
Abstract
Pertussis, caused by Bordetella pertussis, is increasingly recognized in adults who often present with atypical symptoms, leading to underdiagnosis. We report a case of a 64-year-old woman with a persistent cough and sore throat initially treated as refractory community-acquired pneumonia. Despite empirical antibiotic therapy, her symptoms persisted. Conventional diagnostic tests, including sputum and bronchoalveolar lavage fluid cultures, were negative. Metagenomic next-generation sequencing of bronchoalveolar lavage fluid identified Bordetella pertussis with high sequence coverage (7497 reads). The patient showed no clinical improvement with azithromycin, prompting a switch to trimethoprim–sulfamethoxazole, after which she improved and was discharged to complete a 14-day course. At 1-month follow-up, she was asymptomatic with resolved radiographic findings. This case highlights that pertussis can mimic refractory pneumonia in adults without typical features such as whooping cough, and underscores the diagnostic value of metagenomic next-generation sequencing when conventional methods fail. Clinicians should consider pertussis in adults with prolonged cough unresponsive to standard community-acquired pneumonia therapy and be aware of potential macrolide resistance, which may necessitate alternative antibiotics like trimethoprim–sulfamethoxazole.
Keywords
Introduction
Pertussis, an acute respiratory infectious disease caused by Bordetella pertussis, has seen a decline in prevalence due to widespread vaccination. However, a concerning resurgence has been observed globally in recent years. 1 Waning immunity from childhood diphtheria–tetanus–pertussis vaccination is a significant factor in this re-emergence. While often considered a childhood disease, pertussis can affect adults, where presentations are frequently atypical, lacking the characteristic whooping cough. 2 This atypicality, coupled with a low index of suspicion and the lack of sensitive routine diagnostic tests, often leads to misdiagnosis or delayed diagnosis. 3 Adults with underlying respiratory conditions like asthma or chronic obstructive pulmonary disease (COPD) are at increased risk for pertussis and its complications, including exacerbations. 4 Consequently, health authorities like the Centers for Disease Control and Prevention recommend Tdap vaccination for adults, including those with COPD. 5
Diagnosing pertussis in adults presenting with prolonged cough remains challenging. This case report details the diagnosis and management of an adult patient with B. pertussis pneumonia, initially misdiagnosed as common community-acquired pneumonia (CAP), and discusses the differential diagnosis from COPD and asthma. We aim to enhance clinician awareness of pertussis in adults and highlight the role of advanced diagnostic techniques, such as metagenomic next-generation sequencing (mNGS), in similar scenarios.
Case presentation
History and initial presentation
We describe a hospitalized 64-year-old woman in the department of respiratory and critical care medicine. Approximately 2 weeks before hospitalization, the patient began to have a cough without an obvious cause, which was a dry cough at first, with little sputum, obvious at night, and accompanied by a sore throat. She was treated at the local health center and clinic with oral drugs, but her symptoms were not relieved. Three days before hospitalization, she went to our outpatient clinic. Relevant tests were done. Blood routine examination showed white blood cell 12.3 × 109/L↑; neutrophil ratio 77.80%↑; red blood cells 4.39 × 1012/L; hemoglobin was 134 g/L; platelet 277 × 109/L; IgM antibody to Mycoplasma pneumoniae was negative. Chest X-ray showed no obvious abnormality. Budesonide atomization was given, and doxofylline tablets, montelukast sodium tablets, loratadine tablets, roxithromycin ambroxol tablets, cefprozil tablets, and compound pholcodine oral solution were taken orally according to the drug instructions. However, the symptoms did not improve, and the cough was still severe, with intermittent dark brown purulent sputum, which was frequent and could not be completely tolerated. She was hospitalized for further diagnosis and treatment.
Hospital course, diagnostic workup, and treatment
On admission, the temperature was 36.5 °C, P 93 beats/min, R 23 beats/min, BP 116/63 mmHg, SPO2 96%, pharyngeal congestion, auscultation of both lungs coarse breath sounds, both lower lungs can be heard with a little wet rales, heart rate 93 beats/min, rhythm. Admission arterial blood gas analysis: pH 7.49, PCO2 35 mmHg, PO2 85 mmHg, HCO3− 27.7 mmol/L, BE 3.5 mmol/L, SO2 97%, K⁺ 3.3 mmol/L, Ca²⁺ 1.11 mmol/L, Lac 1.0 mmol/L, FIO2 was 21%.
