
Abstract
Objective
We aimed to establish and validate nomograms to evaluate overall survival (OS) and cancer-specific survival (CSS) in patients with metastatic renal cell carcinoma (MRCC).
Methods
Between 2010 and 2015, the clinical information of patients with MRCC was selected using the Surveillance, Epidemiology, and End Results database. Two nomograms were constructed based on Cox regression analysis, and their prediction accuracy was evaluated by concordance index (C-index), receiver operating characteristic (ROC) curve, and decision curve analysis (DCA).
Results
After propensity score matching, there were 568 patients with MRCC in the training group and 568 in the validation group. Multivariate analyses revealed that age, residence, pathology, T stage, N stage, surgery, and metastatic sites were independent prognostic factors for the OS and CSS of MRCC. The C-index and ROC curves indicated that the two nomograms of OS and CSS showed satisfactory discriminative power. Furthermore, DCA displayed that the nomograms achieved more clinical net benefit than the American Joint Committee on Cancer staging system.
Conclusion
We constructed and validated two effective prognostic nomograms for patients with MRCC that accurately predicted the probabilities of 1-, 2-, and 3-year OS and CSS.
Keywords
Introduction
Renal cell carcinoma (RCC) is one of the most frequent cancers in the genitourinary system, accounting for 3% of all adult cancers. 1 The global incidence of RCC has increased by approximately 2% each year throughout the past two decades. 2 Despite the increased use of medical imaging technology, approximately 30% of patients are still initially diagnosed with metastatic renal cell carcinoma (MRCC). 3 Owing to the poor prognosis of patients with MRCC and the median survival of 4 to 20 months, more active management for these patients is needed.4–5
Currently, The American Joint Committee on Cancer (AJCC) TNM staging system is most commonly applied to assess the prognosis of patients with RCC. 6 However, numerous studies have demonstrated that other factors, including age, pathology, surgery, and metastatic sites, are also related to the prognosis of patients with MRCC. 7 Therefore, the AJCC staging system has become less effective in predicting individual survival rates.
The identification of independent risk factors for patients with MRCC is urgently needed. Nomogram-based clinical modeling combining and quantifying all risk factors is an intuitive approach that has played a major role in predictive analysis and cancer management in recent years.8–9 Accurate prediction of the prognosis of patients with MRCC helps clinicians and patients determine an appropriate treatment strategy. Accordingly, using a large and reliable dataset from the Surveillance, Epidemiology, and End Results (SEER) database, 10 we aimed to establish nomograms to predict overall survival (OS) and cancer-specific survival (CSS) for patients with MRCC and assess their prediction accuracy.
Materials and methods
Patients and variables
The SEER Program supported by the National Cancer Institute is an authoritative source from 18 tumor registration centers containing approximately 30% of the United States population. 11 Specific clinical parameters and prognostic outcomes of patients with MRCC from 2010 to 2015 were collected from the SEER database using reference number 14622-Nov2017. The present research did not require local ethics approval or informed patient consent because SEER is a public database. The main factors analyzed included age at diagnosis, race, sex, laterality, grade, histological type, histological type, tumor size (<180 mm), AJCC 6th edition staging system, survival status, median household income, residential area, surgery, survival months, and metastatic sites. The ICD-O-3 histology code (8312/3) was RCC, which included Xp11.2 translocation carcinomas, carcinoma associated with neuroblastoma, mucinous tubular and spindle cell carcinoma, and RCC unclassified.
We excluded the following patients: unknown histological type (n = 89), unknown treatment (n = 6), unknown race (n = 4), bilateral renal tumor (n = 3), or tumor size >180 mm (n = 73). Finally, patients with MRCC were identified from the SEER database and randomly divided into the training cohort and validation group with a ratio of 1:1.
Follow-up
The last follow-up was conducted in December 2015. OS and CSS were the primary endpoints of the present research. OS was analyzed from the time of initial diagnosis to death from all causes or the last follow-up with the patient still alive. CSS was recorded from diagnosis to death caused by MRCC or the last follow-up.
