
Abstract
Background:
Adenotonsillectomy is a common pediatric procedure, but pharyngeal stenosis remains one of its most severe complications. This condition, characterized by cicatricial narrowing of the airway, leads to significant morbidity. Given its rarity and the absence of a standard management protocol, a comprehensive synthesis of the evidence is crucial.
Methods:
A systematic review was conducted following PRISMA 2020 guidelines. A comprehensive search of PubMed, Web of Science, and Scopus from inception through December 2025 identified studies reporting pharyngeal stenosis following adenotonsillectomy, tonsillectomy, or adenoidectomy. Data on epidemiology, etiology, clinical features, management, and outcomes were extracted and analyzed.
Results:
The review analyzed 39 studies encompassing 166 cases. The mean age was 14.87 years, with a near-equal sex distribution. The nasopharyngeal was the most common site of stenosis (122 cases). The most frequent symptoms were nasal obstruction and snoring. Thermal techniques, particularly electrocautery, were the most commonly associated surgical method. Over 40 distinct surgical techniques were identified for management. While significant symptomatic improvement was achieved in 85.2% of cases, the overall recurrence rate was high at 25.4%. Analysis of recurrent cases revealed no single superior technique, underscoring the condition’s refractory nature. The adjunctive use of anti-fibrotic agents like mitomycin C and steroids was a common feature in modern management strategies.
Conclusion:
Pharyngeal stenosis, though rare, is a devastating complication strongly associated with thermal surgical techniques and characterized by a high recurrence rate. Prevention through meticulous surgical technique is paramount. Successful management requires a personalized, multimodal approach combining surgical release, resurfacing with vascularized flaps, anti-fibrotic agents, and, in select cases, prolonged stenting. Long-term follow-up is essential to monitor for recurrence and manage sequelae effectively.
Keywords
Introduction
Adenotonsillectomy remains one of the most frequently performed surgical procedures in pediatric otolaryngology, primarily indicated for obstructive sleep apnea and recurrent infections. 1 While generally considered safe and effective, it is not without potential complications, among which pharyngeal stenosis represents one of the most challenging and debilitating sequelae. 2 This condition, characterized by cicatricial narrowing of the velopharyngeal, oropharyngeal, or nasopharyngeal airway, can lead to severe upper aerodigestive tract obstruction, dysphagia, and sleep-disordered breathing. 3
Although rare, with an incidence that remains poorly quantified, pharyngeal stenosis continues to be documented as an unusual yet serious complication following adenotonsillectomy. 4 The pathophysiology typically involves excessive fibrosis and adhesion formation between raw mucosal surfaces, often exacerbated by electrocautery use, deep dissection, or repeated surgical trauma.2,5 Since the first documented repair of nasopharyngeal stenosis by Nichols in 1896, numerous surgical techniques have been described, including local flaps, Z-plasty, skin grafting, and adjuvant therapies such as mitomycin C or steroid injections.4,5 Despite these advances, recurrence remains common, and no universally accepted management protocol exists.5,6
Notably, while most reported cases occur in children, adult presentations are increasingly recognized, further broadening the clinical spectrum of this iatrogenic condition. 6 The variability in anatomical involvement—ranging from isolated velopharyngeal stenosis to complex oronasopharyngeal strictures—adds to the diagnostic and therapeutic challenge.3,4 Unusual and severe complications continue to be documented in the modern surgical era, underscoring the need for heightened awareness and meticulous surgical technique.7 -11
In this article, we present a case of severe pharyngeal stenosis in a child following adenotonsillectomy, successfully managed with pharyngoplasty and prolonged stenting. Furthermore, we provide a systematic review of all documented cases in the medical literature from 1896 to 2025, offering a consolidated analysis of etiological factors, clinical features, and evolving treatment strategies. This dual aim of case illustration and systematic review seeks to contribute to the limited body of evidence on this rare but consequential complication.
