
Abstract
Keywords
Introduction
Primary thyroid lymphoma (PTL) first affects the thyroid gland and subsequently spreads to the lymph nodes and other organs. 1 PTL typically occurs in patients with Hashimoto thyroiditis.2-5 Common histological subtypes of PTL are extranodal marginal zone B-cell lymphoma of the mucosa-associated lymphoid tissue (MALT) and diffuse large B-cell lymphoma (DLBCL). 6 DLBCL is more aggressive than indolent MALT lymphoma or follicular lymphoma (FL).2,3,7 In patients with PTL, DLBCL is associated with an increased risk of mortality. 8
Ultrasonography (US) is the initial diagnostic modality used to detect PTL, followed by fine-needle aspiration cytology (FNAC). 2 US characteristics predictive of primary thyroid non-Hodgkin lymphoma include marked hypoechogenicity in the lesion and asymmetrical enlargement of the thyroid gland. 9 However, a few studies have mentioned the differentiation between DLBCL and other indolent lymphomas based on the US findings of PTL.
The most common symptom in patients with PTL is neck swelling, followed by pressure symptoms such as dyspnea, dysphonia, and hoarseness.3,10-12 In PTL, clinical symptoms include a rapidly enlarging neck mass (88%), dyspnea (65%), dysphagia (53%), and voice hoarseness (35%). 11 The progression of PTL can cause narrowing of the respiratory tract, including the trachea and larynx; therefore, early diagnosis and airway management are necessary for rapidly growing lymphomas. While reports have described subjective symptoms of respiratory distress, studies reporting evaluation of airway stenosis through imaging are lacking. In the present study, we investigated the differences between DLBCL and other indolent lymphomas and identified the factors predicting the possibility of DLBCL.
Materials and Methods
Medical records of 28 patients with PTL who underwent histological evaluation at our institution between 2005 and 2022 were retrospectively analyzed. As an initial step in the diagnosis of PTL, all patients underwent US, followed by FNAC. 2 In patients with cytologically suspected PTL and those with lesions showing increased lymphocytic infiltration, excisional biopsy was performed to determine the PTL subtype using immunohistochemistry. Patients who underwent treatment or experienced recurrence were excluded.
The recorded variables included sex, age, symptoms (pain and dysphagia), ultrasonographic findings, the presence of airway stenosis, blood test results, disease stage, and pathological diagnosis. Soluble interleukin-2 receptor (sIL-2R), serum C-reactive protein (CRP), and lactate dehydrogenase (LDH) levels were evaluated on blood examination.
We reviewed the recorded US images for each case to ensure an accurate evaluation. According to the classification of US findings proposed by Orita et al, 13 we classified the characteristics of US appearance as follows: linear strand pattern, a lesion with linear echogenic strands; and nodular pattern, a lesion with hypoechogenic lobulated segments (Figure 1). Airway stenosis was evaluated on the basis of computed tomography (CT) and laryngeal endoscopy (Figure 2).