Statistical analysis
The categorical variables were expressed as percentages and analyzed by a chi-squared test. The X-tile program (Yale University, New Haven, CT, USA), which has been applied to define the best cutoff values of continuous variables for patients with breast cancer, 12 was used to determine the optimal cutoff values of age at diagnosis and tumor size.
Propensity score matching (PSM) was performed to achieve a balance in baseline factors with a ratio of 1:1 between the two groups. The independent prognostic factors of OS and CSS were determined by univariate and multivariate Cox analyses of the training cohort. Variables in the univariate Cox regression analysis with P < 0.1 were included in the multivariate Cox regression analysis. On the basis of the outcomes of multivariate Cox regression analysis in the training cohort, we constructed two nomograms of OS and CSS using the “rms” and “survival” packages in R (www.r-project.org).
The concordance index (C-index) was determined to evaluate discriminative ability. The area under the time-dependent receiver operating characteristic curve (time-dependent AUC) was applied to determine the sensitivity and specificity of nomograms. Bootstrapping with 1000 resamples was performed for the C-index and receiver operating characteristic curve evaluations. C-index and AUC values ranged from 0.5 to 1.0, with 0.5 representing a random probability and 1.0 indicating a perfect discriminatory performance. 13 Generally, C-index and AUC values larger than 0.7 indicate a reasonable performance of the nomogram. Furthermore, decision curve analysis (DCA) was used to estimate the clinical benefit of alternative models by quantifying net benefits at various threshold probabilities14–15 and assess the use of two nomograms compared with the AJCC staging system in this study.
IBM SPSS Statistics for Windows, Version 25.0 software (IBM Corp., Armonk, NY, USA) and R version 4.0.3 (www.r-project.org) were used for all statistical analyses, and a two-tailed P < 0.05 indicated statistical significance. This report adheres to the strengthening the reporting of observational Studies in Equator network (STROBE) guideline. 16
Results
Patient characteristics
From 2010 to 2015, 1376 patients with MRCC were identified. The clinicopathological characteristics of the study population are summarized in Table 1. A total of 1201 eligible patients were selected as the training cohort (n = 601) and validation group (n = 600) (Supplementary S1). After PSM, there were 568 cases in both groups. In the training cohort, the main categorical variables were 57 to 77 years old (58.3%), White (75.9%), men (71.1%), grade unknown (44.7%), left tumor (53.2%), T3 (46.3%), <93-mm tumor size (59.0%), surgery (50%), N0 stage (63.9%), clear cell carcinoma (56.9%), only lung metastasis (34.5%), $50,000 to $75,000 household income (51.6%), and urban (95.2%). In the validation group, the main categorical variables were 57 to 77 years old (58.5%), White (74.8%), men (73.4%), grade unknown (42.6%), left tumor (53.0%), T3 (46.5%), <93 mm tumor size (57.7%), surgery (51.9%), N0 stage (63.4%), clear cell carcinoma (57.2%), only lung metastasis (33.6%), $50,000 to $75,000 household income (51.6%), and urban (94.4%). The best cutoff value for age at initial diagnosis and tumor size were determined using X-tile according to survival status. The optimal age cutoff values were 57 and 77 years old for age at diagnosis and 93 mm and 127 mm for tumor size (Supplementary S2).
The demographic and pathological characteristics of included patients in the entire cohort and propensity score-matched cohort.

Nomogram construction and validation
Independent risk predictors were identified by Cox regression model analyses. Two nomograms of OS and CSS were constructed based on the independent prognostic factors (Figure 1), which included age, histologic type, T stage, N stage, surgery, residence, and metastatic sites in the training cohort (Tables 2 and 3). By adding the points for each significant factor located on the total points axis at the bottom of the nomogram and projecting total points on the survival scale, clinicians were able to predict the probabilities of 1-, 2-, and 3-year OS and CSS.

Nomograms to predict the 1-, 2-, and 3-year overall survival (OS) and cancer-specific survival (CSS) rates of patients with metastatic kidney cancer. (a) The predicted 1-, 2-, and 3-year OS rate and (b) The predicted 1-, 2-, and 3-year CSS rate.
