
Abstract
Basal cell adenocarcinoma of the submandibular gland is an extremely rare carcinoma of the salivary gland that originates from the basal cells of the submandibular gland. Due to its rarity, there are relatively few case reports and literature on this cancer. After comprehensive clinical, imaging, and pathologic analyses, we confirmed the patient’s diagnosis and documented the consultation in detail. The purpose of this article is to report the case of a patient with basal cell adenocarcinoma of the submandibular gland and to perform a review of the relevant literature to improve the understanding of this rare disease.
Introduction
The 5th edition of the Classification of Head and Neck Tumors, published by the World Health Organization in 2022, states that basal cell adenocarcinoma (BCAC) is a relatively rare, low-grade malignant tumor that accounts for 1%-3% of all malignant salivary gland Tumors. It occurs predominantly in the parotid gland, while its occurrence in the submandibular gland is very rare. In addition, there are very limited case reports related to BCAC of submandibular gland worldwide.1 -4 BCAC of the submandibular gland has a low degree of malignancy, manifests as a painless gradual enlargement, is usually accompanied by nerve or vascular invasion, and is easily misdiagnosed as a benign tumor. However, based on the currently available literature, it is usually shown to have a relatively good prognosis.5 -7 In terms of growth pattern, this cancer can be categorized into four subtypes: solid, trabecular, tubular, and membranous, with the solid subtype being the most common. 8 According to available studies, the majority of patients are over 50 years of age, with a mean age of 60 years and an even gender distribution. 5 The main symptom is swelling, which may also be accompanied by pain, tenderness, or numbness of sensation in the face. 9 This case reports a case of basal cell adenocarcinoma of the submandibular gland, which is a progressively enlarging tumor that resulted in nerve damage and triggered sensory abnormalities of the face and neck.
Case Reports
History and Clinical Information
A 56-year-old woman was admitted to the hospital with a 2 month history of a right neck mass with progressive enlargement. The right neck mass was found 2 months ago for no apparent reason, and was about the size of a walnut, medium in texture, with no redness, swelling, or ulceration of the surface skin, no compression pain, poor mobility, normal facial sensation, and no symptoms of fever, tinnitus, hearing loss, retractable bloody mucus, nasal congestion, runny nose, rhinorrhea, hoarseness, or tightness in the chest, shortness of breath, dyspnea, or dysphagia. Fifteen days before her presentation to our hospital, she had a solid displacement of the right submandibular gland on ultrasound, but she did not receive any treatment. Now, the mass was found to be larger than before, measuring about 4.5 cm × 3.0 cm, with medium texture, poor mobility, and accompanied by numbness in the right side of the face and neck. To seek further treatment, she was admitted to the ENT clinic of our hospital with a request to investigate the nature of the right submandibular gland mass.
Physical examination: Good general condition, normal heart and lungs, liver and spleen not palpable under the ribs, and no major systemic diseases.
Specialist examination: A swelling of about 4.5 cm × 3.5 cm was detected in the right submandibular region, with medium texture, no redness, swelling or ulceration of the surface skin, no compression pain, poor mobility, and no obvious fluctuation sensation. There was no obvious abnormality in the nasal cavity and pharynx.
Imaging examination: Color ultrasound examination showed that the right submandibular gland was deeply connected with an unevenly echogenic mass, measuring about 4.7 cm × 3.0 cm, with uneven distribution of echoes within it, and spotty strong echoes and small anechoic distributions could be seen, and the margins were not glossy, and small lobes could be seen, with unclear borders. Color Doppler and spectral Doppler showed that slightly rich blood flow signal was seen in and around it. Consider a solid occupancy of the right submandibular gland and suggest further investigation. Computerized tomography (CT) scan of the neck showed that a mass-like slightly low-density shadow was seen in the right medial mandible, with blurred borders, measuring about 4.5 cm × 2.3 cm, with speckled calcified shadows, the lingual septum was shifted to the left by the compression, the right submandibular gland was not seen, and there were no enlarged lymph node shadows in the neck bilaterally (Figure 1). Consider medial occupation of the right mandible (nature to be determined); further examination is recommended.
