
Abstract
Renal cell carcinoma (RCC) is characterized by a marked metastatic potential and is the third most common cancer of metastasis to the head and neck, following breast and lung cancer. We report a rare case of a patient with RCC with metastasis to the tongue. A 72-year-old man visited our otorhinolaryngology clinic complaining of tongue pain and ulcerative lesions which occurred 3 weeks before. The patient had been diagnosed with RCC and received a right radical nephrectomy 3 years previously. Because the lesion was suspected to be malignant, a hemiglossectomy was planned. However, metastatic lesions were suspected on the left upper lung and the left 10th ribs in imaging studies and the result of an incisional biopsy revealed tongue metastasis of RCC. RCC metastasis to the tongue is extremely rare. Only 51 cases were reported worldwide from 1911 to 2017. According to the literature, no case of RCC metastasis to the tongue has been reported to date in Korea. Therefore, we report this case along with a review of the literature.
Introduction
Metastasis of cancer to the oral cavity is very rare, accounting for about 1% of all oral malignant tumors.1,2,3 Metastasis to the tongue is extremely rare and its incidence is 0.17%. 4 Renal cell carcinoma (RCC) is characterized by a marked metastatic potential and is the third most common cancer to metastasize to the head and neck, following breast and lung cancer. 5 Because of this characteristic of RCC, distant metastasis is observed at the time of primary RCC diagnosis in 25%-30% of RCC patients. Even after surgical treatment at an early stage, recurrence or metastasis has been reported in 50% of patients. 6 Most of the metastatic lesions are found within 3 years after surgery. 6 A literature review found that 51 cases of RCC metastasized to the tongue were reported worldwide from 1911 to 2017. 6 We report a rare case of a patient with RCC metastasis to the tongue.
Case Report
A 72-year-old man visited our otorhinolaryngology clinic complaining of tongue pain and ulcerative lesions which occurred 3 weeks before. The oral lesion was a rapidly growing, protruding, occasionally hemorrhagic mass. An examination of his oral cavity showed a 1 cm-sized protruding mass involving the right anterolateral one-third of the tongue (Figure 1A). There were no palpable lymph nodes on either side of the neck and no other specific findings were found, except for otomycosis of the right eardrum in the physical examination using a laryngoscope. His social history included heavy smoking and he drank every day. A heterogeneous enhancing mass was confirmed on the anterolateral tongue on the neck computed tomography (CT) scan, and no neck lymph node metastasis was identified (Figure 1B). He visited a local clinic because of gross hematuria 3 years ago and a 1-cm-sized mass in his right kidney was found on an abdominal CT. After the diagnosis of RCC, a right renal nephrectomy and right adrenalectomy were performed in our urology service. At that time, the pathologic finding was clear cell RCC. One month after surgery, interferon alpha therapy was initiated and positron emission tomographic-computed tomography and chest CT were performed to check for recurrence or metastasis. There was no suspicion of recurrence and the patient did not voluntarily visit after 2 years.
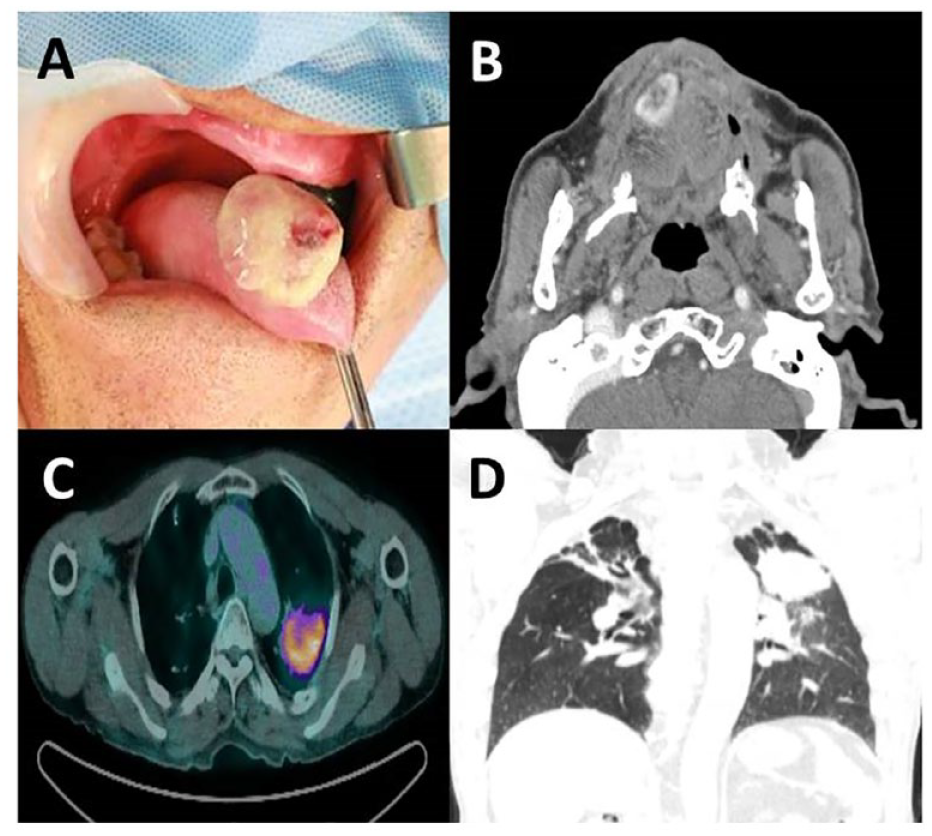
A 2 cm-sized protruding mass on the right tongue (A) and heterogeneous enhancing mass at the right tongue anterior portion on neck computed tomography (CT) (B). About a 5.2 cm-sized fluorodeoxyglucose-avid mass in the left upper lung (C) and a 5 cm-sized lung mass in the left upper lung on high-resolution chest CT (D).