Univariate and multivariate cox analyses of prognostic factors associated with the overall survival of patients with metastatic renal cell carcinoma in the development cohort.
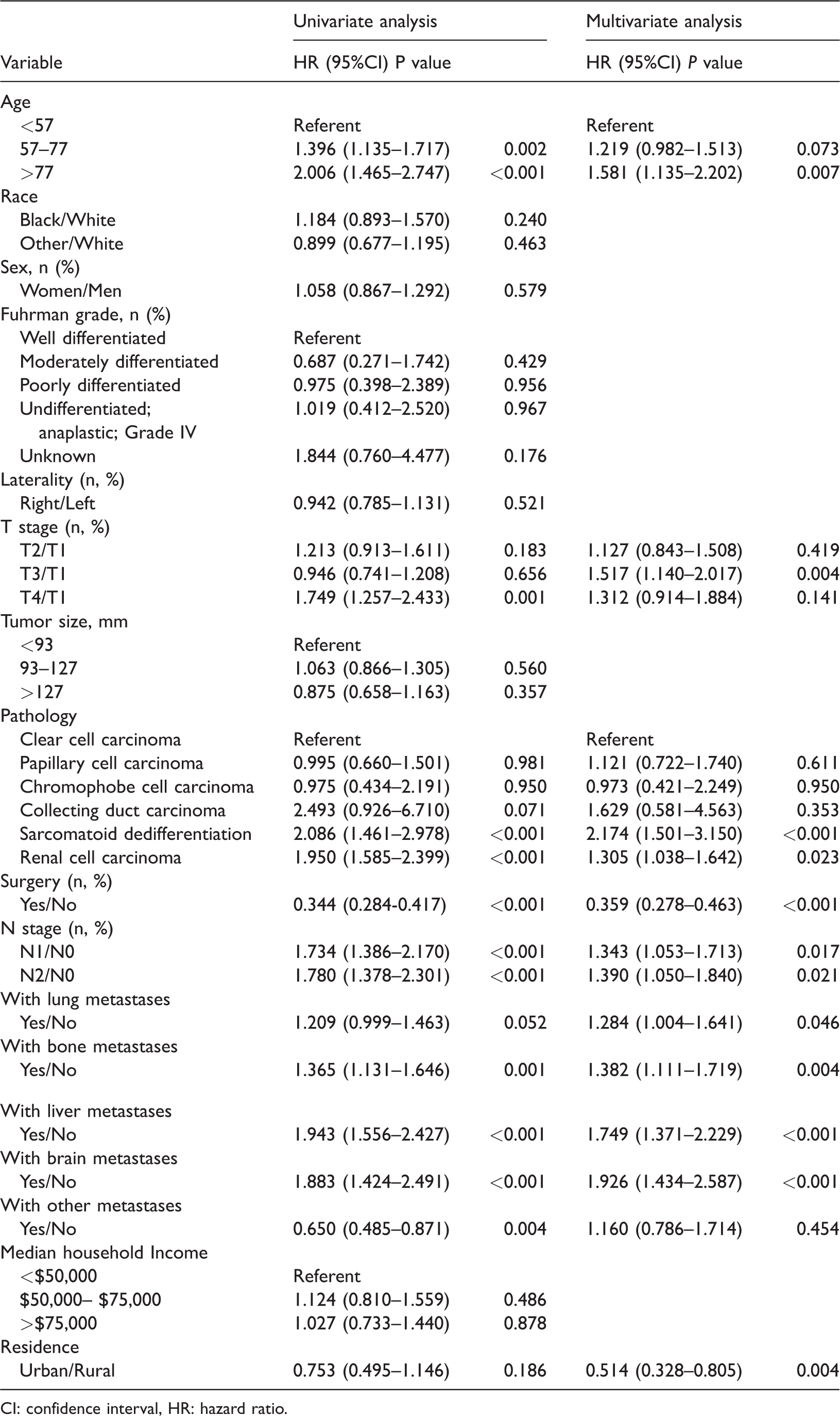
CI: confidence interval, HR: hazard ratio.
