
Abstract
Plasmablastic lymphoma (PBL) is a rare and highly invasive type of non-Hodgkin’s lymphoma. It is usually associated with immunosuppression and human immunodeficiency virus infection. PBL most commonly occurs in the oral cavity, lymph nodes, and in other extranodal sites. However, it rarely originates from bilateral sinuses. Herein, we report the case of a 59-year-old man diagnosed with primary PBL of the sinuses confirmed by endoscopic biopsy, imaging materials, histopathological examination, and immunohistochemistry. The patient underwent 4 cycles of chemotherapy and 22 rounds of radiation therapy for 8 months. Re-examination by sinus computed tomography revealed no obvious tumor tissue in the nasal cavity and sinuses, suggesting that treatment was effective. No local recurrence or distant metastasis was detected at 6-month follow-up after the end of treatment.
Introduction
Plasmablastic lymphoma (PBL) is a rare, highly invasive, diffuse large B-cell lymphoma with high malignancy and a poor prognosis. PBL mostly occurs in people with low immune function, especially those infected with human immunodeficiency virus (HIV), accounting for 69% of cases. 1 This unique malignancy has been described most often in the oral cavity, lymph nodes, and other extranodal sites. It can also develop after living organ transplantation. 2 Only a few Epstein–Barr virus (EBV)-positive cases of primary PBL of the sinuses have been reported to date.
The clinical manifestations of PBL in the nasal cavity and sinuses are not specific and are often misdiagnosed (misdiagnosis rate: >20%). 3 When patients present with typical nasal symptoms, their specificity is poor; they may be confused with infection or inflammation cases. Local nasal medications, oral antibiotics, and other treatments may also increase patient mortality. 4 The pathological features of PBL lack the expression of B-cell-related antigens, which overlap with the features of lymphoma and myeloma with plasma cell morphology, increasing diagnostic difficulty. Histopathological examination is the gold standard for disease diagnosis. Early diagnosis and treatment can minimize the damage of the disease to patients, improve their quality of life, and prolong their survival time.
Case Report
A 59-year-old man presented with progressive right-sided nasal obstruction for 2 years, accompanied by hypoesthesia, intermittent headache, right eye swelling, and tears for 3 months. He had no history of HIV, organ transplantation, or systemic immune suppression. Physical examination showed swelling above the left eyebrow arch, with intact skin and hard palpation. Both eyelids were drooping, with right eye proptosis, conjunctival congestion, congestion of the lower lacrimal punctum, and tearing. The right eye had limited movement with diplopia. Electronic nasal endoscopy before treatment showed irregular tumor surface fester in the right nasal cavity, which was brittle and prone to bleeding upon touch, pushing the nasal septum to the left nasal cavity (Figure 1A and B). Enhanced computed tomography (CT) of the paranasal sinuses showed a soft tissue mass shadow in the right frontal sinus, ethmoid sinus, and nasal cavity, with an outward displacement of the medial wall of the maxillary sinus and compression of the right orbital wall. Soft tissue mass shadow could be seen in the left frontal sinus, with bone destruction in the anterior and basal walls, and some tumors breaking through the superior orbital wall into the orbit. No bone destruction or defect was found in the bilateral frontal sinus septum (Figure 2A–C).
