
Abstract
We present a case of metastatic renal cell carcinoma (RCC) to the petroclival region with clinical symptoms manifested as posterior cranial neuropathies. A 65-year-old male presented with headache symptom for over 1 year, during which time he was diagnosed with RCC and underwent right nephrectomy. However, the headache symptom and cranial neuropathies had been attributed to cranial neuritis all the time until the surgical removal of metastatic tumor in the petroclival region led to the diagnosis of metastatic RCC. RCC has a tendency for metastasis early. The incidence of spread of RCC to brain is a rarity in clinical practice. When a patient presents with cranial nerve neuropathies, the possibility of metastatic RCC should be sought. Brain metastases display nonspecific presentations, and it is useful to examine with magnetic resonance imaging and computed tomography scans radiologically.
Introduction
Renal cell carcinoma (RCC) is a rare malignant tumor, accounting for 3% of all diagnosed malignancies in adults and 90% of renal tumors. 1 Current classification subdivides RCC into 5 types based on growth patterns, cellular origins, and genetic alterations, including clear cell RCC, collecting duct carcinoma, chromophobe RCC, papillary RCC, and unclassified RCC. 2 Clear cell renal cell carcinoma (ccRCC) accounts for 75% of RCC and arises from epithelial cells of the proximal tubules.
RCC is clinically silent and receives little attention at an early stage. About one-third of patients have distant metastases at the time at which the diagnosis of RCC is confirmed.3,4 Over 25% of patients will develop metastatic disease even treated for primary tumor. 5 RCC has a tendency for metastasis early, with the lung, local lymph node, bone, liver, and adrenal gland being the most common sites.6,7 The incidence of spread of RCC to brain is a rarity in clinical practice, in this paper, we present a rare case of metastatic ccRCC to the petroclival region with clinical symptoms manifested as posterior cranial neuropathies.
Case Presentation
A 65 year-old male was referred to our institution with a 1 year history of recurrent headaches and found a space-occupying lesion in the petroclival region on the left side for 10 days. The patient reported a left-sided headache and numb sensation in the occipital region 1 year ago. A few months later, he presented with complaints of palsies of left cranial nerves manifesting as hoarseness, dysphonia, dys-expectoration, and hearing loss in the left ear. Total body positron emission tomography-computed tomography (CT) scan demonstrated no uptake in the skull base. He was diagnosed with mastoiditis and cranial neuritis and given a prescription of corticosteroids which was not effective. An enhanced CT of the abdomen revealed a heterogeneously enhanced solid renal mass suspicious of RCC 5 months ago. Preoperative electromyography indicated neurogenic injury of posterior cranial nerves, especially accessory nerve. Subsequently, the patient underwent a radical nephrectomy of the right kidney in outside hospital. Histopathologic examination, confirming the diagnosis of RCC, revealed clear cell renal carcinoma with focal sarcomatoid features (WHO/International Society of Urological Pathology nuclear classification: Grade 4) (Figure 1). However, there was no improvement in headaches after surgery. CT and magnetic resonance imaging (MRI) of the brain with contrast showed altered signal intensity of the petroclival region on the left side (Figure 2) 10 days ago. Then he presented to the otolaryngology department of our institution. At admission, poor spirit and appetite as well as loss of weight were seen in this patient. His examination revealed immobility and abduction paralysis of the left vocal cord, smoothing out of the left nasolabial fold, atrophy of the left lingual muscle with extended tongue left deviation, and inadequate closure of the soft palate. After a thorough preoperative examination, the patient underwent an endoscopic transmastoid exploration of the tumor in the petroclival region. Extension of the tumor to the jugular foramen area and bone destruction in the jugular foramen and the petroclival region were found during operation. The metastasis of ccRCC was confirmed by histological exam, revealing identical morphology and immunohistochemistry compared with primary renal tumor. Postoperatively, the patient had improvement in headache symptom but presented with palsy of the left abducent nerve. Cerebrospinal fluid otorrhagia occurred after operation, which was found and repaired in time. The patient proceeded to undergo radiation therapy. He died 4 months later after surgery due to multiple organ failure caused by aspiration.