A hemiglossectomy was planned after an incisional biopsy and staging by PET/CT and neck magnetic resonance imaging. However, histologic features of the tongue mass suggested that it was probably RCC (Figure 2). In addition, a preoperative chest X-ray showed a 5 cm-sized mass-like lesion on the left upper lung (Figure 1D). Bone metastasis in the left 10th rib with lung metastasis was found by PET/CT (Figure 1C).
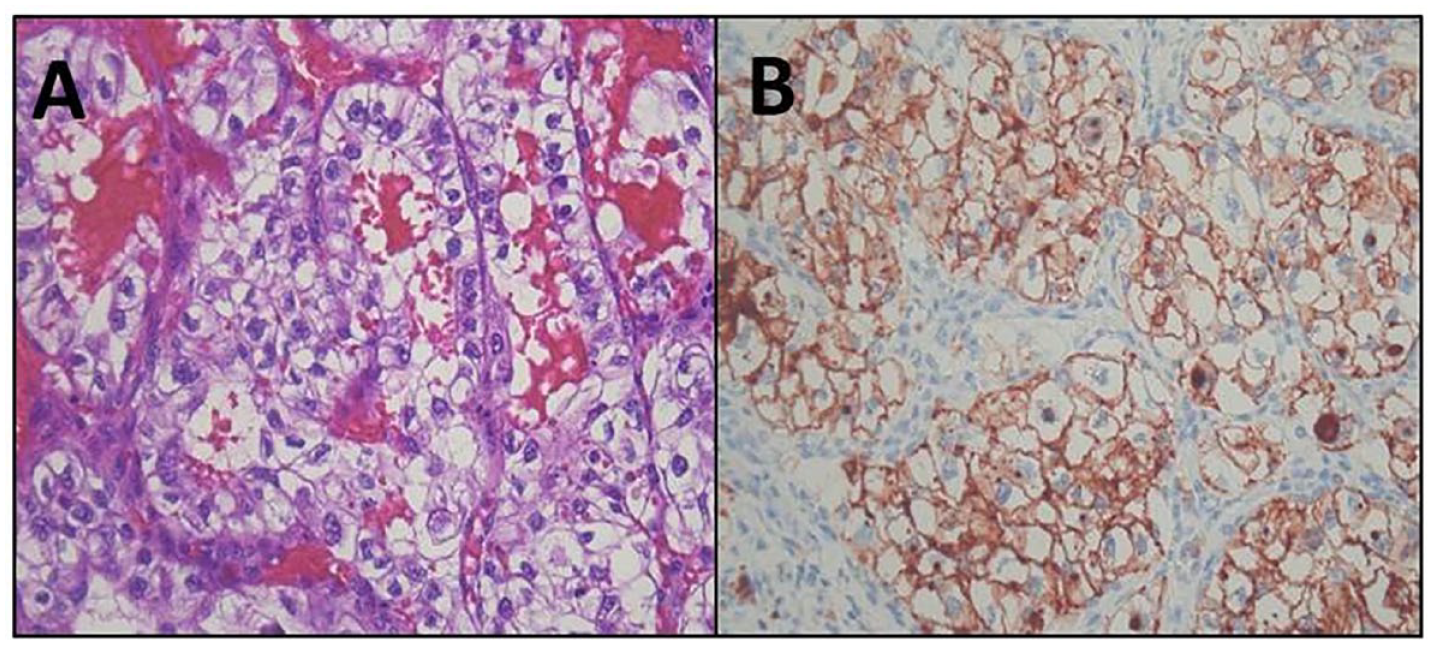
The tumor cells are arranged in acinar patterns, with abundant clear cytoplasm (H&E stain ×200) (A) and strong immunoreactivity to CD10 (×200) (B).