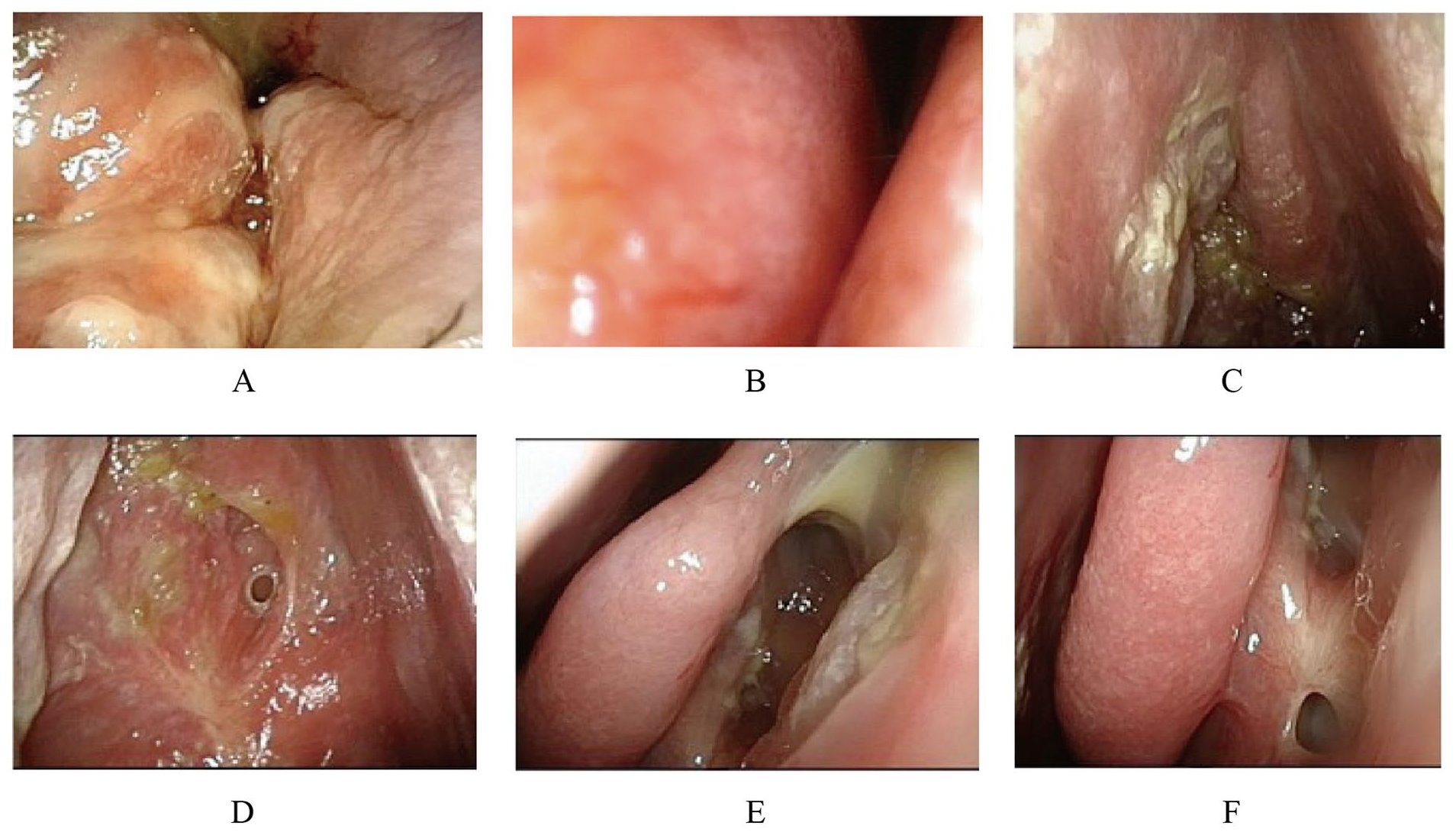
Electronic nasal endoscopy. (A) The right nasal cavity before treatment. (B) The left nasal cavity before treatment. (C-D) The right nasal cavity at the sixth month after the end of treatment. (E-F) The left nasal cavity at the sixth month after the end of treatment.