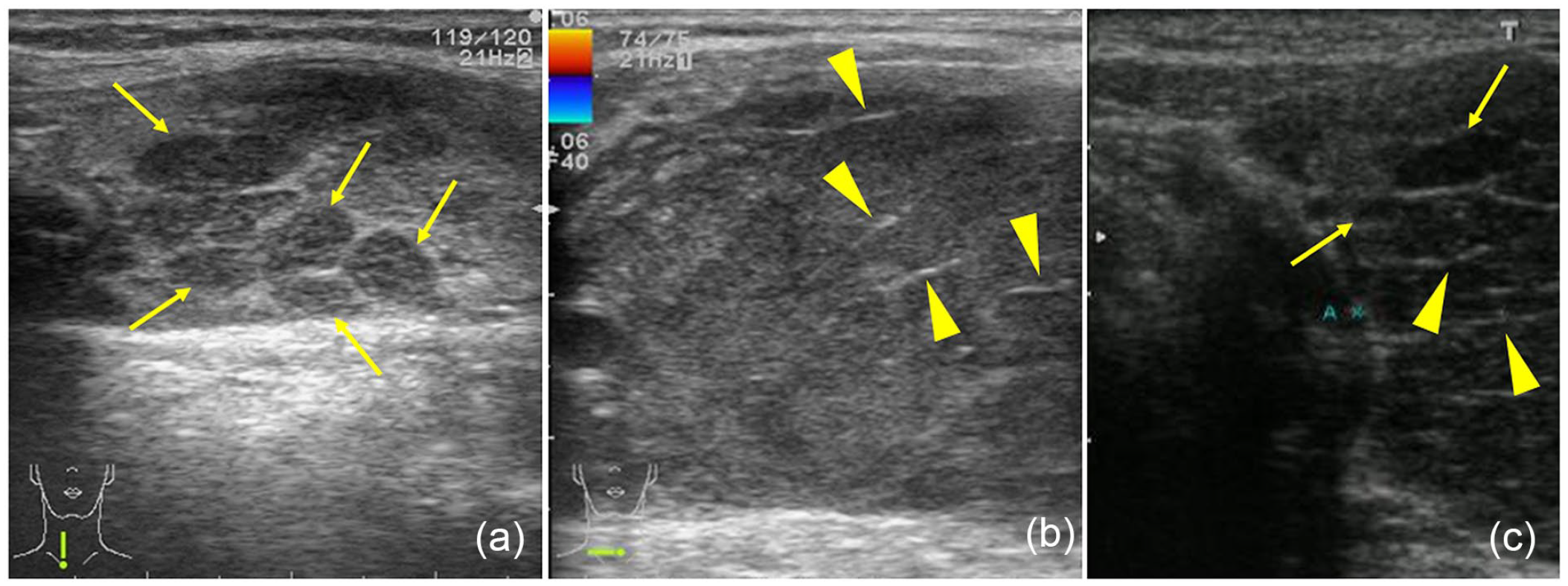
US characteristics of the representative cases. (a) A case showing the lobulated pattern in a lesion (arrows) with hypoechogenic lobulated segments. (b) A case showing the linear strand pattern (arrowheads) in a lesion, with the absence of the lobulated pattern. (c) A case showing both a linear strand (arrowheads) and a lobulated pattern (arrows) in a lesion. US, ultrasonography.
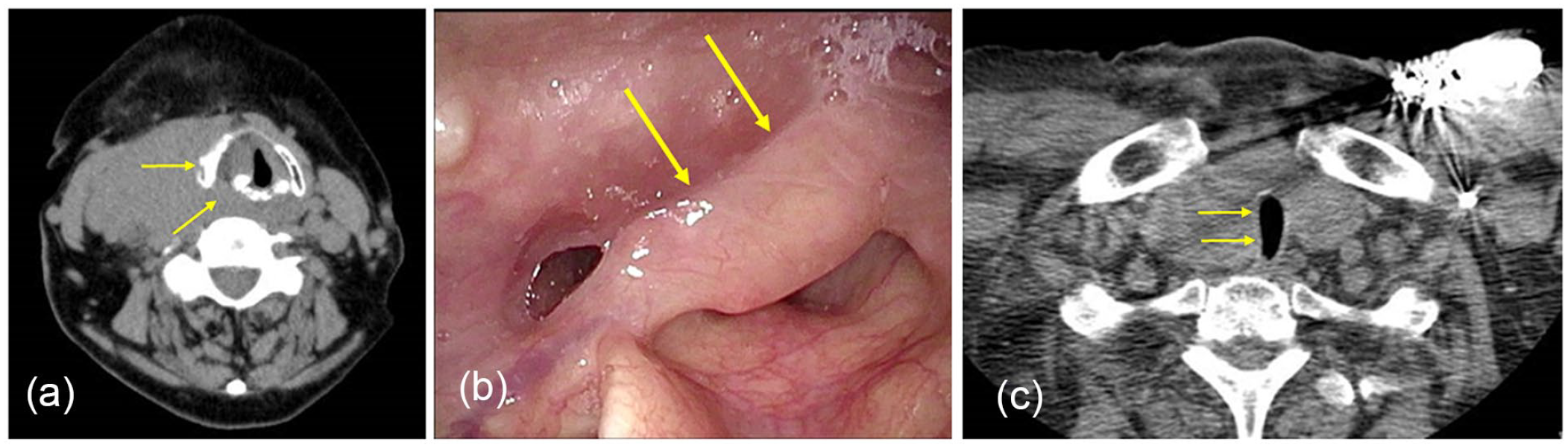
Endoscopic examination and CT findings of cases with airway stenosis. (a and b) In this case with diffuse large B-cell lymphoma, CT, and fiberscopic examination show laryngeal stenosis (arrows). (c) CT findings show tracheal stenosis caused by diffuse large B-cell lymphoma (arrows). CT, computed tomography.