The initial diagnosis was CAP. Given the failure of previous antibiotic therapy (cefprozil, a cephalosporin) and the absence of an identified pathogen, empirical broad-spectrum antibacterial coverage with a β-lactam/β-lactamase inhibitor was initiated. Piperacillin-tazobactam (4.5 g intravenously every 8 h) was administered starting on admission day alongside budesonide inhalation. This regimen was continued for 7 days until mNGS results became available.
Further investigations showed an elevated erythrocyte sedimentation rate (88 mm/h) and C-reactive protein (CRP; 28.9 mg/L). The complete blood count showed persistent leukocytosis (11.2 × 109/L) and neutrophilia (8.65 × 109/L); occasional toxic granules were noted in neutrophils. Coagulation profile, renal function, liver function, and myocardial enzymes were normal. Sputum culture and smear showed no significant pathogens. Chest computed tomography (CT) revealed minor inflammatory changes in the left lower lobe and a linear shadow in the right middle lobe (Figure 1).
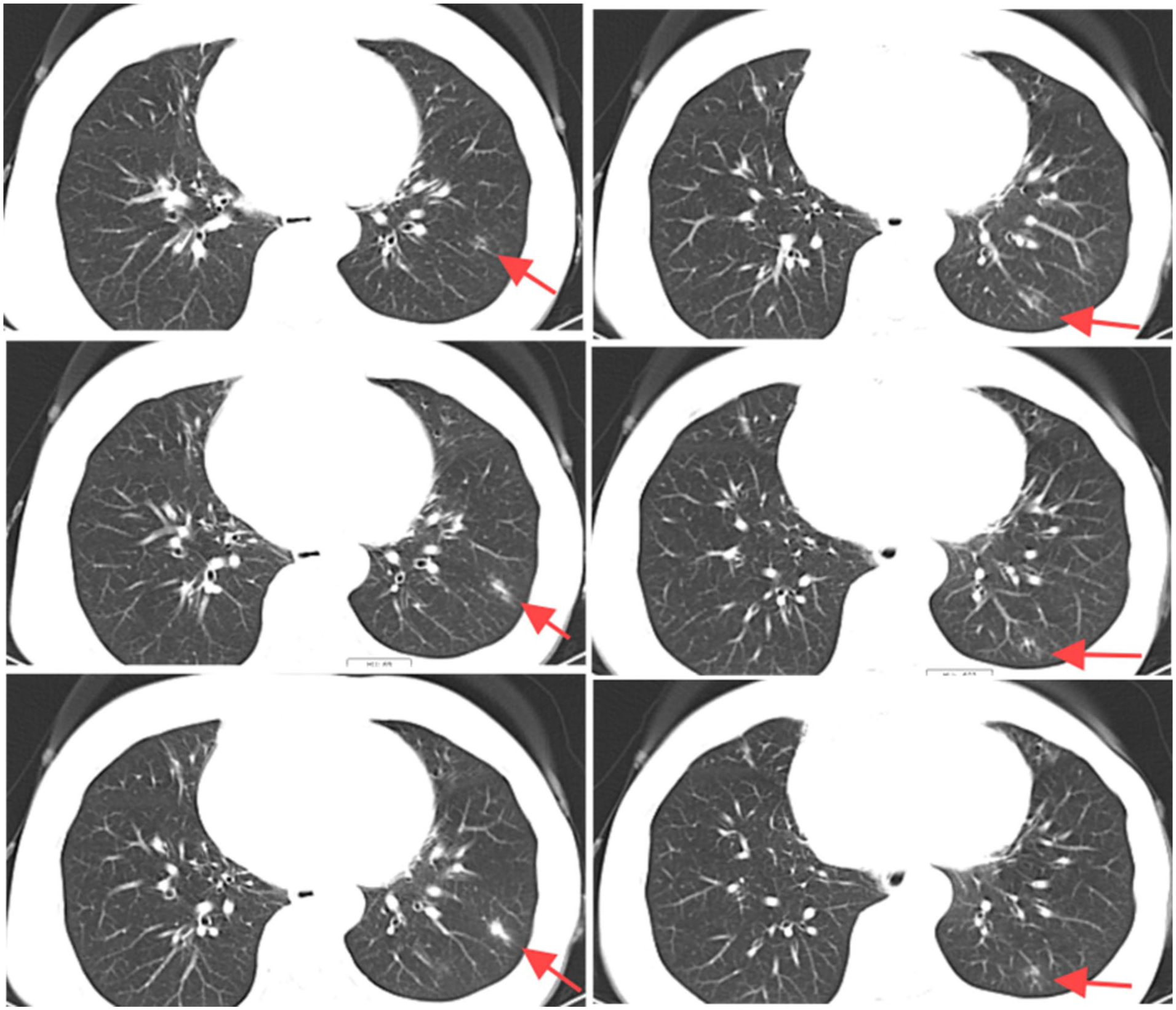
Partial sections of chest CT before treatment. Lesions are indicated by red arrows.
