
Abstract
Mouth floor cellulitis is a type of diffuse cellulitis involving the submandibular, submental, and sublingual spaces. This condition may cause asphyxia due to elevation and posterior deviation of the tissues of the floor of the mouth. The severity of submandibular gland infection often escalates in the presence of underlying comorbidities. Advanced age, hyperglycemia, and an immunocompromised status often lead to the rapid development of infection, resulting in complications such as acute upper airway obstruction. These complications increase treatment difficulty and the risk of mortality. We herein report a case involving an older adult with diabetes who developed mouth floor cellulitis secondary to a submandibular gland infection. Despite the severity of the submandibular gland infection, a timely, effective, and multidisciplinary approach improved the patient’s prognosis.
Keywords
Introduction
Mouth floor cellulitis, also known as multiple interstitial infections in the floor of the mouth, is a type of diffuse cellulitis that simultaneously occurs in the submandibular, sublingual, and submental spaces. 1 It is also known as Ludwig’s angina based on its first description by Wilhelm Frederick von Ludwig in 1836 as a potentially fatal, rapidly spreading soft tissue infection of the neck and floor of the mouth. 2 Mouth floor cellulitis can progress to life-threatening events, including acute upper airway obstruction, aspiration pneumonia, cervical necrotizing fasciitis, and mediastinal infection. Early diagnostics and adequate treatment procedures are important to ensure patient safety. Herein, we report a case of a life-threatening mouth floor cellulitis resulting from submandibular gland infection in a woman of advanced age with multiple underlying health conditions. The purpose of this report is to encourage clinicians to promptly identify the potentially life-threatening characteristics of mouth floor cellulitis, ensuring timely treatment.
Case report
The patient was a woman in her 90s with several underlying diseases, including diabetes, hypertension, atrial fibrillation, chronic heart failure, a bedridden state after fracture surgery, anxiety, and depression. She presented to our institution because she had experience a poor appetite for 1 week and throat pain for 1 day. She had been predominantly bedridden since undergoing lumbar vertebral fracture surgery 2 months previously and had recently experienced a poor appetite. Before admission, she began refusing to eat and take oral medications. The day before admission, she developed a sore throat accompanied by dry mouth and dysexpectoration. She had no other symptoms such as fever, runny nose, or nasal congestion. After nebulization and phlegm reduction, her symptoms were slightly relieved. The day after admission, she developed aggravated pharyngeal pain with increased sputum. The patient exhibited decreased oxygenation levels and required high-flow nasal cannula oxygen therapy, but she maintained stable hemodynamics. Physical examination revealed a body temperature of 37.5°C accompanied by tachypnea without the presence of the triple concave sign, cyanosis, or altered mental status. Neck examination revealed diffuse and tender swelling in the bilateral submandibular region. Blood tests demonstrated neutrophilic leukocytosis, an elevated high-sensitivity C-reactive protein level (147.81 mg/L), and a high interleukin-6 level (167.2 pg/mL). Ultrasound examination revealed diffuse lesions with suspected ductal dilation in the bilateral submandibular glands, possibly related to inflammation, as well as multiple hypoechoic lymph nodes around the bilateral submandibular glands (Figure 1). A computed tomography (CT) scan of the neck revealed swelling of the posterior pharynx wall accompanied by narrowing of the pharyngeal cavity and increased density of the bilateral submandibular glands (Figure 2(a) and (b)).