Case Presentation
An 8-year-old girl presented with bilateral nasal obstruction and stertor several months after an adenotonsillectomy performed 3 years prior. On examination, there was an obstruction of the oropharyngeal with complete closure of the naso-oral isthmus, and the uvula was distracted and disappeared (Figure 1). A lateral radiograph showed complete nasopharyngeal obstruction, suggesting adhesions between the soft palate and the posterior pharyngeal wall (Figure 2). The patient underwent pharyngoplasty without stenting several months after the initial operation, which relieved the symptoms. However, nasal obstruction recurred with severe stricture and pharyngeal fibrosis, and she was scheduled for a second pharyngo-palatoplasty for this recurrent severe nasopharyngeal obstruction, fibrosis, and nasal breathing obstruction. The patient experienced moderate to severe dysphagia with weight loss and buccal obligate breathing, but there was no hoarseness, sialorrhea, hemoptysis, or ear-related symptoms. The surgical intervention involved exposing the oral cavity, releasing adhesions between the soft palate and posterior pharyngeal wall, as well as between the lingual base and posterior pharyngeal wall. Bilateral incisions were made to relax the soft palate. Inferiorly based flaps of the posterior pharyngeal wall and the lateral pharyngeal walls were created and sutured to the soft palate. Stenting was achieved with a silastic sheet rolled into a cylindrical mold, placed and secured with Prolene 3/0 stitches to the soft palate and the posterior and lateral pharyngeal walls. A nasogastric tube was inserted. The postoperative course was uneventful, and stenting was maintained for 3 months to prevent recurrence. After stent removal, the patient gradually improved with good nasal respiration and swallowing.

Oropharyngeal stenosis with absence of the uvula.

Complete nasopharyngeal airway obstruction with adhesions between the uvula and the posterior pharyngeal wall.
Methods
This systematic review was conducted in accordance with the updated Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement. A comprehensive search strategy was designed and executed to identify all relevant published literature. Electronic databases—including PubMed, Web of Science, and Scopus—were searched from their inception through December 2025.
The search utilized a combination of Medical Subject Headings (MeSH) terms and keywords related to anatomical structures (oropharyngeal, nasopharyngeal, oropharynx, nasopharynx, pharyngeal, pharynx, velopharyngeal) and the condition of interest (stenosis, stricture) in the context of the primary surgical intervention (tonsillectomy, adenotonsillectomy, adenoidectomy). These terms were strategically combined using Boolean operators (AND/OR). The search was restricted to publications in the English language; however, no restrictions were placed on the article type or date of publication to ensure a broad capture of potentially relevant studies. Some papers were found by examining the reference lists of other papers.
The Initial database search yielded 325 records. Following the removal of duplicates, the screening process commenced. Two independent reviewers first assessed the titles and abstracts of all identified records for relevance. This initial screening resulted in 39 articles being deemed eligible for full-text evaluation. These full-text articles were then rigorously assessed against pre-defined eligibility criteria.
Studies were excluded if they were not published in English, were not original research (eg, reviews, editorials), or if they discussed pharyngeal strictures attributable to etiologies other than adenotonsillectomy or related procedures. Any discrepancies between the 2 reviewers during the full-text assessment phase were resolved through discussion until a consensus was reached. When consensus could not be achieved, a third reviewer was consulted for arbitration. This process culminated in the inclusion of 39 studies for final analysis,1 -6,12 -44 the selection of which is detailed in the PRISMA flow diagram (Figure 3).