Laboratory tests: blood, urine, and liver and kidney functions were essentially normal.
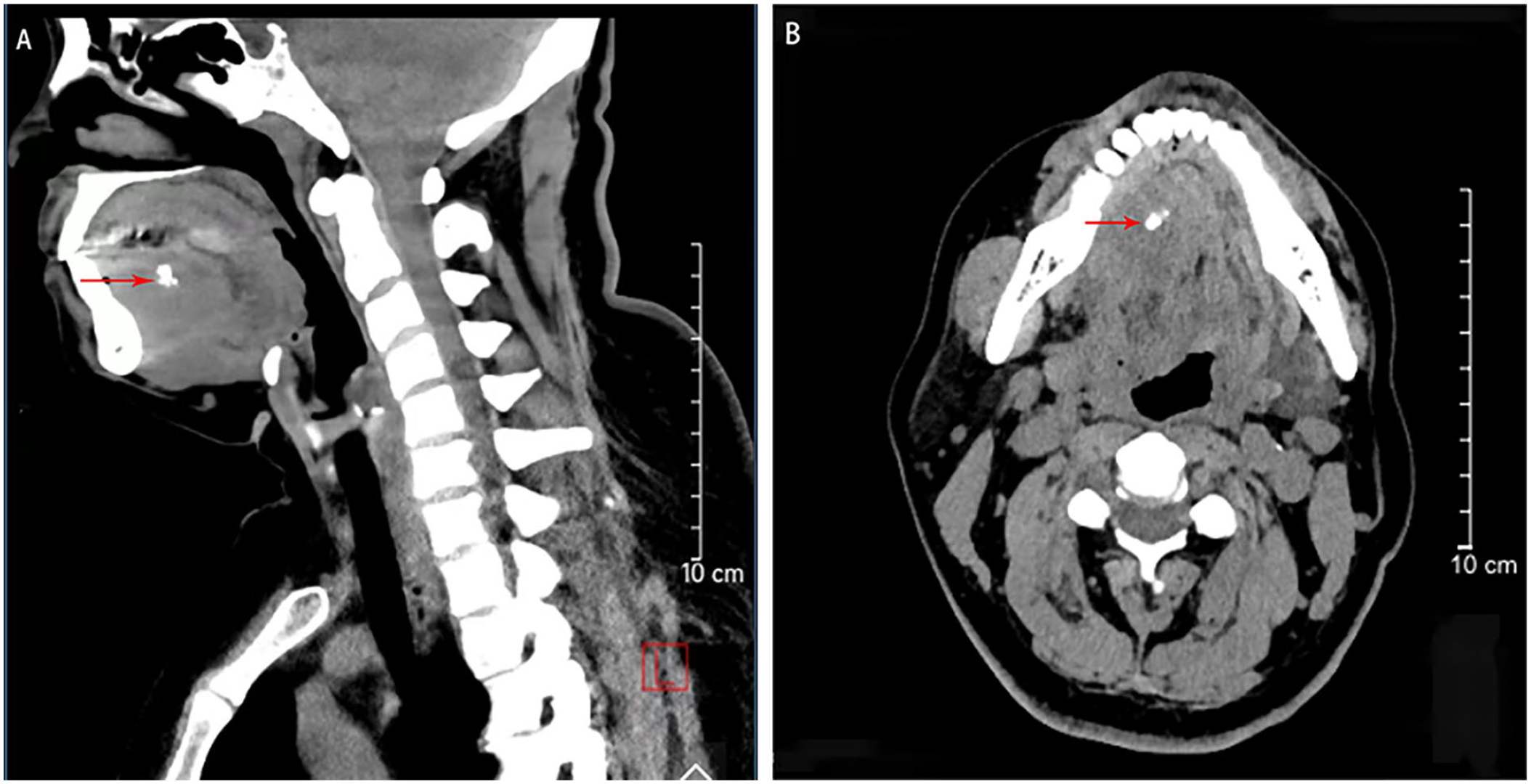
Preoperative CT sagittal (A) and coronal (B) views of the neck showing a mass in the right submandibular gland area, respectively (red arrows mark foci of high-density calcification within the tumor).