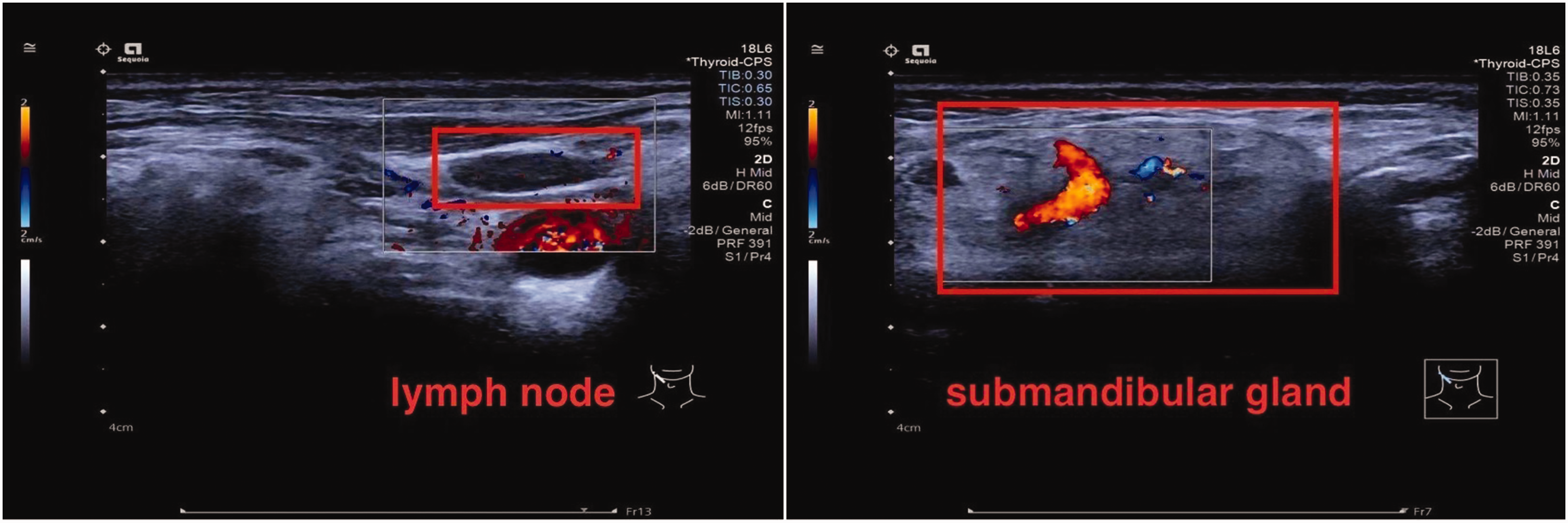
Color Doppler ultrasound of the submandibular gland and cervical lymph nodes after the second day of admission.
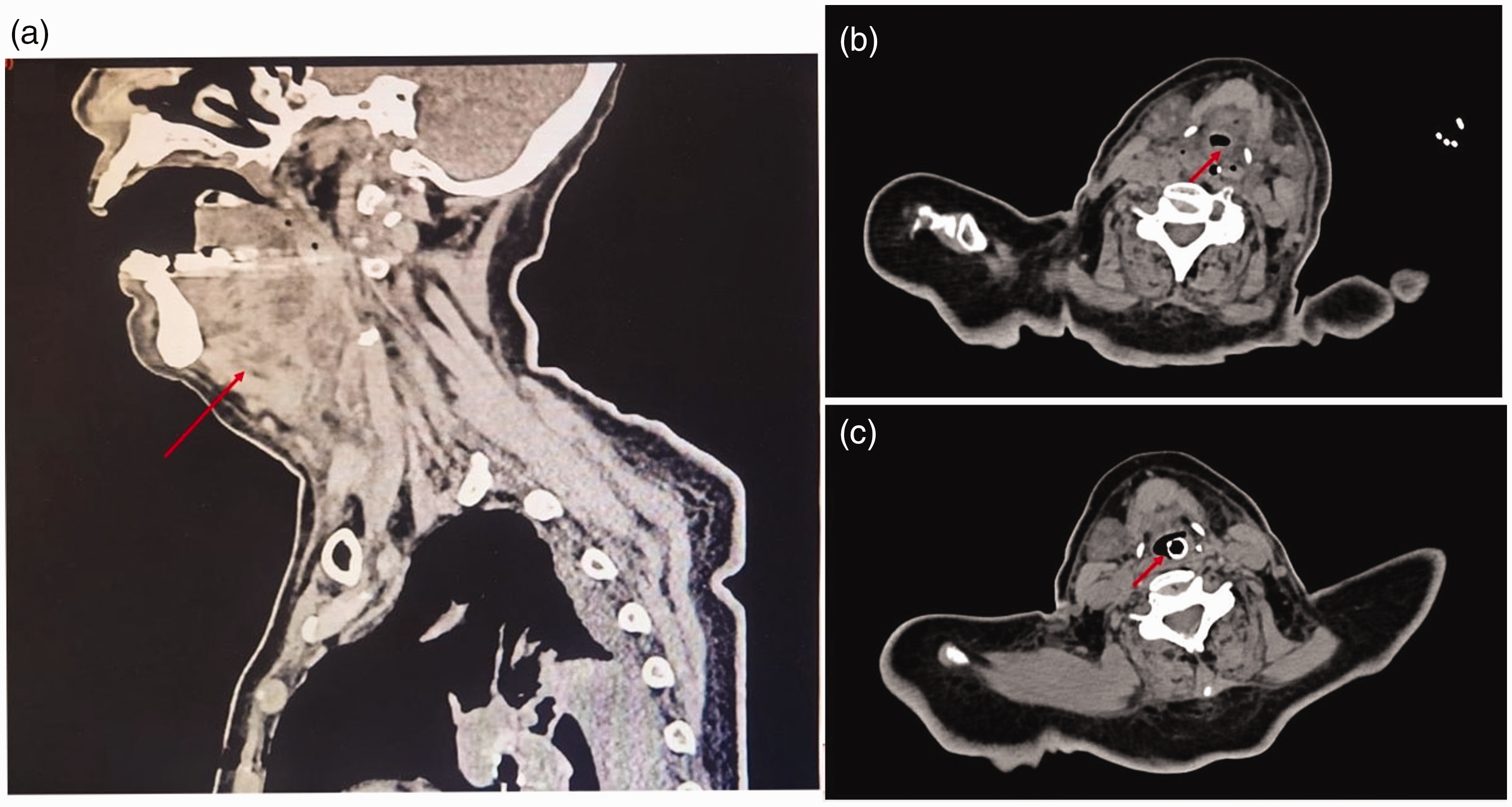
Computed tomography scan of the neck. (a) Sagittal view showing an increased anterior cervical soft tissue shadow before tracheal intubation. (b) Cross-sectional scan before tracheal intubation and (c) cross-sectional scan on the third day of tracheal intubation.
The patient was diagnosed with acute upper airway stenosis, mouth floor cellulitis, and bilateral submandibular gland inflammation after multidisciplinary consultations involving the otolaryngological department, stomatological department, anti-infective department, and ultrasound department. Given the high risk of airway obstruction, she was intubated and placed on positive-pressure ventilation after obtaining her daughter’s consent to treatment. She received intravenous ceftriaxone, omadacycline, dexamethasone, and gamma globulin for 3 days. She also underwent intensive oral care, irrigation of the bilateral submandibular ducts, and manual drainage of purulent fluid. Three days later, the swollen bilateral submandibular glands had significantly improved. A CT scan of the neck was repeated, which showed that the swelling of the posterior pharyngeal wall and bilateral submandibular glands had improved (Figure 2(c)). However, bronchoscopy revealed that the mucosa was still significantly and diffusely swollen with abundant purulent secretions (Figure 3(a)). Next-generation sequencing of a blood sample and culture of a purulent secretion were performed, and the results of both revealed Staphylococcus aureus sensitive to penicillin and tigecycline. The patient continued to receive intravenous antibiotics, intubation, and ventilator support. On the 11th day of admission, bronchoscopy showed that the swelling in the