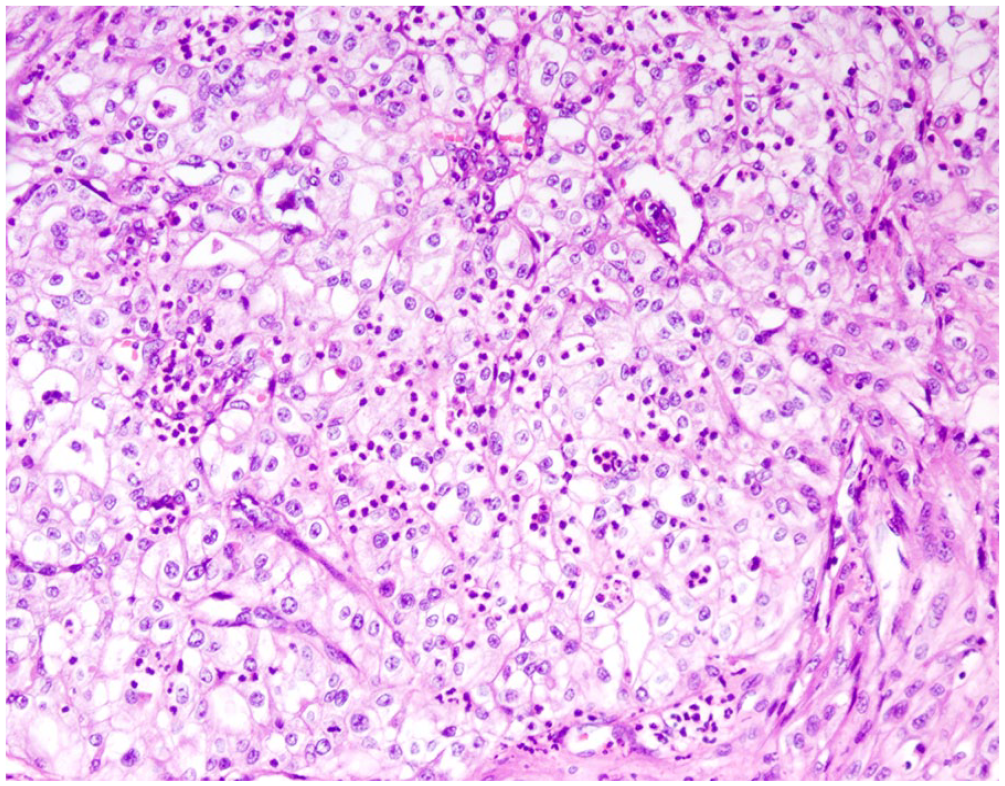
Renal cell carcinoma of right kidney. A histologic specimen showing large cells with clear, abundant cytoplasm and a dense vascular pattern. Hematoxylin-Eosin (HE) staining ×200.
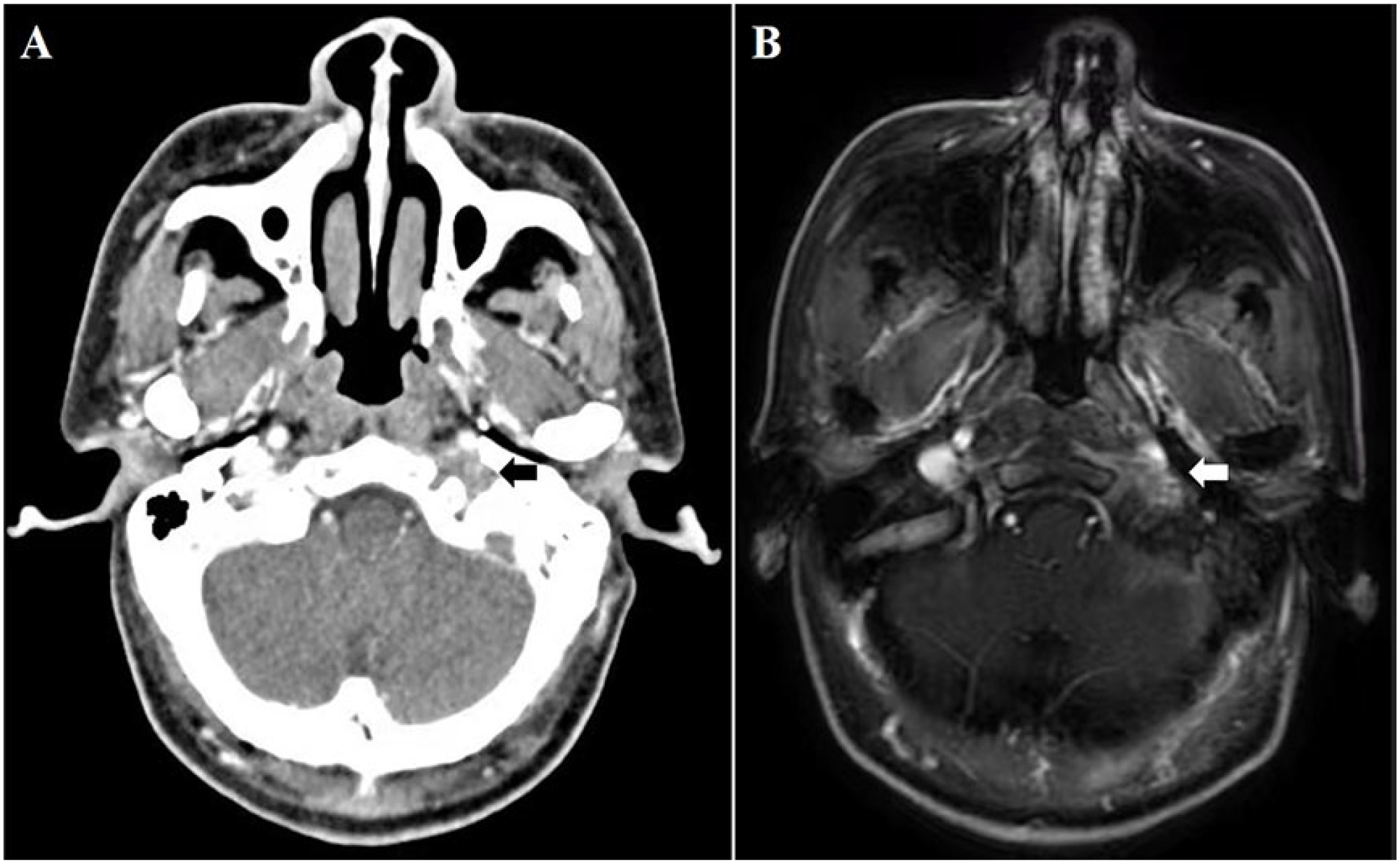
Contrast-enhanced axial CT (A) and MRI (B) showing space-occupying lesion at jugular foramen area and hypoglossal canal with mild enhancement.