Univariate and multivariate cox analyses of prognostic factors associated with the cancer-specific survival of patients with metastatic renal cell carcinoma in the development cohort.

CI: confidence interval, HR: hazard ratio.
The OS and CSS nomograms were internally and externally well validated. The C-index value of the nomogram for predicting OS was 0.724 (95% confidence interval [CI] 0.700–0.748) for the internal verification and 0.710 (95% CI 0.686–0.734) for the external validation. Moreover, this value was 0.729 (95% CI 0.705–0.753) and 0.712 (95% CI 0.687–0.737) for predicting CSS in the internal and external validation, respectively (Table 4). The time-dependent AUC values were >0.7 for the prediction of 1-, 2-, and 3-year OS and CSS in the training group and validation cohort (Figure 2), indicating that the nomograms had good discriminatory performance.
The C-indices for the predictions of OS and CSS in the training cohort and validation group.
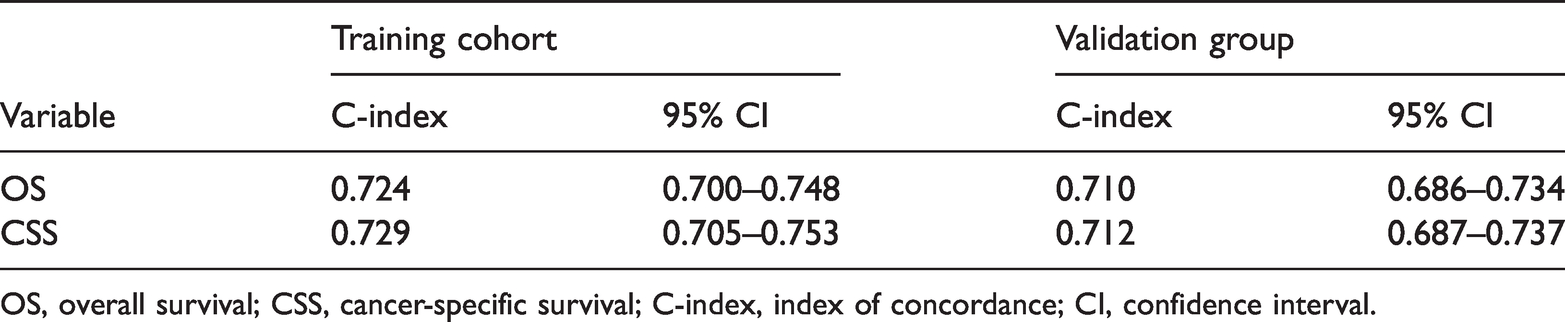
OS, overall survival; CSS, cancer-specific survival; C-index, index of concordance; CI, confidence interval.
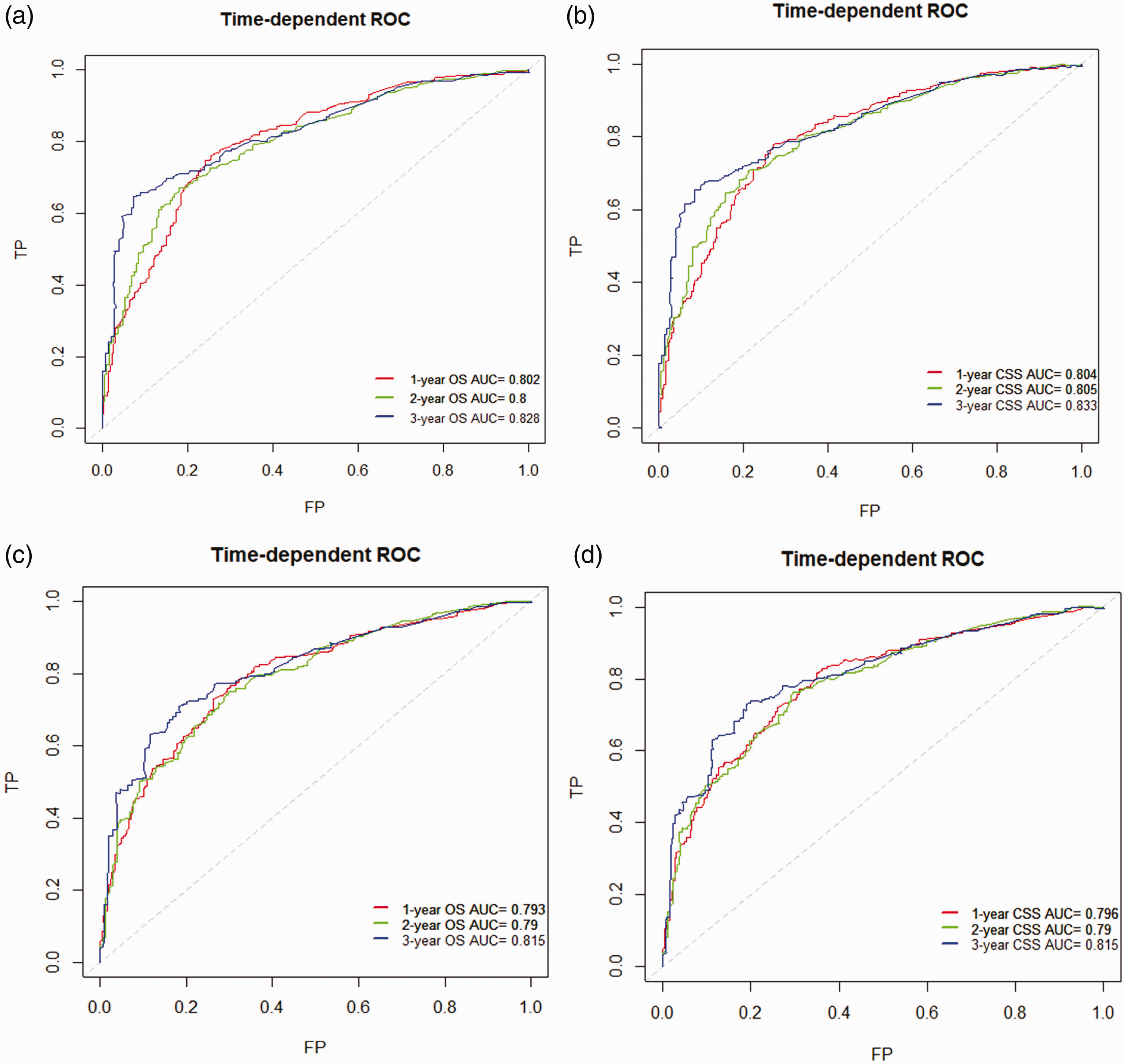
Receiver operating characteristic (ROC) curves to internally and externally verify the accuracy of the nomograms in predicting 1-, 2-, and 3-year overall survival (OS) and cancer-specific survival (CSS) in patients with metastatic kidney cancer. (a) Verifying 1-, 2-, and 3-year OS in the training group (TP: true positive, FP: false positive, AUC, area under the curve). (b) Verifying 1-, 2-, and 3-year CSS in the training group. (c) Verifying 1-, 2-, and 3-year OS in the validation cohort and (d) Verifying 1-, 2-, and 3-year CSS in the validation cohort.
The DCA results also demonstrated that the two nomograms showed a significantly better performance compared with that of the AJCC staging system (Figure 3). In general, the OS and CSS nomograms for patients with MRCC had significant discrimination and calibration abilities.

Decision curve analysis demonstrating the net benefit of nomograms and The American Joint Committee on Cancer (AJCC) staging system for the prediction of prognosis in patients with metastatic kidney cancer. (a) Overall survival (OS) and (b) cancer-specific survival (CSS) in the training cohort. (c) OS and (d) CSS in the validation group.
Discussion
In recent decades, approximately one-third of patients initially diagnosed with RCC have presented with locally aggressive tumors or distant metastasis. Distant metastasis severely influences patients' quality of life and significantly reduces their survival time. 17 In the RENSUR3 study, the median survival time of patients with MRCC in the entire cohort was 11.9 months. 5 In India and Brazil, the median survival times were 12.87 months and 14.1 months, respectively. 5 Similarly, the median survival time was 11 months for patients with MRCC from the SEER database. Given the poor prognosis of patients with MRCC, the medical community is now paying more attention to clinical prognostic evaluation and individualized therapeutic management. In this context, we are actively committed to constructing nomograms of OS and CSS for MRCC that can help clinicians and patients predict survival times and select optimal management strategies.