The disease stage was determined according to the Ann Arbor classification system. The treatment was chosen at the discretion of the attending physician. The treatments administered to the 13 patients with DLBCL were as follows: rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) for 8 patients; pirarubicin, cyclophosphamide, vincristine, and prednisolone for 3 patients; and radiotherapy (RT) with total doses of 40 to 50 Gy for 2 patients. Treatments administered to the other 15 patients with indolent lymphoma were as follows: RT with total doses of 30 to 36.6 Gy for 6 patients; R-CHOP for 3; careful follow-up for 3; bendamustine and rituximab for 2; and surgery for 1 patient.
Statistical Analysis
Differences in baseline characteristics were assessed using Student’s t-test and Fisher’s exact test. Survival time was defined as the interval from the diagnosis of lymphoma to death or the last follow-up examination. Survival was estimated using the Kaplan-Meier method, and differences in survival between groups were assessed using the log-rank test. Patients were censored when they were lost to follow-up. All analyses were performed using the Bell Curve for Excel (SSRI, Tokyo, Japan). A P value < .05 was accepted as significant, while a P < .1 was considered to indicate a tendency.
All study protocols were approved by the Institutional Review Board of the Japanese Red Cross Society Himeji Hospital, Himeji city, Hyogo, Japan.
Results
Patient Characteristics and Overall Outcomes
The patient characteristics are summarized in Table 1. Overall, data from 28 patients including 11 men (39.3%) and 17 women (60.7%) with a mean age of 74.5 years (range, 47-96 years) were analyzed. Five (17.9%) patients had dysphagia and 4 (14.3%) complained of spontaneous pain. The FNAC results indicated PTL in 18 of the 28 patients (64.3%), while nonspecific lymphocytic infiltrates were observed in the remaining 10 cases (35.7%).
Demographic Characteristics of 28 Patients.
