
Abstract
Diffuse large B-cell lymphoma of the frontal sinus is a very rare malignant tumor with atypical clinical manifestations. It usually involves the orbital and ethmoid sinuses and causes vision loss, visual field damage, and nasal obstruction as the first symptoms. Herein, we report the diagnosis and treatment of a patient with diffuse large B-cell lymphoma of the frontal sinus, introduce imaging features of the disease, and discuss the differential diagnosis and treatment of the disease.
Introduction
Non-Hodgkin’s lymphoma (NHL) of the paranasal sinuses is a very rare malignant tumor. 1 Its incidence rate is approximately 3–5% of all malignant tumors, 2 1% of all cancers in the head and neck, 3 and 1.5–15% of all lymphomas.4-5 Diffuse large B-cell lymphoma (DLBCL) is the most common type of NHL of paranasal sinuses, accounting for approximately 66% of cases. It is rare for primary NHL to metastasize from the node to the sinus.3,5 Most cases of primary NHL occur in the maxillary or ethmoid sinuses and nasal cavity, 6 and primary cases in the frontal sinus are extremely rare, accounting for only 0.17–1.63% of all types of lymphomas. The clinical symptoms of DLBCL of the frontal sinus are often atypical. It generally invades orbital and ethmoid sinus tissues, causing related symptoms that can be easily misdiagnosed. Here, we report a case of DLBCL of the frontal sinus with orbital involvement as the first symptom.
Case Report
A 65-year-old man was admitted to our hospital for “the discovery of an upper right orbital mass and his right eye tearing for over a month.” One month prior, the patient had unintentionally palpated the upper subcutaneous mass in the right orbit. He found that the lesion was about the size of a soybean, soft, and without tenderness; however, it caused watering in the right eye. He did not seek treatment at this point. Later, the patient felt a progressive enlargement of the right orbital mass, with ptosis and a mild decline of vision in the right eye. Therefore, the patient visited our hospital seeking treatment.