Treatment
After completing various examinations and excluding contraindications to surgery, the patient underwent “enlarged excision of right submandibular mass + reconstruction of the floor of the mouth + lymph node dissection of the neck region” under general anesthesia. Intraoperatively, an incision of about 8 cm in length was made along the lower edge of the right mandibular angle at 2.0 cm, parallel to the lower edge of the mandible. The skin and subcutaneous tissue were incised layer by layer, and the cervical vastus muscle flap was lifted to expose the swelling, which was seen to be hard and poorly movable, with severe adhesion to the suprahyoid muscles (mandibular hyoid muscle, chin bone hyoid muscle, and diastasis versicolor), and no obvious glandular tissues were seen. Protect the mandibular marginal branch of the facial nerve, along the mass in the superficial layer of the deep cervical fascia from the bottom upward blunt separation, ligation of the facial artery and facial vein, upward separation to the intramuscular muscle of the tongue, protection of the hypoglossal nerve, lingual nerve, in the diastematous muscle above the enlargement of excision and mass adhesion part of the suprahyoid muscle group, mass invasion to the right side of the intramuscular muscle of the tongue and the mucous membrane of the floor of the mouth, after the complete excision of the mass, and the vestibule of the oral cavity, and finally sweeping of the suprahyoid region (IA, IB area) lymphatic-fatty connective tissues. After the operation, the cavity was thoroughly rinsed with saline, the mucous membrane of the floor of the mouth was closed tightly and intermittently, and then the neck incision was closed layer by layer, the right neck was placed with a negative-pressure drainage bulb, the neck was bandaged, and a nasal feeding tube was inserted. The excised material was sent for pathological examination.
Postoperative Pathological Diagnosis
Pathologic examination report of our hospital: the submandibular gland mass was considered to be basal cell adenocarcinoma with necrosis (Figure 2); 8 lymph nodes were detected, all of which did not show cancer metastasis (0/8). Immunohistochemistry report: S-100 protein (S100), adenoepithelial (CK), smooth muscle actin (SMA), KIT (CD117), and the proliferative nuclear marker Ki-67 were all positive in the tumor cells. Conversely, Desmin, epithelial membrane antigen, estrogen receptor, and progesterone receptor were found to be negative in the tumor cells.
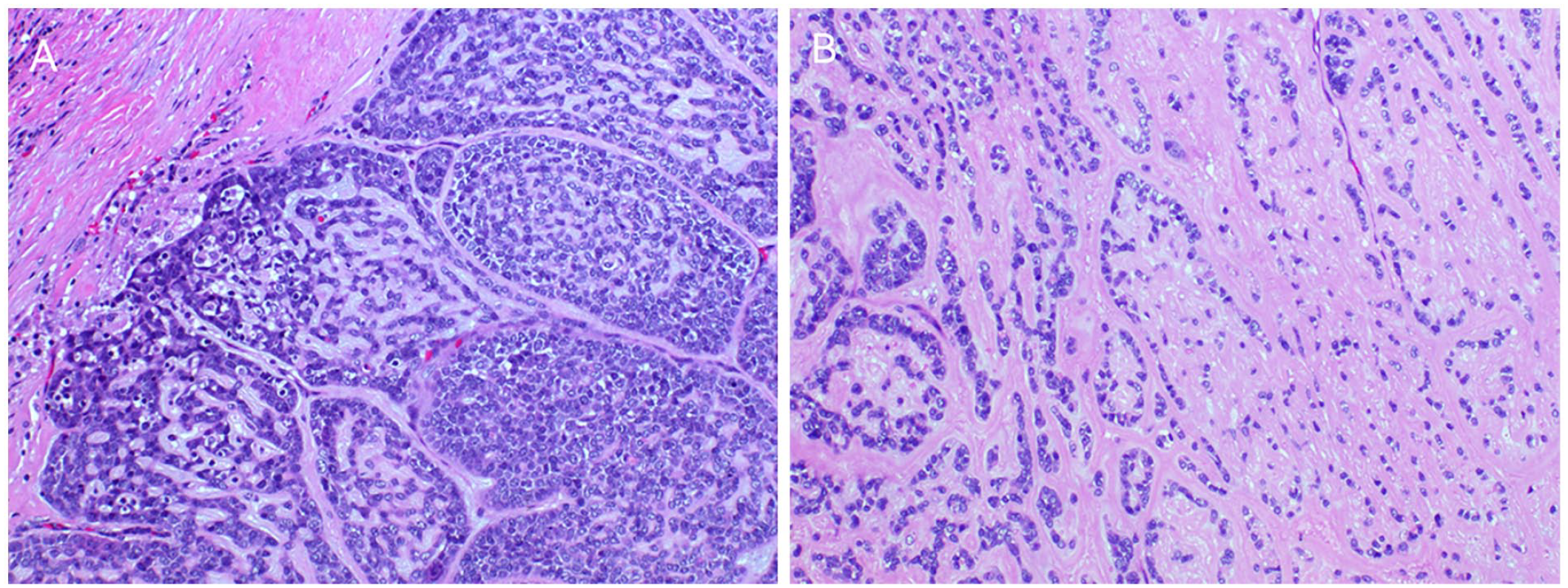
(A) Section shows that the nests of tumor cells are connected with each other in a strip-like fashion, with focal areas in a sieve-like shape, and light blue secretion can be seen in the lumen; (Haematoxylin & Eosin (H&E) Staining, ×10) (B) Section shows that the nests of tumor cells are made up of collagen fibers of varying thickness, small, darkly stained cells with little cytoplasm, some nuclei are slightly vacuolated, and small nucleoli are occasionally visible (Haematoxylin & Eosin (H&E) Staining ×40).
Postoperative Treatment