On hospital day 3, the patient continued to report pharyngeal dryness, itching, and pain. Laryngoscopy showed a dark red nodule at the left tongue base, congested throat mucosa, and prominent congestion in the arytenoid area. Given the persistent cough, COPD and asthma were considered. However, pulmonary function tests on day 4 showed normal ventilation function, slightly increased lung residual volume, mildly decreased diffusion capacity, and a flow-volume curve with slightly decreased values except for maximal expiratory flow at 25%. A bronchodilation test was negative. Concurrent blood tests showed resolving leukocytosis (WBC 6.4 × 109/L, neutrophils 4.06 × 109/L) and normalized CRP (<10 mg/L). Bronchoscopy on day 6 revealed swelling and redness of the bronchial mucosa throughout both lungs; otherwise, the airways appeared normal. Bronchoalveolar lavage (BAL) was performed in the left lower lobe’s lateral basal segment. The BAL fluid was sent for standard bacterial and fungal culture, acid-fast bacillus smear and culture, and cytological examination; these routine tests were unremarkable.
Due to the persistence of symptoms despite broad-spectrum antibiotic therapy and the lack of a definitive pathogen identified through conventional methods, metagenomic mNGS was performed on the BAL fluid sample to identify potential atypical or fastidious pathogens. On day 7, mNGS detected B. pertussis sequences with high read coverage (7497 reads), supporting a confident diagnosis.
The diagnosis was subsequently revised to B. pertussis pneumonia. Based on guidelines recommending macrolides as first-line therapy, the antibiotic was adjusted to azithromycin (500 mg intravenously once daily). On day 9, the patient reported nasal pain. A sinus CT revealed a deviated nasal septum and bilateral inferior turbinate hypertrophy, but no evidence of abscess or sinusitis. By day 11, the patient reported no significant improvement in her respiratory symptoms with azithromycin. A repeat chest CT showed a slight increase in the inflammatory infiltrates in the left lower lobe (Figure 2). Considering the reported high rates of macrolide resistance in B. pertussis 6 and the lack of clinical response, antibiotic therapy was switched to oral trimethoprim–sulfamethoxazole (TMP–SMX; 800/160 mg, two tablets every 12 h). Blood tests on day 12 showed normalized white cell count (6.3 × 109/L), neutrophil count (3.8 × 109/L), and CRP (<10 mg/L). On day 15, the patient still experienced throat discomfort. Laryngoscopy findings had improved but showed mild mucosal congestion and atrophy, consistent with chronic pharyngitis. This was managed symptomatically with oral Chinese patent medicine (e.g. soothing lozenges) and saline gargles. As her respiratory infection was deemed under control with oral antibiotics, she was discharged on hospital day 15 with instructions to complete a 14-day course of TMP–SMX.

Partial sections of chest CT after treatment. Lesions are indicated by red arrows.
Follow-up
One month after discharge, the patient was followed up in the outpatient clinic. She reported complete resolution of all respiratory symptoms, and physical examination was unremarkable. A repeat chest CT showed complete resolution of the previous lung infiltrates (Figure 3), and infection markers remained normal. The timeline of diagnostic and therapeutic interventions is shown in Figure 4.