Physical Examination
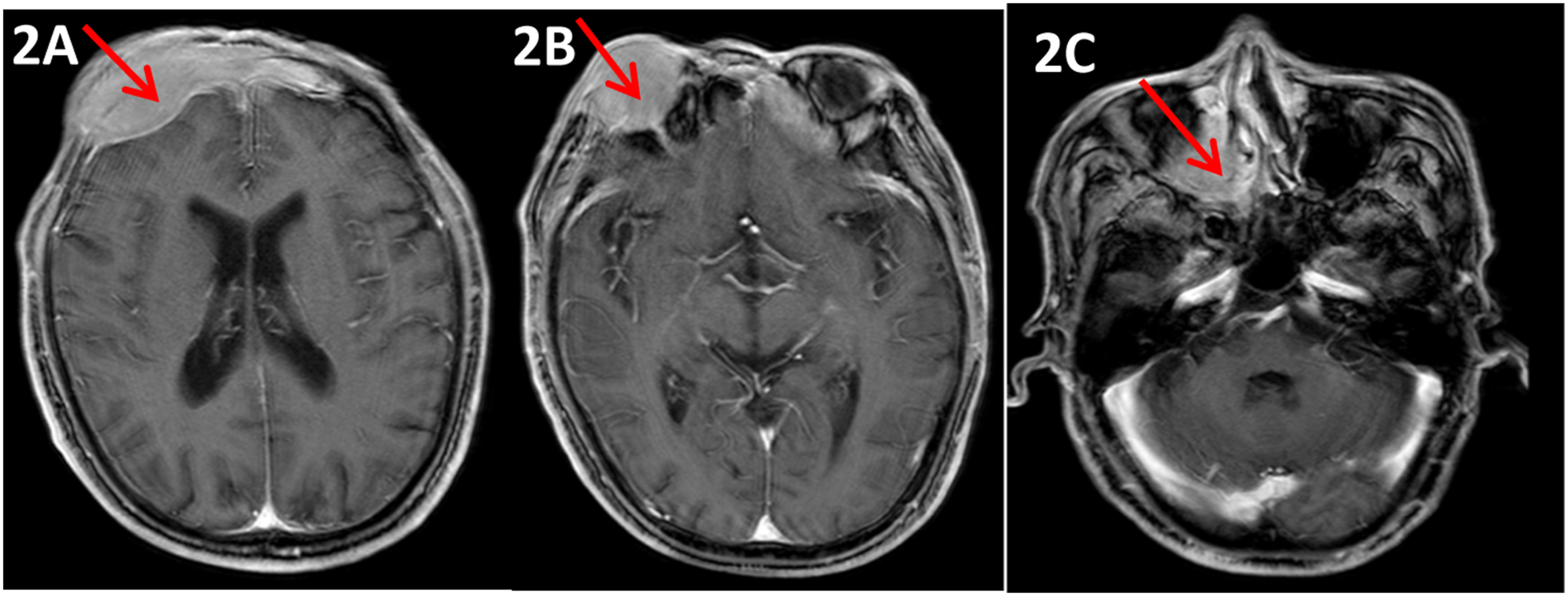
A 2 × 3 cm block was found in the upper part of the right orbit. It had regular morphology, soft texture, no tenderness, and an obvious demarcation from the surrounding tissue. It was not mobile, with no right orbital skin swelling. The right eye presented with ptosis, limited eye opening (Figure 1A), and a decrease in visual acuity, but no visual field or eye movement defects. The left eye had normal vision, visual field range, and movement abilities. Pupils were 3 mm in size and sensitive to light reflex. An orbital computed tomography (CT) scan showed a soft tissue shadow in the frontal, ethmoid, the bilateral, and maxillary sinuses of the right eye; therefore, neoplastic lesions were considered. Cranial enhanced magnetic resonance imaging (MRI) revealed (Figure 2) abnormal density images of the posterior nasal cavity, bilateral ethmoid sinus, right maxillary sinus, bilateral frontal sinus, and adjacent forehead, which provided further evidence for neoplastic lesions. In addition, an ultrasonic cardiogram revealed the patient had various heart-related issues: (i) a mildly enlarged right heart; (ii) a moderate tricuspid regurgitation, with moderate pulmonary hypertension; (iii) mild mitral regurgitation; and (iv) decreased left ventricular diastolic function. Other relevant auxiliary examinations did not reveal further obvious abnormalities. (A) shows the right superior orbital mass. (B) shows the right superior orbital mass disappearing In the posterior part of nasal cavity, bilateral ethmoid sinus, right maxillary sinus, bilateral frontal sinus, and adjacent frontal part (obvious on the right side), there are lamellar abnormal shadows; the lesions showed low signal intensity on T1W1, high signal intensity on T2W1 and T2-flair, and high signal intensity on Dwi.
