
Abstract
Vocal fold process avulsion results from trauma that detaches the vocal process and thyroarytenoid muscle from the body of the arytenoid cartilage. Vocal fold laxity often causes severe dysphonia. Findings can be subtle. A high index of suspicion often permits diagnosis and effective surgical repair.
Vocal Fold Process Avulsion
This 42-year-old female with acquired tracheal stenosis who had undergone 10 laser and dilation procedures presented with dysphonia after her last procedure. Her laryngeal examination showed that the left vocal process with musculomembranous vocal fold was separated from the arytenoid cartilage (Figure 1). The left vocal fold process avulsion was reconstructed successfully using a figure-of-8 suture (Figure 2).
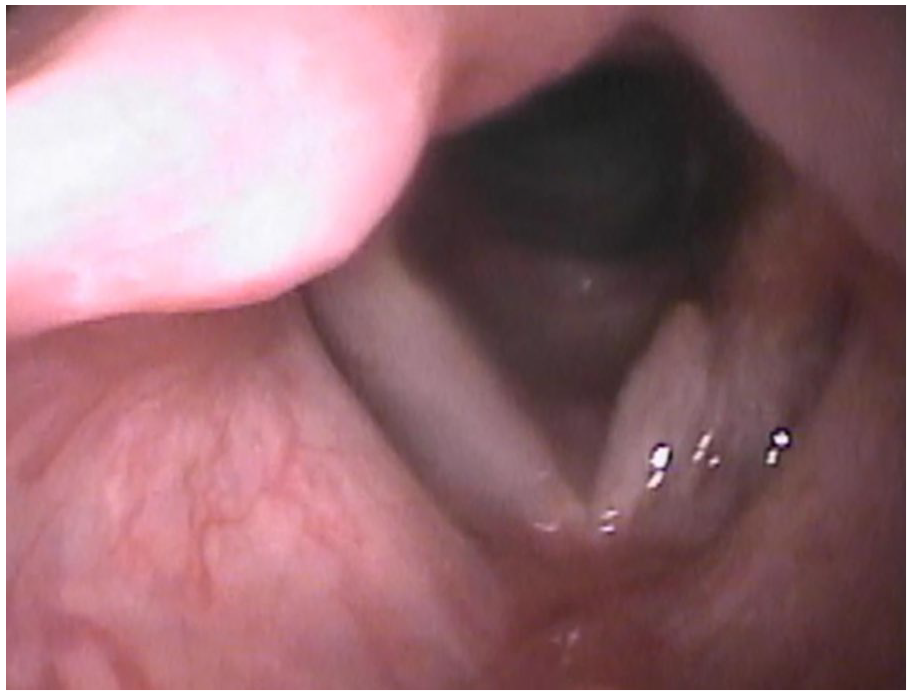
Left vocal process avulsion.

Reconstructed left vocal fold process.
Discussion
There is still a small indentation because of deficient vocalis muscle, but tension has been restored and voice quality remained improved markedly a year after surgery. Vocal fold process avulsion is the separation of the vocal fold process from the body of the arytenoid cartilage and frequently presents with dysphonia, as well as shortness of breath especially on phonation. 1 Avulsion should always be suspected after traumatic intubation or laryngeal procedures and is evaluated best with the strobovideolaryngostcopy. Laryngeal computed tomography occasionally is helpful. Observation of a freely moving vocal fold process during breathing or phonation, thyroarytenoid muscle laxity sometimes with a medial muscle bulge within the vocal fold, and correction of vocal process angulation with pressure from the contralateral vocal process suggest the diagnosis which is confirmed through intraoperative palpation of the defect. 1 This injury can present in children, due to the susceptibility of smaller airways to injury from trauma. 2 Acute avulsion can present with airway compromise due to hematoma expansion. So, the index of suspicion should remain high, and airway management should be a priority, and laryngeal function should be evaluated only if the patient is not in acute distress. 3 Repair may be performed endoscopically, depending on the extent of the surrounding damage. Chemical tenotomy with botulinum toxin, closed reduction with suture, and open reduction via cordotomy are appropriate. 4
Footnotes
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases or case series.