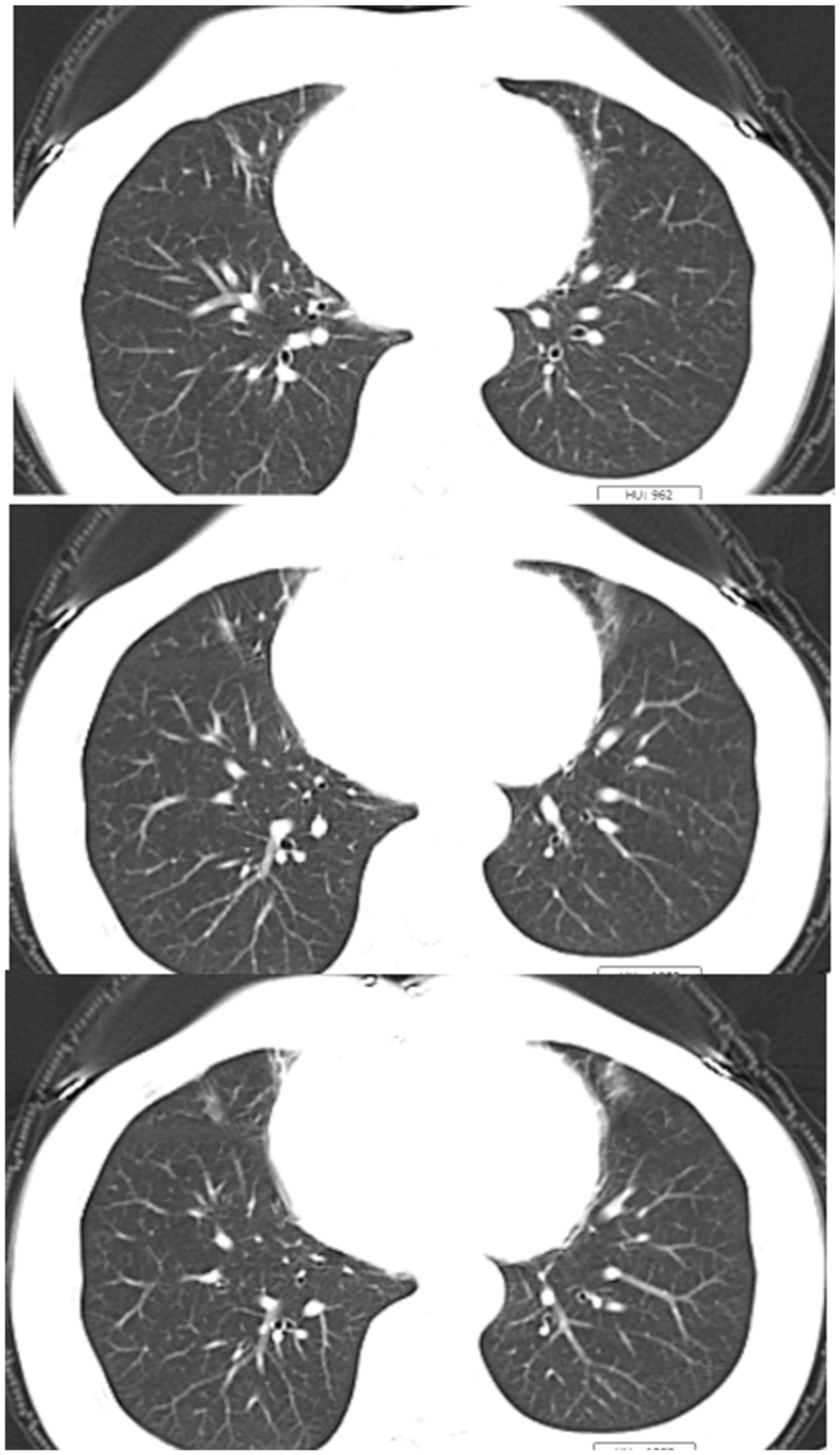
Follow-up chest CT after discharge. The lesion in the original section was completely absorbed.

Timeline of diagnostic and therapeutic interventions.
Discussion
This case illustrates the diagnostic challenge posed by pertussis in adults. The patient’s main symptoms were cough and sore throat, accompanied by elevated inflammatory markers and pulmonary infiltrates on CT, initially suggesting a common upper respiratory infection with concomitant pneumonia. The lack of response to first-line empirical CAP treatment, including a cephalosporin and later a macrolide (roxithromycin outpatient, azithromycin inpatient), was a crucial clue that an atypical pathogen might be involved.