Discussion
In this paper, we deal with the case of a patient with headache as the first clinical manifestation of ccRCC, following posterior cranial neuropathies related to metastasis to the skull base. The patient presented with headache symptom for over 1 year, during which time he was diagnosed with RCC and underwent right nephrectomy. However, the headache symptom had been attributed to cranial neuritis all the time until the surgical removal of a metastatic tumor in the petroclival region led to the diagnosis of metastatic ccRCC.
While distant metastases to the head and neck are rare, RCC is overall the third most common tumor to metastasize to this region, after lung and breast carcinomas. 8 A 2017 study reported that the presence of brain and liver metastases of RCC was associated with higher cancer-related mortality. 9 The time interval between nephrectomy and tumor metastasis is also related to prognosis, the shorter interval, the poorer prognosis. The median survival time of metastatic RCC was only 6 to 12 months, and the survival rate ranges between 10% and 20% at 2 years. 10 Distant metastasis after nephrectomy is associated with T stage and Fuhrman nuclear grade of the primary tumor.11,12 In this case, histopathologic examination demonstrated that the primary tumor is poorly differentiated and highly malignant. The nuclear grade is 4, which indicates a high possibility of metastasis.
Spread of cancer cells to the head and neck region is extremely complex and not fully understood up to now. CcRCC is rich in blood vessels because tumor cells can secret vascular endothelial growth factors, which facilitate angiogenesis. Besides, kidneys receive one-fourth of the circulating blood volume, and the petroclival region is abundant in blood supply, so we think the metastasis spread via the hematogenous system. There are 2 possible routes for RCC to metastasize to the petroclival region. The first includes the inferior vena cava, in which tumor cells can enter the basilar plexus through the inferior vena cava, the heart and the lungs, allowing emboli to seed structures and develop metastasis in the lungs. This theory suggests that RCC with head and neck metastasis already has disseminated lung metastasis, but it may not be seen on chest X-rays. The second involves the paravertebral venous plexus, in which tumor cells bypass the fine pulmonary filter bed. Emboli are shunted through the Batson plexus into the paravertebral venous plexus, which communicates superiorly with the intracranial plexus to reach the petroclival region. Therefore, tumor cells from the pelvis can also spread to other areas of head and neck, such as sinuses and thyroid, without passing through pulmonary circulation.13,14
Although rare, metastatic RCC should always be suspected in patients with symptoms suggestive of cranial nerve pathologies, especially with a history of primary RCC. It is important to remark that RCC is a malignancy with a high tendency for early metastasis and symptoms due to the metastatic lesion may be the only presenting complaint, such as headache and cranial nerve paralysis in this case. Radiological examination may not reveal metastatic lesions in the early stage; however, considering the location of the petroclival region, minimal metastases to this area can present with multiple symptoms. Since metastatic RCC may grow rapidly, cranial nerve neuropathies must be diagnosed with the possibility of metastatic RCC in mind. Even in the absence of radiological findings, patients should undergo systemic evaluation with contrast-enhanced MRI regularly. In this case, the patient was correctly diagnosed and treated after 1 year. The diagnostic delay occurred due to the protean nature and unusual manifestation of the tumor, as well as the overlook of presenting symptoms and the lack of follow-up contrast-enhanced brain MRI examination. MRI is necessary for assessing brain metastases since its better detection of small soft tissue lesions than CT. 15
Conclusion
The case described here highlights the importance of correct early-stage diagnosis of metastatic RCC. When a patient presents with cranial nerve neuropathies, the possibility of metastatic RCC should be sought. Brain metastases display nonspecific presentations, and it is useful to examine with MRI and CT scans radiologically. Correct diagnosis of metastatic RCC at an early stage is the basis of correct treatment.
Footnotes
Author Contributions
Y.T. contributed to drafting the article; P.Y. and L.Y. contributed to acquisition of data; H.J., Y.W., and L.S. contributed to clinical management; A.C. and F.Z. contributed to conception and design. All authors read and approved the final manuscript.
Data Availability
Data openly available in a public repository.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Natural Science Foundation of Shandong Province (Y.T., grant number ZR2022QH336); and the Traditional Chinese Medicine Science and Technology Project of Shandong Province (Y.W., grant number Z-2022067).
Ethical/Consent Statement
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional guidelines on human experimentation (Shandong Provincial ENT Hospital) and with the Helsinki Declaration of 1975, as revised in 2008. Written consent form was obtained from the patient involved in the study.