epiglottis was reduced, the glottic activity was good, and the vocal cords were not edematous (Figure 3(b)). Finally, she was successfully extubated and transferred from the intensive care unit to the general ward with continuation of the antibiotic therapy for several weeks. The reporting of this study conforms to the CARE guidelines. 3

Bronchoscopy examination. (a) On the third day of tracheal intubation, bronchoscopy examination revealed that the mucosa was significantly diffusely swollen and (b) on the 11th day of tracheal intubation, bronchoscopy examination showed that the swelling in the epiglottis was alleviated, the glottic activity was good, and the vocal cords were not edematous.
Discussion
Ludwig angina is a life-threatening cellulitis of the soft tissue involving the floor of the mouth and neck. Odontogenic infection is the most common cause of mouth floor cellulitis, followed by submandibular sialadenitis, lymphadenitis, and acute tonsillitis.4,5 Ludwig angina develops in previously healthy patients; however, some predisposing factors have been suggested, including diabetes, 6 oral malignancy, dental caries, poor oral hygiene, malnutrition, and an immunocompromised status. Our patient had multiple predisposing factors, including being bedridden, having diabetes mellitus, and having neurological disease, and the cause of her mouth floor cellulitis was submandibular sialadenitis. Submandibular gland inflammation refers to a retrograde infection of the submandibular gland caused by narrowing or blockage of the submandibular duct by salivary stones, foreign bodies in the duct, surgery, or scar contracture after injury. 7 The condition may rapidly progress, leading to edema of the airway structures (epiglottitis, vocal cords, and aryepiglottic folds) and potential airway obstruction. 4 Therefore, timely identification and intervention are crucial.