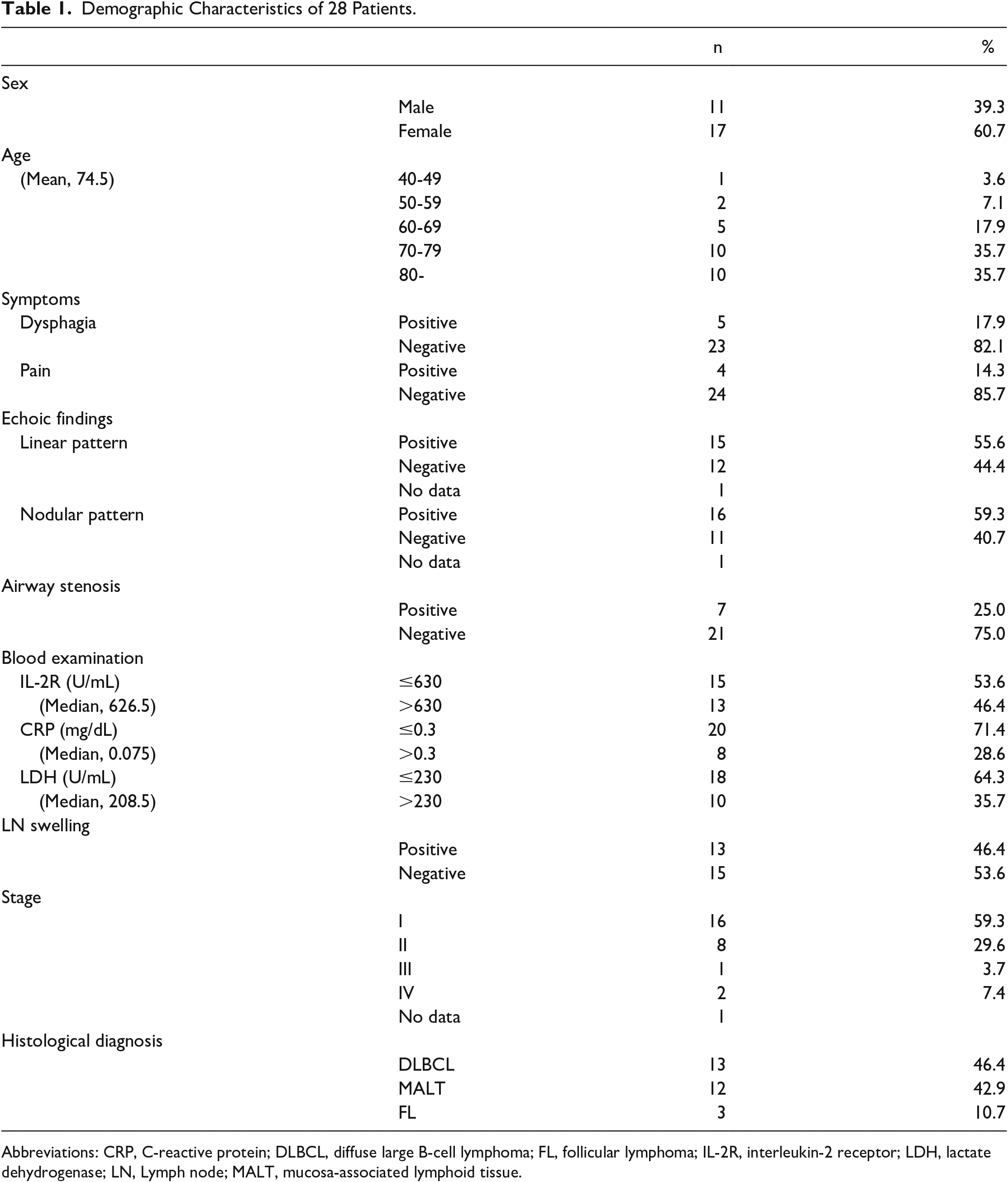
Abbreviations: CRP, C-reactive protein; DLBCL, diffuse large B-cell lymphoma; FL, follicular lymphoma; IL-2R, interleukin-2 receptor; LDH, lactate dehydrogenase; LN, Lymph node; MALT, mucosa-associated lymphoid tissue.
Of the 27 patients with US data, linear strand and nodular patterns were observed in 15 (55.6%) and 16 (59.3%) patients, respectively. Local or imaging findings revealed airway stenosis in 7 patients (25.0%). The median sIL-2R, serum CRP, and LDH levels at histological diagnosis of PTL were 626.5 U/mL (range, 226-7418 U/mL), 0.075 mg/dL (range, 0.00-19.43 mg/dL), and 208.5 U/mL (range, 150-505 U/mL), respectively. Lymphadenopathy was observed in 13 patients (46.4%).
In total, 13 patients received a histological diagnosis of DLBCL; 12, MALT lymphoma; and 3, FL. The FNAC results indicated the possibility of PTL in 11 of 13 patients with DLBCL (84.6%) and 7 of 15 patients with indolent lymphomas (46.7%), including MALT lymphoma and FL (P = .055). Cytological findings tended to be less suggestive of PTL in indolent lymphomas than in DLBCL.