The differential diagnosis for persistent cough in an elderly adult includes conditions such as COPD and cough-variant asthma.7,8 However, the normal pulmonary ventilation function and negative bronchodilator test effectively ruled out obstructive lung diseases as the primary cause. The complaint of nasal pain prompted consideration of sinonasal pathologies such as abscess or tumor, causing post-nasal drip, but CT imaging excluded these. The definitive diagnosis was ultimately achieved through mNGS testing of BAL fluid, which identified B. pertussis. This highlights the utility of mNGS in diagnosing difficult cases of refractory respiratory infection where conventional methods fail, especially for fastidious or atypical pathogens.9,10 Its broad, unbiased detection capability makes it particularly valuable in this context.
Notably, even after identifying the pathogen, treatment challenges persisted due to suspected macrolide resistance. The patient’s failure to improve on azithromycin, followed by clinical stability after switching to TMP–SMX, supports this suspicion and aligns with reports of increasing macrolide-resistant B. pertussis strains.6,11 This underscores the importance of considering resistance patterns and having alternative treatment options available.
Several aspects of this case are noteworthy for understanding adult pertussis. The patient reported a sore throat throughout her illness. The mechanisms for this in pertussis may include direct mechanical trauma to the pharyngeal mucosa from violent paroxysmal coughing, inflammation caused by the bacterium’s toxins, or secondary infections due to compromised local immunity. 12
Secondly, while cough is a feature of pertussis, COPD, and asthma, their patterns differ. Pertussis typically progresses through catarrhal, paroxysmal, and convalescent stages, with the paroxysmal stage characterized by staccato coughing fits, often followed by an inspiratory whoop and post-tussive vomiting, lasting 2–6 weeks. 13 COPD cough is often chronic, productive, and worse in the mornings, while asthma-related cough is typically episodic, associated with triggers, and may include wheezing. 14 Careful history-taking is essential to distinguish between them. Pertussis should be considered a common cause of persistent cough in adults. 3
Additionally, the patient’s nasal pain, though initially misleading, is a recognized symptom in adult pertussis, with studies reporting incidences as high as 80% for sinus pain or discomfort. 15 This is likely related to the catarrhal symptoms and inflammation extending to the sinonasal passages (Supplemental Material).
Finally, this case reinforces that pertussis is highly contagious via respiratory droplets. Adults, often unaware of their infection, can be important reservoirs and transmit the bacteria to vulnerable infants, for whom the disease can be severe or fatal.16,17 Public health measures, including vaccination of adults and caregivers (cocooning strategy) and hygiene practices such as covering coughs, are crucial for prevention.
Conclusions
This case highlights that adult pertussis can present as refractory pneumonia without typical features like whooping cough. mNGS played a critical role in identifying B. pertussis after conventional diagnostic methods failed. Furthermore, the lack of response to first-line macrolide therapy, suspected to be due to resistance, underscores the need for awareness of alternative treatments. Clinicians should consider pertussis in the differential diagnosis of adults with persistent cough, particularly those not responding to standard CAP therapy, and be mindful of its public health implications.
Supplemental Material
sj-docx-1-sco-10.1177_2050313X251411124 – Supplemental material for Pertussis is identified among common respiratory diseases: A case report
Supplemental material, sj-docx-1-sco-10.1177_2050313X251411124 for Pertussis is identified among common respiratory diseases: A case report by Jiajia Chen, Yongchang Wu, Jiamei Tang, Jiguang Guo and Yu Zhai in SAGE Open Medical Case Reports
Footnotes
Acknowledgements
The above authors would like to express their gratitude to Yu Zhai for his outstanding guidance and leadership in this case.
Ethical considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent to participate
Written and signed documentation of this consent is within the patient’s hospital records. Copies of the consent forms are available upon request.
Consent for publication
Written informed consent was obtained from the patient for their anonymized information and images to be published in this article.
Author contributions
Jiajia Chen was responsible for writing the entire manuscript. Jiamei Tang and Yongchang Wu were responsible for consultation and editing. Jiguang Guo was responsible for the revisions of the article after its review and the polishing of its English language expression.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting the findings of this case report are included within the article. The original mNGS data and clinical details are available from the corresponding author upon reasonable request. No publicly available datasets were generated or analyzed in this study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.