At present, the prognosis of RCC patients is evaluated mainly based on the AJCC and Fuhrman pathological grading system. However, multiple patient factors cannot be evaluated both individually and completely, which may result in some bias. Therefore, we analyzed confounding variables by Cox regression model analyses and identified independent prognostic factors of patients with MRCC, which included age, residential area, pathological type, stage, surgery, and metastatic sites. In contrast, tumor size, sex, and race were not independent risk factors. Then, we incorporated the above independent predictors into nomograms to predict the 1-, 2-, and 3-year OS and CSS of patients with MRCC. Nomograms play a critical role in individual prognostic prediction and personalized therapeutic management. 18 Finally, the accuracy of the two nomograms was validated internally and externally, and DCA confirmed that our nomograms predicted outcomes with a better clinical benefit than the AJCC staging system.
Previously, several studies subjectively categorized patients into diverse tumor size cohorts and age groups, which might lead to a statistical bias. 12 To address this issue, we applied X-tile to define the best cutoff value for tumor size and age at initial diagnosis based on survival status and survival time. Some scholars reported that compared with younger age at diagnosis (<57 years), older age at initial diagnosis was an adverse factor for patients with MRCC. 19 Similar to the above research, the Cox regression analysis in this study showed that increased age at initial diagnosis was a significant risk factor for a worse prognosis.
It is universally acknowledged that patients with RCC are prone to metastasis to multiple organs, including the lungs, brain, bone tissue, and liver. Similar to a previous study, 20 we found that an increased number of metastatic sites was significantly related to a poor prognosis. Currently, whether surgical resection obtains survival benefits for patients with MRCC remains controversial. Several researchers have reported that nephrectomy did not significantly improve the survival rate of patients with the metastasis of MRCC to multiple organs, which subsequently led to a significantly higher rate of 6-month mortality after surgery. 21 In addition, Méjean et al. used a prediction model to classify patients with MRCC into intermediate-risk or poor-risk groups and indicated that the efficacy of sunitinib treatment alone was comparable to that of sunitinib treatment after nephrectomy. 22 Accordingly, nephrectomy appeared to not be necessary for patients with MRCC. However, in the study by Culp et al., 21 patients who underwent surgery had distinctly lower kidney cancer-special mortality (66.3% vs. 90.8%, P < 0.001) and all-cause mortality (70.5% vs. 92.7%, P < 0.001) than those who did not. Other scholars11,23 demonstrated that nephrectomy was an independent prognostic factor for survival benefits, even in patients with MRCC, although all known tumors showed incomplete resection. According to our nomogram, surgery achieves the highest score in patients with MRCC based on survival time and survival status and may be an important prognostic indicator for these patients.
The association between the living location and survival status of patients with MRCC has been rarely reported. In our study, compared with patients with MRCC living in rural areas, patients living in urban areas had a lower risk of death (OS: hazard ratio [HR] = 0.514; 95% CI = 0.328–0.805, P < 0.004; CSS: HR = 0.471; 95% CI = 0.300–0.740, P < 0.001). According to our nomogram, patients living in rural areas achieved a high score, indicating that rural areas had a serious adverse impact on the OS and CSS of MRCC. The most likely explanation is that patients living in rural areas may have limited access to rudimentary medical facilities. The pathology of RCC also played a significant role in personal prognostic prediction. Previous reports have shown that patients with clear cell carcinoma had a more favorable prognosis compared with patients with other histological types. 18 In addition, among patients with MRCC, those with clear cell carcinoma had a better prognosis than patients with non-clear cell carcinoma (31 vs. 24 months) in the multicenter Korean registry. 5 Similar to our result, patients with clear cell carcinoma exhibited a better prognosis than patients with non-clear cell carcinoma tissue types. Moreover, compared with clear cell carcinoma, collecting duct carcinoma and sarcomatoid dedifferentiation tissue types were significantly related to a worse prognosis according to our constructed nomogram.