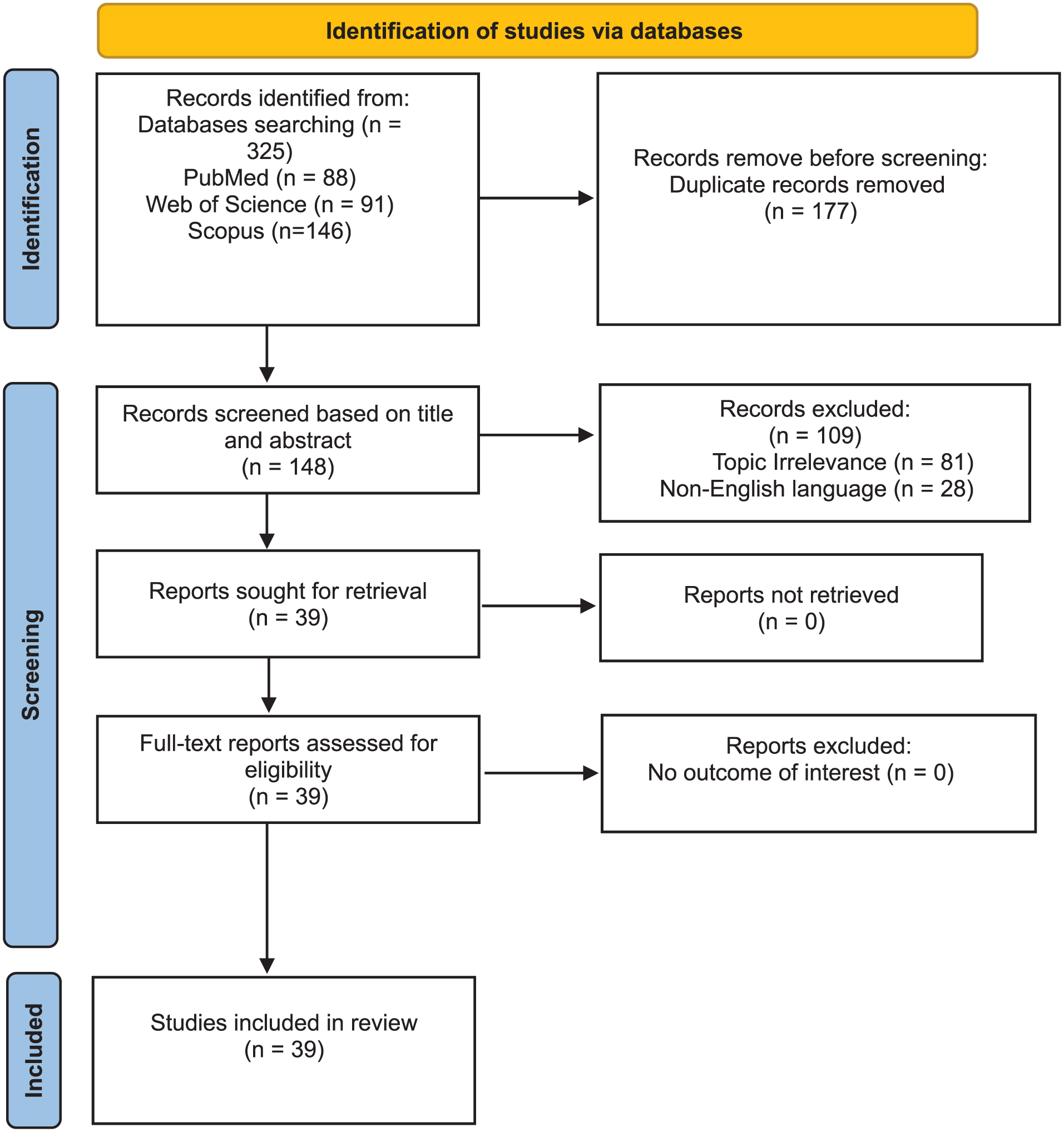
PRISMA flowchart for selection of the articles in the systematic review.
Data from the included studies were extracted independently by 2 reviewers using a standardized, piloted data extraction form developed in Microsoft Word. The form was designed to capture detailed information across several domains: epidemiology, etiology, clinical manifestations, diagnostic, management strategies, and treatment outcomes. The extracted data were subsequently cross-verified between the 2 reviewers to ensure accuracy and consistency, with any discrepancies being resolved by referring back to the original source article. Study quality was assessed using JBI critical appraisal tools for case reports/series.
Results
Study and Case Characteristics
Our systematic review identified 39 papers reporting documented cases of pharyngeal stenosis as a complication of tonsillectomy. These included 19 case series and 20 case reports, encompassing a total of 165 cases. With the addition of the case presented in this paper, the overall number of documented pharyngeal stenosis cases in the medical literature reaches 166 (Table 1; Figure 3). Age was reported in 80 cases, with a range of 2 years to 62.1 years and a mean age of 14.87 years. Patient sex was reported in 79 cases, comprising 42 females and 37 males. Table 1 shows a summary of all cases.
Summary of all Pharyngeal Stenosis cases documented in literature.

Abbreviations: NA, N/A: not available. F: female. M: male. Both: nasopharyngeal and oropharyngeal. COME: chronic otitis media with effusion.