During nasal endoscopy, the left middle nasal tract mass was swollen, with a soft and smooth surface, and there was swelling growth of the preserved soft mass, pressing on the skull base and orbit. Surgical removal of the anterior screen was performed, and the tissue was pathologically evaluated as “nasal sinus new organism” malignant tumor (Figure 3A); Immunohistochemistry (Figure 3B-3J): CK (-), CD20 (+), CD3 (-), CD5 (-), Ki-67 (+, 60%), S-100 (-), P-a x-5 (+), CD10 (-), bcl-6 (+), mum-1 (+), bcl-2, C-myc (-), C-m 30 (-), and EBER1 / 2 (-), supports large B-cell lymphoma. Combined with the examination, NHL was diagnosed, specifically DLBCL stage II group A IPI 2 points. Histological features of the patient’s tumor in most lesions. Hematoxylin and eosin staining (X40) was used to observe neoplastic cells with prominent nucleoli and partial cytoplasm (3A). Immunohistochemical staining (X400) showed CD20 positive (3B), Pax-5 positive (3C), bcl-6 positive (3D), bcl-2 weakly positive (3E), mum-1 positive (3F), Ki-67 positive (3G), CD3 negative (3H), CD5 negative (3I), and CD10 negative (3J).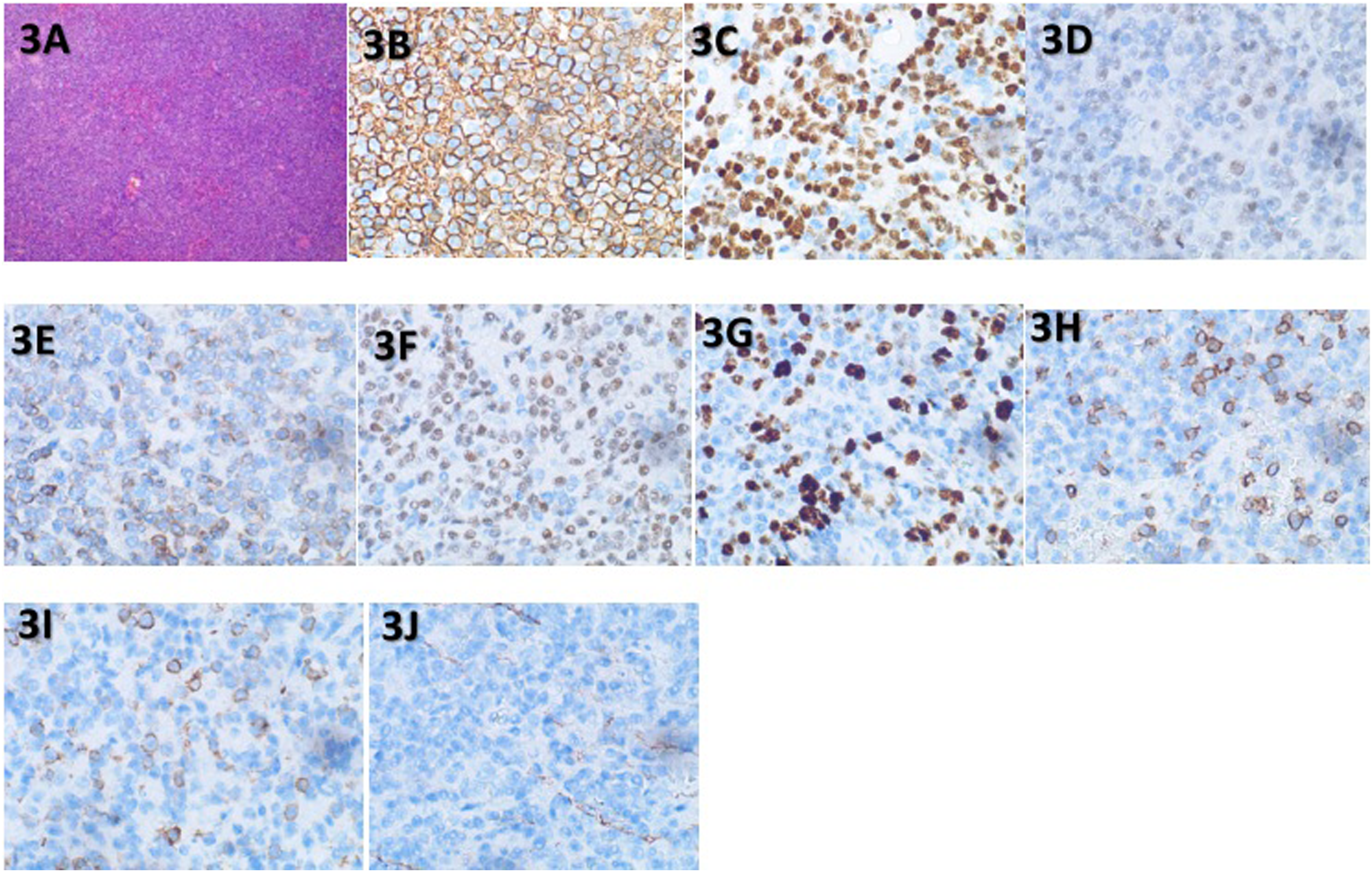
Treatment
Four cycles of postoperative chemotherapy with R-CHOP regimen (rituximab + epirubicin + vincristine + cyclophosphamide + prednisone) were administered on 7 October, 7 November, 2 December, and 23 December 2020. One month after chemotherapy, the patient was re-examined with an enhanced cranial MRI (January 2021) (Figure 4), in which the soft tissue mass around the frontal bone destruction area was found to have decreased in size. Physical examination confirmed that the upper orbital mass subsided, as well as right eye opening (Figure 1B), and the visual field returned to normal. Patchy bony destruction is seen in the frontal bone, mainly cumulating the right part of the frontal bone. Around the frontal bone is a mass of patchy abnormal signal, about 3.9 cm x 1.1 cm in size, with equal signal in T1W1 and slightly elevated signal in T2W1, the lesion involved the right frontal sinus cavity.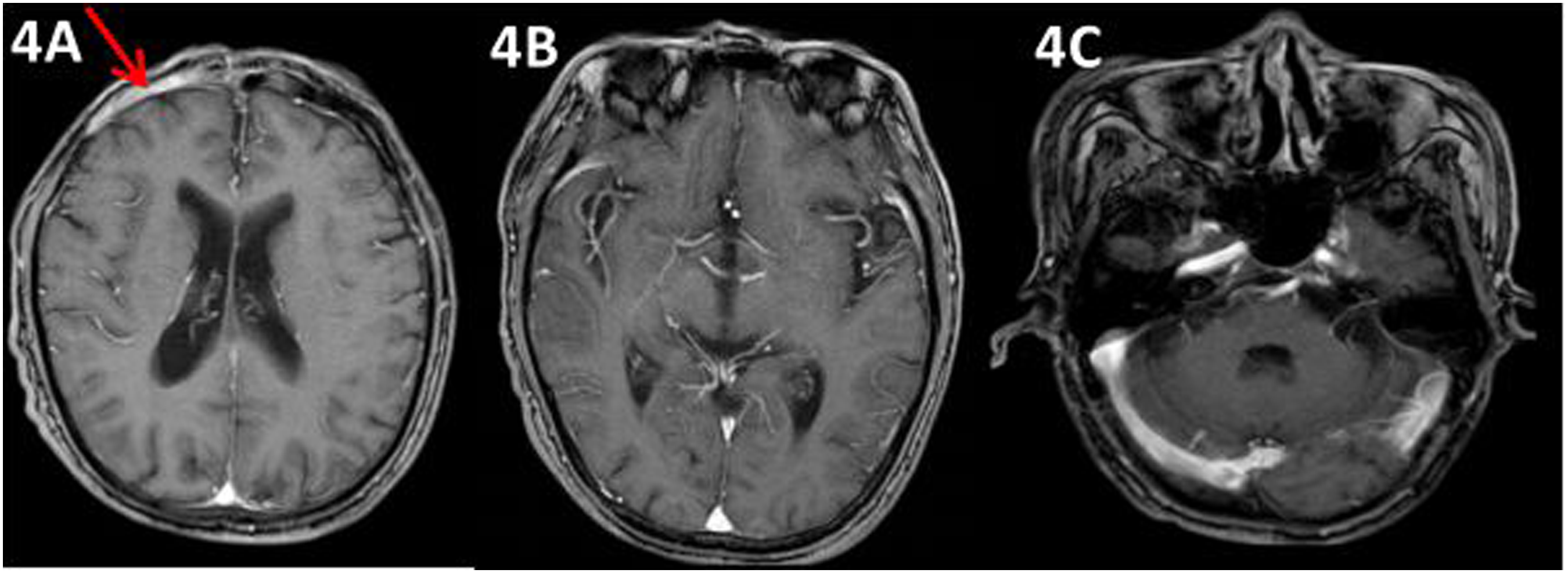