Of the 27 patients except for 1 patient for whom case details were unknown, 16 (59.3%), 8 (29.6%), 1 (3.7%), and 2 (7.4%) patients had stage I, II, III, and IV, respectively. The 5-year disease-specific survival rates of patients with DLBCL and indolent lymphomas were 68.2 and 100%, respectively (Figure 3). Significant differences in the disease-specific survival rates were evident between the DLBCL and indolent lymphoma groups (P = .043). Of the 13 patients with DLBCL, 3 died of the primary disease.
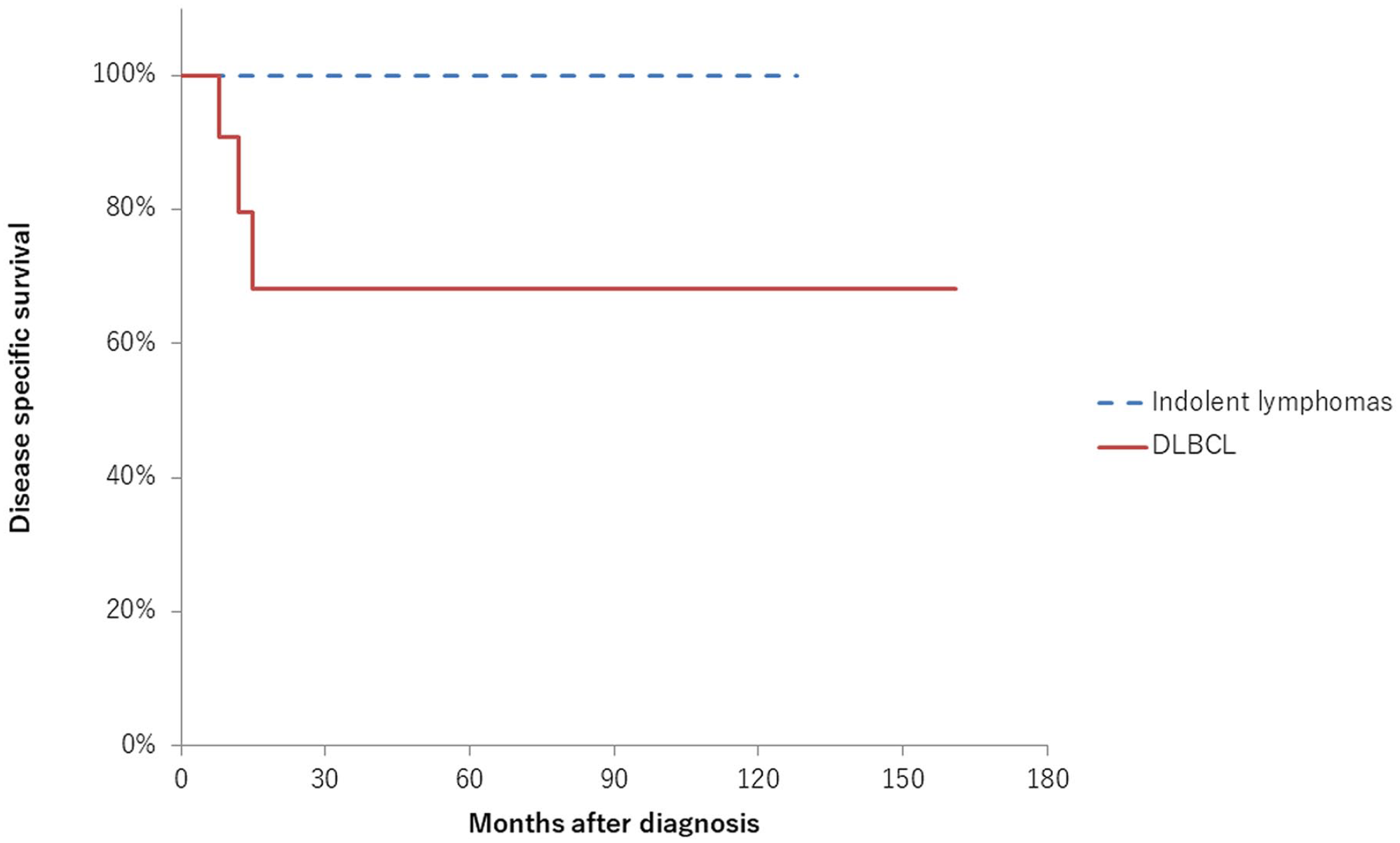
Disease-specific survival rate of patients with primary thyroid lymphoma. The 5-year disease-specific survival rates of patients with DLBCL and other indolent lymphomas were 68.2 and 100%, respectively (P = .043). DLBCL, diffuse large B-cell lymphoma.