The diagnosis of mouth floor cellulitis relies mainly on clinical evaluation; imaging examinations do not play a direct role in the immediate assessment of the patient. 2 If the airway is secure, neck CT is helpful to assess the severity of the infection and identify abscesses. Our patient’s vital signs were stable, so a neck CT scan was promptly conducted. Some researchers have reported that the mortality rate in untreated cases is close to 100% because of acute sepsis or airway obstruction.1,8–10 Rapid airway management, antibiotic therapy, and aggressive surgical treatments can significantly decrease the risk of mortality. Our patient’s neck CT scan revealed significant narrowing of the upper airway, and preventive tracheal intubation was promptly implemented to secure the airway.
Most cases of mouth floor cellulitis are polymicrobial and involve Gram-positive, Gram-negative, and anaerobic microorganisms. Viridans streptococci and Staphylococcus aureus are the most commonly isolated organisms. Broad-spectrum intravenous antibiotics covering aerobic, anaerobic, and oral microflora are recommended. 10 In immunocompromised patients, the antibiotic coverage should include Gram-negative rods and beta-lactamase-producing aerobes and anaerobes. Furthermore, clinicians should consider methicillin-resistant Staphylococcus aureus (MRSA) coverage for patients at increased risk of MRSA or those with a history of MRSA infection. 2 Omadacycline is a novel aminomethylcycline antibiotic agent derived from minocycline that circumvents the efflux and ribosomal protection mechanisms of tetracycline resistance, restoring activity in vitro and in vivo against common community-acquired pathogens including staphylococci (e.g., methicillin-susceptible Staphylococcus aureus and MRSA), streptococci, Enterococcus species, and many Gram-negative bacilli.11,12 For our immunocompromised patient with diabetes, intravenous ceftriaxone was a viable option to provide coverage against Gram-negative rods and beta-lactamase-producing aerobes, and it was combined with omadacycline to cover both cocci and anaerobic bacteria.
The role of steroids in managing mouth floor cellulitis remains controversial. Some studies have suggested the limited utility of steroids, 13 while others have indicated that their use may reduce edema and cellulitis, ease intubation, and enhance the penetration of antibiotics. 4 As demonstrated in our case report, intravenous steroids were used as adjuvant treatment. Open surgical incision and drainage of the submandibular space should be considered to improve the airway status when an abscess is visible on imaging, fluctuance is present on examination, or antibiotic treatment has proven ineffective. Our advanced-age patient responded well to antibiotic therapy and catheter irrigation, and smooth drainage was maintained during her intensive care unit stay. She did not require surgical intervention.
Conclusion
We have presented a case of life-threatening mouth floor cellulitis in a patient of advanced age with multiple underlying diseases that improved with prophylactic tracheal intubation and antibiotic therapy. This case highlights the importance of early identification, diagnosis, and treatment through multidisciplinary collaboration.
Footnotes
Acknowledgements
The authors would like to express their gratitude to the staff of the Stomatological Department, Anti-infective Department, and Ultrasound Department for their valuable contributions to this case.
Author contributions
Jie Liu and Zhifang Fu contributed to the design of this case report. Jie Liu wrote the main manuscript text and prepared all figures. Dan Sun participated in the preparation of the figures. Zhifang Fu and Hongmei Jiao participated in the revision of the manuscript. Meilin Liu provided financial support. All authors read and approved the final manuscript.
Data availability statement
All data underlying the results are available as part of the article, and no additional source data are required. This patient details have been de-identified such that the identity of the patient may not be ascertained in any way.
Declaration of conflicting interests
The authors declare that they have no conflicts of interest.
Ethics
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of the Peking University First Hospital for publication (ethics approval number: 2024研21-001). The patient’s daughter provided written consent for treatment of the patient. The patient’s daughter also provided verbal consent for publication of this report.
Funding
This work was supported by the PKU-Baidu Fund (No. 2019BD019).