Regarding RCC, T stage has been demonstrated to be a significant risk factor for patient prognosis. 21 Based on the AJCC staging system, patients with pT3 and pT4 RCC show the following features: perirenal fat involvement, tumor thrombus, direct ipsilateral adrenal invasion, and extension beyond Gerota’s fascia. Previous reports have revealed that perirenal fat involvement, tumor thrombus, direct ipsilateral adrenal gland invasion, and Gerota fascia invasion were significantly related to a poor prognosis. Furthermore, compared with patients with pT3 RCC without adrenal invasion, patients with direct adrenal gland involvement have a worse prognosis. 24 According to our nomograms, patients with pT3 and pT4 MRCC obtained a high score and displayed unfavorable survival outcomes. Adrenal invasion was classified into the pT3 stage based on the 6th edition of the AJCC staging system, and we think this may be the main reason why patients with pT3 disease earned a higher score.
In recent decades, multiple scholars have reported that lymph node invasion is a significant risk factor for survival in patients with MRCC.5,21 In the present study, the roles of lymph node status in our constructed nomograms were consistent with those in previous reports, and the multivariable Cox regression model showed that N stage was inversely related to patient prognosis. Currently, there are limited reports regarding the specific number and location of metastatic sites in patients with MRCC. One study reported that the lung was the most common metastatic organ in 342 patients with MRCC. 25 Another study showed that the metastatic sites of 231 patients, such as the lung, bone, or liver, had a negative effect on the OS and CSS of MRCC, and liver metastasis had the worst prognosis among these three metastatic organs. 11 In our analysis, the lung only was the most frequent metastatic location, followed by both lung and bone metastasis. In addition, brain metastasis had the highest score among the metastatic sites, including the liver only, lung only, bone only, and brain only. Moreover, patients with multiple distant organ metastases showed a significant decrease in survival time compared with patients with solitary solid organ metastasis.
Although the registration information of patients with MRCC in the SEER database was summarized in detail, the present study has some limitations. First, we could not obtain more information from the SEER database, such as comorbidities, personal performance status, smoking status, laboratory tests, and treatment information, which might result in some bias. In addition, immune checkpoint inhibitors for patients with MRCC have been introduced in recent years. If the SEER database provides immunotherapy information in the future, comprehensive prediction nomograms may achieve improved prediction and personalized medical treatment. Finally, our constructed prediction model requires more multi-center, large sample data for repeated validation in the future.
Conclusion
Despite these limitations, our current research provides insight into the prognosis of patients with MRCC. The OS and CSS nomograms were internally and externally verified, which confirmed the accuracy and reliability of these models. At present, these models can be used to predict the prognostic outcomes of patients with MRCC and identify individualized therapeutic methods.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605221105367 - Supplemental material for Construction and validation of a novel prognostic nomogram for patients with metastatic renal cell carcinoma: a SEER-based study
Supplemental material, sj-pdf-1-imr-10.1177_03000605221105367 for Construction and validation of a novel prognostic nomogram for patients with metastatic renal cell carcinoma: a SEER-based study by Zhaoxiang Lu, Wei He, Jun Zhou, Cheng Yang and Rong Xiang in Journal of International Medical Research
Footnotes
Author contributions
Investigation: Zhaoxiang Lu, Wei He.
Methodology: Zhaoxiang Lu, Rong Xiang.
Supervision: Jun Zhou, Wei He, Cheng Yang.
Validation: Rong Xiang.
Writing – original draft: Zhaoxiang Lu, Jun Zhou.
Writing – review & editing: Zhaoxiang Lu
Declaration of conflicting interest
The authors have no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Science Research Fund Project of Anhui Medical University in Anhui Province (2019XKJ166), Natural Science Fund of the University of Anhui Province (KJ2018A0457), College Excellent Youth Talent Support Program of Anhui Province (gxyq2019081), and Open Fund for Discipline Construction, Institute of Physical Science and Information Technology, Anhui University (OEIAM202008).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.