The patient’s tongue lesion grew twice as large in 3 weeks and was accompanied by persistent tongue pain, so a partial glossectomy was done to control the symptoms and prevent any possible complications. Immuno-histochemical findings of the tumor cells show strong immunoreactivity against CD10 (×200) (Figure 2B). Our patient was referred to our oncology department for consultation. At the time of this writing, sunitinib therapy (multitarget tyrosine kinase inhibitors) in our oncology department was planned.
Discussion
RCC metastasis to the tongue is extremely rare. Only 51 cases were reported worldwide from 1911 to 2017. Two-thirds of these occurred in men and the mean age was 59 years. No case of RCC metastasis to the tongue has been reported to date in Korea. This case is meaningful as the first case of tongue metastasis of RCC in Korea.
The distant metastasis of RCC is very common and occurs in multiple organs, mainly in the lung (50%), bone, liver (30%), and head and neck (12%). 6 Among them, only 1% of RCCs metastasize to the tongue. 6 To date, the mechanism of this metastasis is thought to be hematogenous through the arteries, veins, or lymph nodes. Metastasis to the head and neck can spread distantly through the Bastone (paravertebral) venous plexus without lung involvement but is generally associated with lung metastasis. 4 Even in this case, the PET/CT scans showed lung and bone metastases.
Metastatic RCC is associated with a poor prognosis. The 5-year survival rate is less than 10% and the average life expectancy is 5.8 months.4,5 The treatment of tongue metastasis, such as surgical resection, chemotherapy, and immunotherapy, is usually palliative. Surgical treatment is performed to reduce the symptoms and discomfort of the patient. In recent years, several new treatments have been developed. These include multitargeted tyrosine kinase inhibitors, monoclonal vascular endothelial growth factor-antibody, mammalian target of rapamycin inhibitors, and immunotherapy.7,8 The prognosis for metastatic RCC is improving due to the development of these new therapies. 5
The patient was diagnosed with RCC 3 years ago and received a right radical nephrectomy and right adrenalectomy at that time. He was referred to our hospital with pain in the anterior tongue and a hemorrhagic episode. Because the lesion was suspected to be malignant, an incisional biopsy and staging were performed, and a hemiglossectomy was planned. However, metastatic lesions were suspected on the left upper lung and left 10th ribs in imaging studies and the result of an incisional biopsy revealed tongue metastasis of his RCC.
A wide excision was performed to reduce pain caused by the mass and to manage possible complications. Immunohistochemical tests showed strong immunoreactivity to CD10. The results of a percutaneous transthoracic needle biopsy performed at the time of staging showed positive staining with cytokeratin, CD10, and vimentin markers. Ultimately, metastases to the tongue, lung, and bone were confirmed. After surgery, the patient was referred to the oncology service and was recommended for immunotherapy or targeted therapy.
RCC is a tumor with a high metastatic potential to the head and neck. Tongue metastasis of RCC should not be ruled out if there is a clinical suspicion of tongue cancer. In addition, unlike this case, there are several reports in which tongue metastasis of RCC appeared as an initial presentation, so it should be considered in the early stage of the differential diagnosis. Since previous cases of tongue metastases tended to have multiple systemic metastases, the possibility of other distant metastases at the time of the diagnosis should be considered. Therefore, it is important to select the appropriate treatment for the patient considering the prognosis after staging.
Conclusion
RCC has a high potential for metastatic spread to the head and neck but metastasis to the tongue is extremely rare. To date, only 51 cases have been reported worldwide. This case is the first case of tongue metastasis from RCC in Korea. This case highlights the fact that tongue metastasis of RCC should not be ruled out if there is a clinical suspicion of tongue cancer. Previous studies have reported several cases in which the tongue metastasis of RCC appeared as an initial presentation; thus, the possibility of distant metastasis should be considered. Because the prognosis is poor in most cases, it is important to choose a treatment considering the patient’s quality of life after staging.
Footnotes
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This paper was supported by Fund of Biomedial Research Institute, Jeonbuk National University Hospital.
Ethics Statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee.
Research Involving Human Participants and/or Animals
Not indicated.
Informed Consent
Not indicated.