After a comprehensive evaluation of the patient including his physical condition, radiotherapy was started for the frontal sinus tumor lesions from February 2021. Using intensity-modulated radiation therapy (prescribed dose: P-GTV: 50GY/25Fx), radiotherapy was performed until 16 March 2021. An MRI scan after radiotherapy showed lesion reduction. R-CHOP chemotherapy was continued for two cycles on 24 April and 18 May 2021. In June 2021, 18F-fluorodeoxyglucose positron emission tomography (PET-CT) was performed (Figure 5), showing bone destruction of the frontal sinus, with no obvious abnormalities (Deauville five-point scale: 2 points). According to the results of the examination, the patient has reached complete response (CR). Six months after the end of treatment, the patient was re-examined by contrast-enhanced MRI and no significant abnormalities were noted. Frontal sinus bone destruction, mainly involving the right frontal bone, slightly increased glucose metabolism, adjacent to the frontal soft tissue thickening, considering the changes after treatment of lymphoma.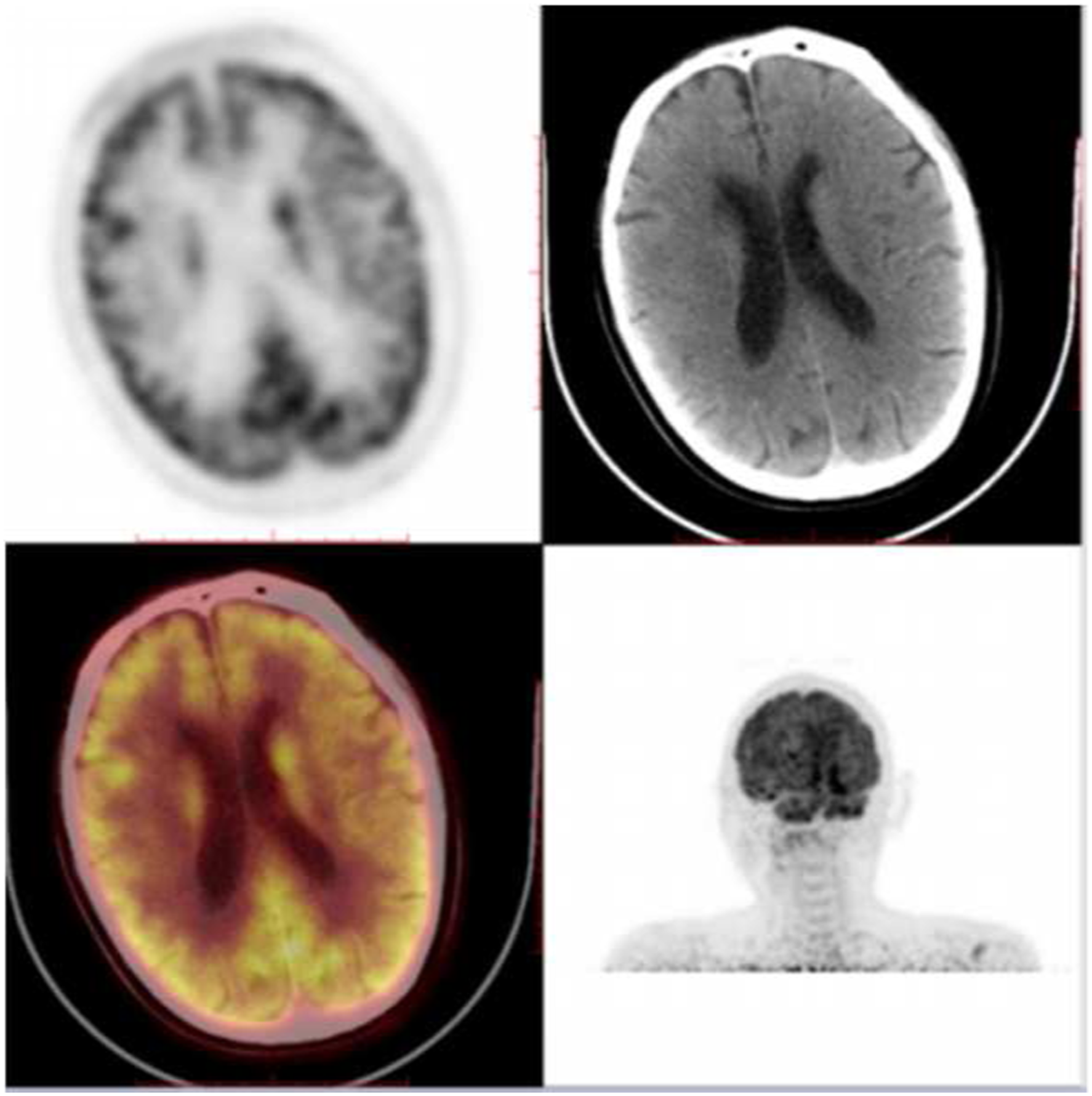
Discussion
Based on the tumor growth rate, NHL is classified as indolent and aggressive, with DLBCL being the most common histological subtype of aggressive NHL. 7 The head and neck are the most common sites of pathogenesis, with the neck and tonsil area being primary sites. The clinical manifestations of DLBCL are diverse, and the first-episode clinical symptoms are mainly associated with the tumor growth site.8-9 In cases of DLBCL in the nasal cavity, the main symptoms are nasal congestion and