Treatment Modalities and Outcomes
Regarding the anatomical site of the stenosis, the distribution was as follows: 122 cases were located in the nasopharyngeal, 7 in the oropharyngeal, and 37 cases involved both regions (nasopharyngeal and oropharyngeal).
Concerning the primary surgical procedure that led to the complication, the vast majority of cases (147) occurred following adenotonsillectomy. The remainder were attributed to tonsillectomy alone (5 cases), adenoidectomy alone (9 cases), while the specific procedure was not definitively identified in 5 cases.
The reported symptoms of nasopharyngeal and oropharyngeal stenosis include difficulty breathing (nasal obstruction, mouth breathing, dyspnea, exertional breathlessness, respiratory distress, suffocation, and obstructive sleep apnea), snoring, speech abnormalities (hypernasality, hyponasality, impaired speech), dysphagia (difficulty swallowing, odynophagia, food trapping), nasal symptoms (rhinorrhea, inability to blow the nose, anosmia, nasal congestion, chronic rhinosinusitis), gagging, pharyngeal reflux, pharyngeal fullness, weight loss, fatigue, headaches, daytime somnolence, decreased physical endurance, and chronic otitis media with effusion (COME). The most common symptom Is nasal obstruction. The second most common symptom is snoring.
The latency period between adenotonsillectomy and the onset of pharyngeal stenosis symptoms was reported in 39 cases. The duration ranged from immediately postoperatively to 1825 days (5 years), with a mean of 221.3 days. Two significant outliers—one with a latency period of 11 years and another of 30 years—were excluded from this calculation.
Data on the surgical technique employed for the adenotonsillectomy were available for 48 cases. The distribution was as follows: electrocautery was used in 29 cases, KTP laser in 8, cold instrument dissection in 2, LigaSure in 1, Coblation in 5, coblation radiofrequency in 2, and intracapsular tonsillectomy in 1 case.
Regarding treatment techniques, 137 cases were reported as follows: 3 cases of Mackenty flap, 4 of lysis of scar bands, 7 of mucosal flaps, 2 of lysis with silver obturator, 4 of lysis with skin graft on stent, 2 of Mackenty flap lysis and dental obturator, 1 of lysis and tantalum obturator, 1 of mucosal flap with tantalum obturator, 1 of lysis with polyethylene obturator, 1 of lysis and stent, 2 of skin graft on stent, 3 of lysis and obturator, 1 of lysis and edge closure, 1 of lysis and Kazanjian two-stage, 1 of lysis and packing, 7 of bilateral "Z" plasties, 2 of Kazanjian first stage, 2 of Kazanjian two-stage, 6 of modified Z-plasty, 6 of unilateral palatoplasty, 1 of insertion of plastic tubes through the atresia, 5 of laterally based pharyngeal flap, 2 of laterally based pharyngeal flap with stent, 1 of laterally based pharyngeal flap and V-Y pharyngeal advancement flap, 1 of laterally based pharyngeal flap with Nylon suture to create opening, 1 of lateral-based posterior pharyngeal wall flap with triamcinolone acetonide injection (multiple sessions), 2 of triamcinolone acetonide injection (multiple sessions), 1 of triamcinolone acetonide injection with Z-plasty, 1 of triamcinolone acetonide injection (multiple sessions) with bilateral horizontal-to-vertical plasty, 1 of dilation, 3 of endoscopic intranasal repair with stenting and minor revision, 1 of endoscopic intranasal repair with stenting and Nd:YAG laser, 2 of transpalatal with endoscopic intranasal repair and stenting, 1 of dilation with steroid injection, 1 of pharyngoplasty with posterior pharyngeal wall advancement flap, 12 of two-stage palatal eversion with midline division, scar removal, lateral fixation for 6 weeks, then reunion, 1 of scar excision with AlloDerm graft, Z-plasty flaps, intra-op tissue expander dilation, triamcinolone injection, and Mitomycin C application, 1 of lysis of scar bands with bilateral buccal mucosal graft, 1 of surgical scar division and palatal scar lengthening with local advancement flap reconstruction, 10 of modified single-stage palatal eversion with midline soft palate split, sharp dissection of pillars, scar excision, and lateral fixation with absorbable sutures, 3 of scar resection and horizontal-to-vertical pharyngoplasty, local pharyngeal flap rotation, free skin graft, and prolonged nasopharyngeal stent (>6 months), 2 of scar resection and horizontal-to-vertical pharyngoplasty, local pharyngeal flap rotation, and prolonged nasopharyngeal stent (>6 months), 1 of surgical excision with 3mm margins, triamcinolone infiltration, primary layered closure, and palatopharyngoplasty, 14 of bivalved uvular flap with Mitomycin C application, 1 of stricture release (scalpel and cobaltion), application of Feracrylum gel 3%, and placement of an indwelling infant feeding tube as a stent, 1 of surgical excision (plasma device) with triamcinolone injections, 1 of Madame Butterfly free everted palatal flap technique, scar tissue excision, placement of uncuffed endotracheal tubes and a Silastic sheet for 2 weeks post-op, 1 of extracapsular tonsillectomy, dissection of stenosis, and anterolateral repositioning suturing of the palatopharyngeal arches, 1 of dissection of fibrous adhesions and anatomical layered reconstruction of the soft palate, and 1 of adhesiolysis, bilateral soft palate relaxing incisions, inferiorly based pharyngeal flaps, and placement of a silastic stent for 3 months.