Statistical Analysis of Factors That May Affect Predicting the Possibility of DLBCL
Results of the univariate analysis of factors predicting the possibility of DLBCL are shown in Table 2. Airway stenosis (P < .01), high LDH levels (>230 U/mL; P < .01), and linear echoic changes (P = .019) were significantly associated with DLBCL. By contrast, echoic nodular change was significantly lower in DLBCL (P < .01). Multivariate analyses showed that linear echoic strand pattern (P = .0497) and absence of an echoic nodular pattern (P = .012) were independent factors associated with the prediction of DLBCL (Table 3).
Univariate Analysis of Factors That May Affect Predicting the Possibility of DLBCL.
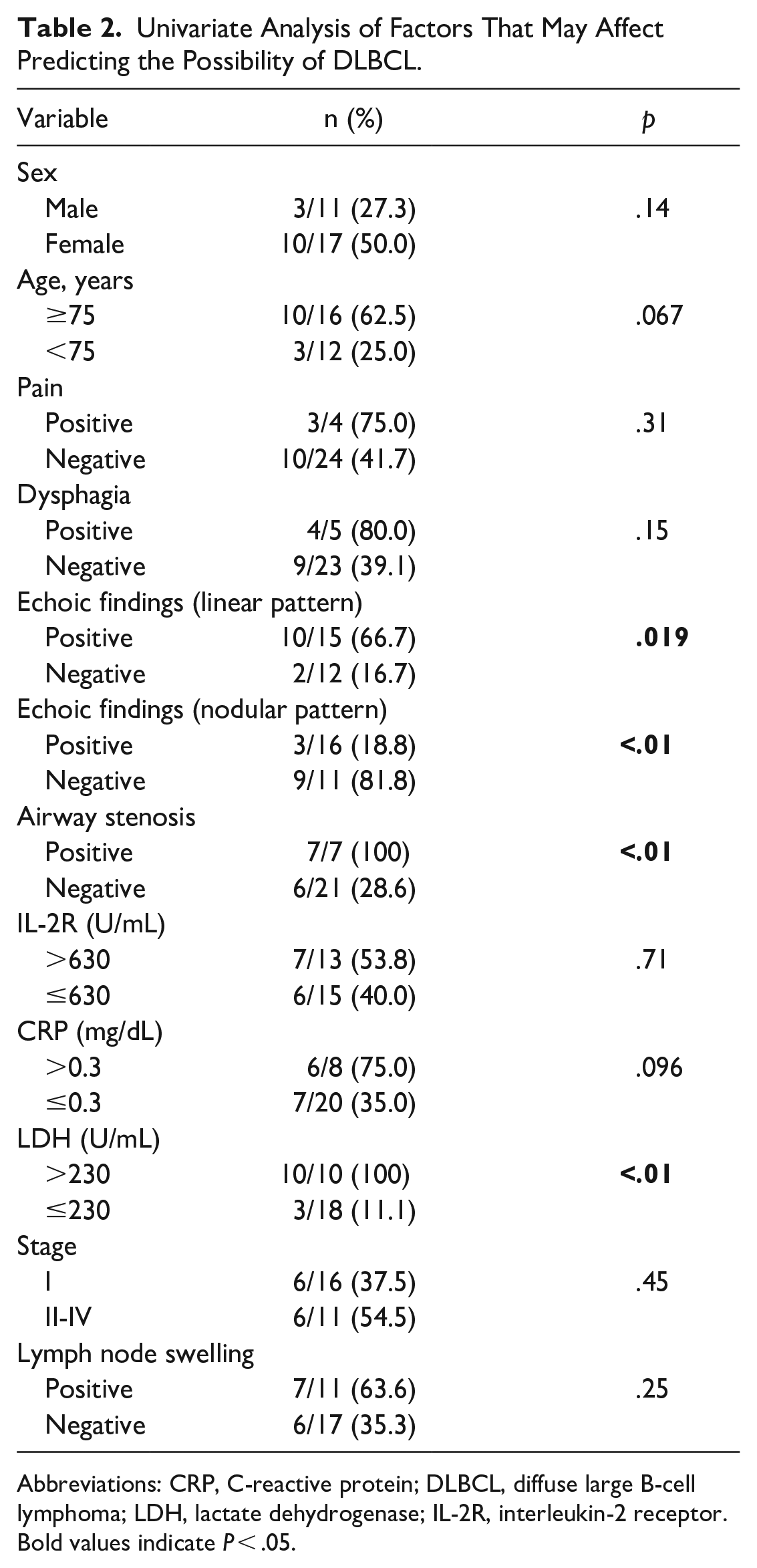
Abbreviations: CRP, C-reactive protein; DLBCL, diffuse large B-cell lymphoma; LDH, lactate dehydrogenase; IL-2R, interleukin-2 receptor.
Bold values indicate P < .05.
Multivariate Analysis of Factors That May Affect Predicting the Possibility of DLBCL.
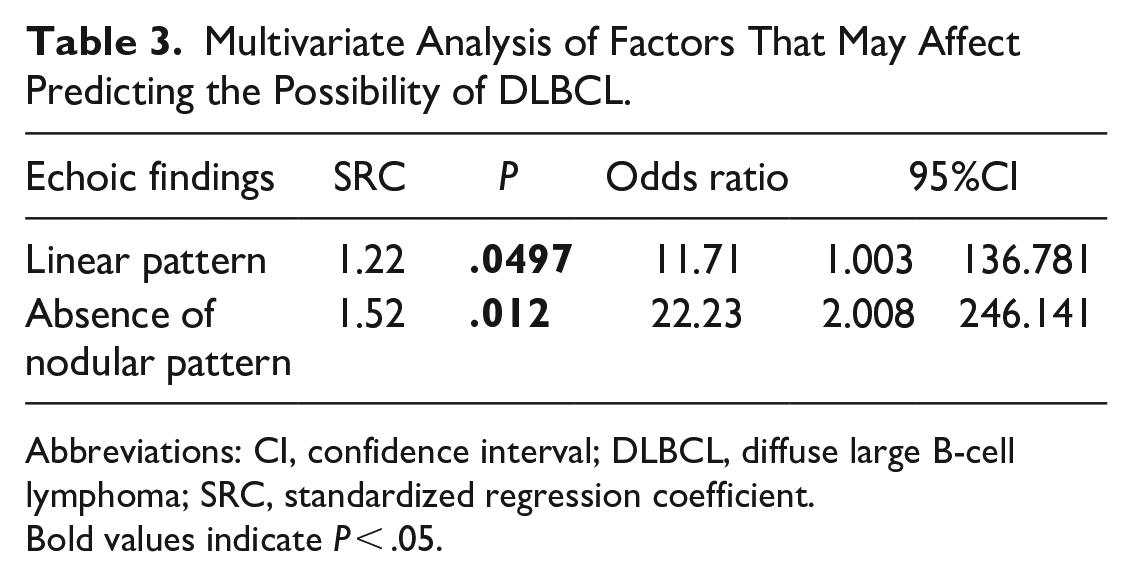
Abbreviations: CI, confidence interval; DLBCL, diffuse large B-cell lymphoma; SRC, standardized regression coefficient.