purulent nasal discharge. A lymphoma in the sinus has symptoms of facial swelling, numbness, and pain. Symptoms of a tumor in the tonsils and tongue include sore throat, pharyngeal foreign body sensation, and swallowing obstruction. The main symptom of a tumor growth in the neck is a painless neck mass. Pathological examination is the main basis for the diagnosis of NHL; in addition to the morphological characteristics and immunohistochemistry, flow cytometry, fluorescence in situ hybridization, and molecular detection are complementary methods important for the accurate classification of lymphoma.10-12 NHL is sensitive to chemotherapy, but the preferred treatment method of sinonasal fibrosis and schwannoma is surgical resection. The differentiation of sinonasal ossified fibroma, nasal and paranasal sinus schwannoma, and central extranodal lymphoma depends on pathological biopsy and imaging evidence. Therefore, special attention should be paid to discriminating between these pathologies during clinical work. 13
The onset age of sinonasal osteoblastic fibrosis ranges from 11 to 30 years of life; although it is a benign tumor, it is characterized by progressive growth and is clinically aggressive. The clinical symptoms of the disease are not clearly specific and have a late onset. 14 Pathology presents as well-defined fibrobone lesions and visible sandy material distributed in the fibrous matrix. 15 A CT scan shows a clear lesion margin, with the edge showing a low-density signal similar to the fibrous tissue. The interior of the lesion has a high-density signal similar to calcifications, but the most important radiological marker is its clear edge. 16 Nasal and paranasal sinus schwannomas mainly show solitary tumors with capsule, with clear borders and mostly unclear borders when malignant changes. 17 MRI is commonly characterized by solid and cystic regions of different phases of size.