The postoperative period necessitates
Discussion
BCAC requires differential diagnosis from basal cell adenoma, adenoid cystic carcinoma, basal-like squamous cell carcinoma, and vesicular cell carcinoma. BCAC and basal cell adenoma have similar histological features and are distinguished by the presence or absence of peripheral nerve or vascular invasion. 3 BCAC can be distinguished from other diseases by its different histological features.10,11 The postoperative pathology report in this case showed that BCAC was considered and no lymph node metastasis was seen.The immunohistochemistry report indicated positivity for S100, CK, SMA, CD117, and Ki-67. Combined with relevant studies, the diagnosis can be clarified. BCAC of the submandibular gland is rare but has a promising therapeutic outlook. 2021 ASCO guidelines published in J Clin Oncol clarified the importance of complete surgical resection with the requirement that margins should be adequate, which has become the mainstay of treatment for BCAC. Surgeons should make every effort to completely remove the tumor during the first surgery to avoid recurrence.12,13 Due to the low rate of lymph node metastasis in BCAC of the submandibular gland, local lymph node dissection is usually not required. However, if clinical evidence of significant lymph node metastasis is found, cervical lymph node dissection may be considered. In non-early-stage patients, adjuvant chemotherapy may be required. Several reports in the literature suggest that radiation therapy following surgery 14 may improve local control and survival. 15 This case report emphasizes the importance of early diagnosis and comprehensive treatment in the management of this disease and provides general insight into the patient’s prognosis. Due to its rarity, further clinical studies and accumulation of literature are needed to improve understanding and treatment strategies for this rare cancer.
Results
The primary site of the tumor in this case was the submandibular gland, and BCAC of the submandibular gland is a rare salivary gland carcinoma with a low degree of malignancy, which can be easily misdiagnosed as a benign tumor. Comprehensive clinical and pathological evaluation is required to confirm the diagnosis and treatment. The successful cure of this case report helps to raise the level of awareness of the disease, leading to better management and treatment of similar patients.
Footnotes
Acknowledgements
The authors would like to thank for the contribution of Q.J.H., F.X.C., X.C., and Q.W.H. for their guidance and revision of the thesis, and for the great support through the hospital-conducted research.
Data Availability Statement
Data will be made available on request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
The study complies with ethical review, protects the rights and interests of research subjects, and adheres to ethical principles.
Informed Consent/Patient Consent
Informed consent has been obtained from patients and their personal information has been kept confidential.
Trial Registration Number/Date
2023-08-23
Grant Number
Not applicable.