Bold values indicate P < .05.
Discussion
The present study showed that the survival rate of patients with DLBCL was significantly lower than that of patients with indolent lymphomas, including MALT lymphoma and FL; this is consistent with previous reports.6,14,15 Univariate analysis revealed a significantly higher frequency of airway stenosis in patients with DLBCL. In this study, airway stenosis was evaluated using CT and local findings, which facilitated a more objective evaluation of airway stenosis. Obstructive symptoms were more common in patients with DLBCL than in those with MALT lymphoma.4,14 However, previous studies evaluated airway stenosis using subjective rather than objective symptoms. Although it remains unclear whether airway narrowing noted on imaging and in local findings is specific to DLBCL might be one of the factors suggesting DLBCL.
In PTL, the materials obtained by core-needle biopsy are insufficient for ancillary histological studies, especially when thyroid lymphoma has low-grade histology, such as MALT lymphoma.2,4 DLBCL is easily distinguished by the presence of numerous large monotonous atypical cells, whereas MALT lymphoma is often difficult to differentiate from thyroiditis because of its heterogeneous appearance. 7 In the present study, indolent malignant lymphomas tended to have fewer cytologically suspicious findings than DLBCL. In indolent lymphomas with a good prognosis, it might be reasonable to perform a histological examination for cases with increased lymphocytes since distinguishing PTL from thyroiditis on cytology is difficult. By contrast, an early histological diagnosis is necessary when DLBCL with an aggressive clinical course is suspected, or when a differential diagnosis from anaplastic thyroid cancer with rapid growth is required.
In our study, DLBCL showed a high incidence of linear shadows and an absence of nodular patterns. The linear echoic strand pattern indicates fibrous bands in the specimens. 13 A typical US feature of PTL is the presence of linear echogenic strands.9,12 It has also been reported that the majority of MALT lymphomas show hypoechoic changes (74.7%), followed by single nodular (15.0%) and multiple patchy hypoechoic areas (7.5%). 16 Up to 40% of all DLBCLs appear to be transformed from MALT lymphomas. 17 Some nodular-type lymphomas may transform into other types. 5 In addition, the US appearance of the destructive pattern might suggest the transformation of MALT lymphoma into high-grade ML. 13 We speculated the appearance of the linear echoic strand pattern and the disappearance of the segmental pattern to indicate a transformation from indolent lymphomas to DLBCL.
In the present study, high LDH levels were only observed in patients with DLBCL. In several previous reports, LDH levels were higher in patients with DLBCL than in those with MALT lymphoma (56% vs 21%); however, none of these differences were significant. 4 In addition, elevated LDH levels have been reported in 26.2% of patients with MALT lymphomas and 41.4% of those with DLBCL,16,18 respectively. More cases need to be accumulated in the future to determine whether a high LDH level in PTL is suggestive of DLBCL.
The present study had some limitations. First, our institution encountered only 28 cases of PTL in 18 years owing to its rarity. Further studies with a larger number of cases are necessary for a more accurate analysis of the clinical features of PTL. Second, the treatments administered to patients included in this study were inconsistent. Chemotherapy followed by RT for high-grade lymphomas and radiotherapy alone for indolent lymphomas may be more effective treatment options. 15
In conclusion, among PTLs, DLBCL can cause airway stenosis. Linear echogenic strand pattern and the absence of nodular pattern should be recognized as factors predictive of DLBCL.
Footnotes
Acknowledgements
The authors are particularly grateful to all the people who have given us help with our article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
This study was approved by the ethics committee of the Japanese Red Cross Society Himeji Hospital, Himeji city, Hyogo, Japan.
Informed Consent
Because this is a retrospective study, the informed consent was not applicable.