In terms of treatment, anthracyclines have been proven to be the most effective drug for treating DLBCL. For older patients under 80 years of age, six to eight cycles of R-CHOP is the standard treatment regimen. 18 But Hershman et al. showed that any regimen of plorubicin increased the risk of congestive heart failure (CHF) by 29% in DLBCL patients, and their study was the first to confirm that hypertension is an independent factor that increases the cardiotoxicity of anthracycline. Therefore, in elderly patients and patients with hypertension or heart disease, ventricular function examination is recommended to dynamically evaluate the heart function of the patient pre-treatment. 19 Retrospective studies have confirmed that stage I and II patients of DLBCL in the head and neck can achieve CR with chemotherapy or radiotherapy alone, while advanced stage (stage III and IV) tumors generally achieve CR through chemotherapy combined with radiotherapy.20-22 Chemotherapy combined with radiotherapy can further eliminate the tumor lesions, improve the survival rate, and reduce the risk of tumor recurrence.23-24 In Boyle et al.’s and Kwak et al.’s studies, patients with early-stage DLBCL in the head and neck received sequential radiotherapy after chemotherapy. They reported that compared with chemotherapy alone, sequential radiotherapy after chemotherapy has significant clinical benefits. 25 However, Persky et al. reported that three cycles of R-CHOP treatment with sequential radiotherapy can clinically benefit DLBCL patients with high-risk factors or limitations periods older than 60 years.26-28 As an effective treatment measure of central nervous system lymphoma, radiotherapy after any stage of chemotherapy has shown to yield clinically significant results. 20
The prognosis of DLBCL in the head and neck is associated with the primary location, with the lowest 5-year overall survival with occurrence in the nasopharynx. The patient’s physical condition and treatment mode are also related to the prognosis. 29 By analyzing the clinicopathological characteristics and related factors of 94 DLBCL patients, Lin JY et al. concluded that patients with a high International Prognostic Index (IPI) score or high Eastern Cooperative Oncology Group (ECOG) score had poorer survival outcomes, where age was an independent risk factor affecting the prognosis of DLBCL.
After four cycles R-CHOP chemotherapy, the patient chose to not continue with chemotherapy and undergo radiotherapy for residual frontal sinus lesions because of older age, weaker constitution, and indication of cardiac insufficiency. At the end of radiotherapy, chemotherapy was performed according to the residual condition of the lesion. The treatment of sequential radiotherapy after chemotherapy not only reduces the risk of CHF, but also results in clinical benefits. Our patient achieved CR after treatment and is undergoing clinical follow-up.
In conclusion, primary DLBCL of the frontal sinus is very rare and prone to clinical misdiagnosis; therefore, clinicians should be careful when identifying DLBCL. Currently, the treatment of elderly patients with aggressive lymphoma and hypertension or cardiac disease remains challenging; however, treatment using three cycles of R-CHOP combined with radiotherapy may achieve satisfactory results.
Footnotes
Author Contributions
Lu Yang participated in the design of the study methods and wrote the main text, Xue Du was involved in the literature search and picture finishing, Yu Cui was involved in the literature search and picture finishing, and Bang-Xian Tan was involved in the guidance of the manuscript research methodology and the review of all the data. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.