Regarding postoperative outcomes, data were reported for 122 cases. Among these, significant symptomatic improvement was noted in 104 cases, partial improvement in 10 cases, and no improvement was reported in 8 cases.
Concerning recurrence, this parameter was documented for 126 cases. Of these, 32 cases reported a recurrence of stenosis, yielding a recurrence rate of 25.4%.
Follow-up duration was reported for 88 cases. The period ranged from 0.25 to 108 months, with a mean follow-up time of 15.5 months.
Analysis of Recurrent Cases
Patients with documented recurrence (n = 32):
Primary surgical procedure: The initial procedures leading to stenosis in these recurrent cases were distributed as follows: adenotonsillectomy (22 cases), revision adenotonsillectomy (6 cases), tonsillectomy (1 case), and adenoidectomy (3 cases).
Site of stenosis: The stenosis was located in the nasopharyngeal in 29 cases, while 3 cases involved both the nasopharyngeal and oropharyngeal.
Management techniques: The therapeutic interventions employed for these recurrent cases were highly varied and included the following procedures: Lysis of adhesions/scar bands (3 cases), lysis with placement of a skin graft over a stent (2 cases), placement of a skin graft over a stent (3 cases), mackenty flap, lysis of adhesions, and placement of a dental obturator (1 case), lysis of adhesions and placement of an obturator (3 cases), mucosal flap reconstruction (1 case), lysis of adhesions utilizing the Kazanjian two-stage technique (1 case), bilateral z-plasties (1 case), lysis of adhesions, placement of an obturator, and first-stage Kazanjian procedure (1 case), modified Z-plasty (1 case), laterally-based pharyngeal flap (2 cases), multiple procedures (including lysis, dilation, steroid injections, and local flaps/grafts) culminating in a jejunal free flap reconstruction (1 case), bilateral laterally-based posterior pharyngeal wall flaps (1 case), endoscopic intranasal repair with stenting; minor revision required (2 cases), combined transpalatal and endoscopic intranasal repair with stenting (1 case), lateral pharyngeal flap reconstruction with stenting (1 case), stricture release (using scalpel and coblator), application of feracrylum 3% gel, and placement of an indwelling infant feeding tube as a stent (1 case), pharyngoplasty without stenting (1 case)
Tonsillectomy technique: Among the recurrent cases where the initial technique was documented, electrocautery was used in 2 cases. Of the 8 cases where KTP laser was the recorded technique, 3 of these cases recurred. 1 case underwent adenotonsillectomy using a cold instrument. While the rest of the cases did not report the technique used.
Discussion
This systematic review, encompassing 166 documented cases of pharyngeal stenosis following adenotonsillectomy, provides a comprehensive analysis of one of the most challenging complications in otolaryngologic surgery. Our findings illuminate the multifaceted nature of this iatrogenic condition, spanning its epidemiological characteristics, etiological triggers, diverse clinical presentations, and the extensive array of management strategies employed with varying degrees of success.
