular tonsillectomy, and subsite C is a relatively safe zone. These findings suggest that tonsillectomy is safest when performed close to the upper pole and dangerous when performed close to the lower pole.
Demarcation of the anatomical subsites indirectly reflected the topography of the arterial vessels. Thus, the numbers and densities of vessels at the various subsites should be considered during tonsillectomy. The most common sites of PTH were anatomically delineated. All late bleeding and all PTHs requiring surgical intervention involved pulsatile arterial bleeding in subsites D and E (except for one bleeding in subsite C). In contrast, surgical intervention was rarely required for PTHs at subsite A or B. In earlier studies, the inferior pole was the most common site of clinical PTH.8,9,12,13
We found no significant association between PTH and sex. However, a higher BMI was associated with increased PTH risk, in line with previous studies.17,18 Obesity is usually accompanied by maxillofacial deformities and pachyglossia, which result in poor oropharynx exposure and thus the surgical instruments may damage the dangerous subsites. The PTH risk was significantly higher among patients with recurrent tonsillitis compared to tonsillar hypertrophy, which is in line with previous studies.19-21 Recurrent tonsillitis not only created hyperplastic scars at subsites D and E and synechia of the tonsillar capsule and tongue base but also increased the diameters of capillaries in fibrotic tissue. 16 Thus, PTH was easily induced during tonsillectomy. However, the secondary analysis showed that only obesity predicted bleeding in the adult cohort. This explains why the incidence of PTH in adults was significantly higher than in children.
We did not find any significant correlations between early bleeding and surgical technique, although the incidence of late bleeding in the coblation group was significantly higher than in the cold steel group. Some studies have reported that PTH is related to the size of the diathermy tip. 22 The tip of the coblation wand was larger than the needle tip Bovie of monopolar electrocautery, which increased the injury to the surrounding tissue and produced more extensive damage. The needle tip Bovie of monopolar electrocautery may improve the precision of cautery. In addition, PTH is related to instrument characteristics.10,23 During coblation, lower temperatures (i.e., 40–60°C) result in minimal mechanical and thermal damage to adjacent tissues, while coagulum and clots start forming at temperatures > 60°C. 24 The extents of epithelial destruction and collagen denaturation in surrounding tissue are less after coblation than electrocautery, leading to reduced inflammation and granulation tissue formation. These factors may attenuate the tissue inflammatory response and coagulum formation. 23 Thus, closure with the ablation method may be adequate for small blood vessels, but for medium and large vessels, closure with the ablation method is unreliable. As reported previously,11,16 endoscopy revealed that the vessel diameters of the subsites D and E were significantly greater than that of subsite C. Intracapsular tonsillectomy has been recommended by some scholars; this may minimize the exposure of larger blood vessels.11,16 Other scholars have suggested suturing of the inferior pole to reduce the PTH incidence after coblation extracapsular tonsillectomy.8,9
The topographical relationship between the palatine tonsil and vessels provides an anatomical rationale for a change in the surgical technique to minimize vascular injury and improve the safety of tonsillectomies. The novel classification of the anatomical subsites of the tonsillar fossa presented here would aid inexperienced surgeons and emphasize the need to avoid damage to the tonsillar capsule when approaching dangerous subsites, especially the lateral zone of the inferior pole. Our results suggest that tonsillectomy with preservation of the inferior pole should be considered to avoid injury to the extracapsular capillary networks of pediatric cases. However, for adults with OSA or inflammatory disease, prophylactic cautery should be considered for both the relatively safe and dangerous subsites if an inferior pole injury is suspected. The limitations of the study are the few cadaveric specimens, the lack of specimen sectioning, and the lack of data on vessel calibers.
Conclusion
Classification of the anatomical subsites of the tonsillar fossa aids inexperienced surgeons and affords an anatomical rationale for variation in the surgical technique to minimize vascular injury and thus improve safety.
Footnotes
Author’s Contributions
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Technology Agency of Yiwu city, China (Grants#2021-3-55).