The demographic data, with a nearly equal sex distribution and a mean age of 14.87 years, underscore that while predominantly a pediatric concern, this complication can present across a wide age spectrum, including adults.2,6,16 This broad age range highlights the necessity for vigilance among surgeons performing adenotonsillectomy in all patient groups. The overwhelming majority of cases were linked to adenotonsillectomy rather than isolated procedures, suggesting that the combined surgical trauma to both the oropharyngeal and nasopharyngeal tissues creates a more significant risk for opposing raw surfaces to adhere.2,5,16 The nasopharyngeal the most frequently involved site, consistent with the pathophysiology of soft palate adhesion to the posterior pharyngeal wall, a classic presentation of this complication.4,5,19
The latency period from initial surgery to symptom onset exhibited considerable variability, averaging just over 7 months but extending to several years. This insidious development reinforces the concept that pharyngeal stenosis is a dynamic process of fibrosis and scar contracture rather than an immediate postoperative event.5,16 Clinicians must maintain a high index of suspicion for this complication even remotely after surgery, particularly when patients present with the hallmark triad of symptoms: nasal obstruction, snoring, and dysphagia.1,4,16 The potential progression to obstructive sleep apnea, weight loss, and speech abnormalities signifies the severe functional impairment and diminished quality of life this condition can inflict.1,2,5
A critical finding of this review is the association between thermal energy-based surgical techniques and the development of stenosis. Electrocautery was the most commonly reported modality, followed by KTP laser and cobaltion.3,13,16 This suggests that thermal injury and the resultant tissue necrosis may be a significant predisposing factor for excessive scar formation, beyond the mere apposition of mucosal surfaces. It advocates for meticulous technique, judicious power settings, and the consideration of cold dissection in areas prone to cicatrization, particularly the inferior tonsillar poles and posterior pharyngeal wall.2,5,16
The management of pharyngeal stenosis remains notoriously difficult, as evidenced by the vast arsenal of over 40 different surgical techniques identified in this review. This heterogeneity itself signals the absence of a single gold-standard treatment and the tendency for this condition to be refractory to initial interventions. The fundamental principles of all successful techniques are universal: 1) complete release and excision of scar tissue to break the contracture and 2) resurfacing the resulting defect with healthy epithelium to prevent re-adhesion by secondary intention healing.5,14,15 The evolution from historical methods like obturators and skin grafts to the use of well-vascularized local flaps (eg, buccal mucosal, pharyngeal, uvular, palatal) represents a significant advance, as these flaps provide immediate mucosal coverage and improve wound healing.5,14,17,19 The high overall success rate of 85.2% (significant improvement) is encouraging but must be interpreted alongside a concerning recurrence rate of 25.4%.
The analysis of recurrent cases is particularly instructive. Recurrence was not confined to any single initial technique but was observed across a wide range of procedures, from simple lysis to complex flaps. This suggests that the underlying pathobiology—a patient’s innate propensity for keloid or hyperfibrotic healing—is a major driver of recurrence, sometimes overwhelming even the most sound surgical plan.2,13 Notably, the nasopharyngeal was the site of recurrence in the vast majority of cases, indicating its particular vulnerability, likely due to its complex muscular dynamics and narrower space compared to the oropharyngeal.4,5 The presence of revision surgery in the history of several recurrent cases implies that repeated trauma further amplifies the risk of aggressive scar reformation.2,16
The adjunctive use of anti-fibrotic agents has emerged as a pivotal strategy to combat recurrence. The application of mitomycin C, an alkylating agent that inhibits fibroblast proliferation, and the injection of corticosteroids like triamcinolone, which reduce collagen synthesis and inflammation, are now commonly integrated into surgical protocols to improve long-term patency.4,5,14 Their increasing use reflects a growing understanding of the condition at a cellular level and a move towards multimodal therapy.4,5,14
Furthermore, the role of postoperative stenting, as illustrated in our case report, remains a valuable, though debated, tool. Stents act as a physical barrier to prevent opposing raw surfaces from contacting during the critical healing phase. While prolonged stenting can be cumbersome and carries risks of infection and discomfort, its successful application in complex cases, including our own, demonstrates that it can be a crucial element in preventing recurrence when managed appropriately.4,18
Notably, the recurrence rate of 25.4% (32/126 cases) was disproportionately observed in patients whose initial adenotonsillectomy utilized thermal techniques, particularly the KTP laser, which recurred in 3 of 8 documented cases. This suggests that while electrocautery was the most commonly implicated modality, certain energy-based tools may confer an even greater risk of aggressive scar reformation. Furthermore, the high success rate of combined modality treatments—integrating surgical release, vascularized flaps, and anti-fibrotic agents—underscores that technical intervention alone is insufficient without addressing the underlying hyperfibrotic biology driving recurrence.
The persistently high recurrence rate observed in this review underscores the recalcitrant nature of pharyngeal stenosis, necessitating a paradigm shift towards long-term, multifaceted management strategies. Preoperative assessment, including computed tomography and nasopharyngoscopy, is indispensable for delineating the extent of fibrosis and precisely planning the surgical approach, particularly to address scarring at multiple levels or near the eustachian tube orifices. 23 Furthermore, the variability in healing and propensity for restenosis demand individualized, often prolonged, follow-up regimens extending beyond 6 to 12 months to detect late recurrence and manage sequelae such as chronic otitis media or velopharyngeal insufficiency. 25 This emphasizes that successful outcomes depend not only on the technical execution of the repair but also on meticulous preoperative planning and committed postoperative surveillance.
The persistence of pharyngeal stenosis despite surgical intervention highlights the complex interplay between surgical trauma and individual fibrotic response, which may be influenced by underlying genetic or immunological factors not yet fully characterized. This review underscores that while the initial mechanical insult—often from thermal techniques—creates the conditions for adhesion, the subsequent pathological wound healing is the primary driver of stenosis and its recurrence.26,30 Consequently, future management paradigms must extend beyond technical repair to incorporate a deeper understanding of fibrotic biology. This could involve pre-operative identification of high-risk patients, perhaps via biomarkers for keloid tendency, and the development of targeted anti-fibrotic pharmacotherapies to be used adjuvantly with surgery.24,30 A proactive, personalized medicine approach is therefore essential to mitigate the risk of this devastating complication.
Study Limitations
This review has several limitations inherent to its design. The analysis is based on case reports and series, which are susceptible to publication bias, as successful outcomes or unusual techniques are more likely to be reported than failures. The heterogeneity of the data precluded a formal meta-analysis. Furthermore, the long-term follow-up was variable and often limited, potentially underestimating the true recurrence rate, which may manifest many years later.
Clinical Implications and Future Directions
This analysis leads to several key conclusions and recommendations. First, prevention is paramount. Surgeons must employ meticulous technique, minimize mucosal damage—especially at the inferior poles—and use thermal energy judiciously. Second, management must be highly individualized based on the location, severity, and nature of the stenosis, as well as prior interventions. A shift towards multimodal treatment is advisable, combining precise surgical release, resurfacing with vascularized tissue (where possible), application of anti-fibrotic agents, and the considered use of temporary stenting in high-risk cases. Finally, patients and families should be counseled about the potential for recurrence and the possible need for multiple procedures. Future research should focus on standardized reporting of outcomes and prospective, multi-institutional studies to better evaluate the comparative effectiveness of these complex surgical approaches.
Conclusion
Pharyngeal stenosis, though rare, remains a severe complication of adenotonsillectomy, often associated with thermal surgical techniques and characterized by a high recurrence rate. This review underscores the importance of meticulous surgical technique to prevent its occurrence and highlights the necessity of individualized, multimodal management—incorporating surgical release, vascularized flaps, anti-fibrotic agents, and judicious stenting—to address its complex pathophysiology. Long-term follow-up is essential to monitor for recurrence and manage sequelae, emphasizing that both prevention and tailored intervention are critical to improving patient outcomes.
Footnotes
Ethical Considerations
This study is a systematic review based on already published data. In addition to displaying the case; therefore, ethical approval is not applicable. Written informed consent was obtained from the patient's legal guardian for publication of this case report and accompanying images.
Author Contribution
AAK: Conceptualization, methodology, validation, formal analysis, investigation, resources, writing—original draft preparation, writing—review and editing. AA and MAA: data curation, writing—review and editing. AM: supervision, methodology, writing—review and editing. All authors have read and agreed to the published version of this manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are embedded in the manuscript as secondary research.