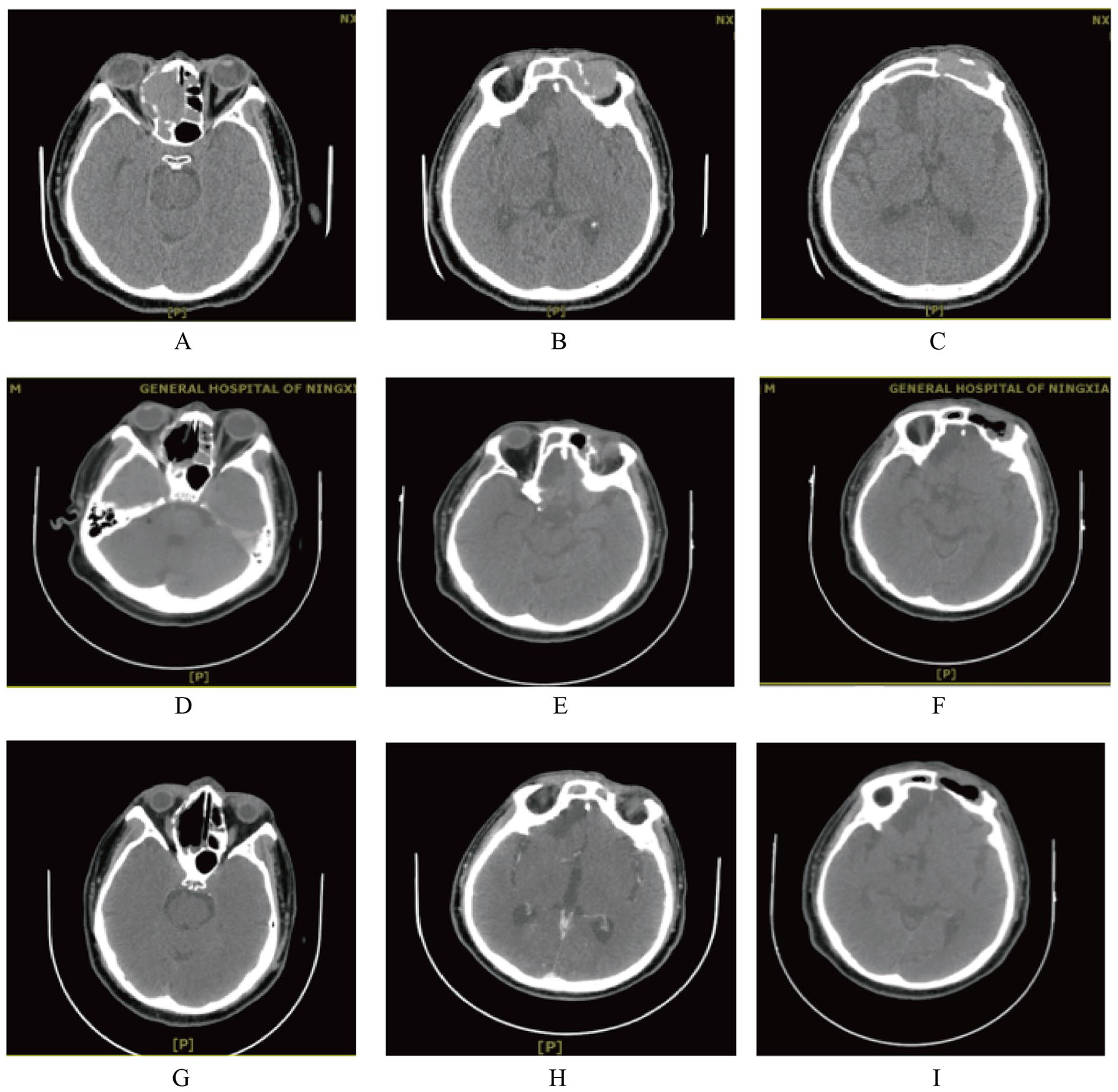
CT of the paranasal sinus. (A-C) Before treatment. (D-F) At the end of treatment. (G-I) The sixth month after the end of treatment. CT, computed tomography.
The patient underwent a nasal endoscopic biopsy. During this process, it was observed that the base of the right nasal tumor was suspected to originate from the top of the ethmoid sinus, with some protruding towards the frontal sinus and invading the nasal cavity downwards. The right middle turbinate was compressed and moved inward, and the right maxillary sinus was not invaded. The nasal septum mucosa was smooth. After contracting the left nasal mucosa, no tumor tissue was found in the middle nasal meatus. Therefore, a biopsy of the left sinus tumor was performed through an eyebrow arch incision. During the process, it was observed that the base of the left sinus tumor was located in the frontal sinus, with bone destruction in the anterior and basal walls. Some tumors protruded into the orbit, and the frontal sinus septum was intact. The pathological results showed diffuse infiltration of tumor cells with a “starry sky” phenomenon, misaligned nuclei, vacuolated, with a single prominent nucleolus or multiple peripheral nucleoli. The cytoplasm was basophilic with a perinuclear halo. The immunophenotype demonstrated strong positive expression of CD38 and CD138, confirming the plasma cell differentiation of the tumor cells, and CD79α (+), CD20 (−), EBER (+), G: Ki67 (about 90%), Mum-1 (+), and C-myc (90%, +), which are consistent with the immune phenotype of PBL (Figure 3). Bone scan showed no obvious abnormalities. There was no enlargement of the liver and spleen. No swollen lymph nodes were found throughout the body.
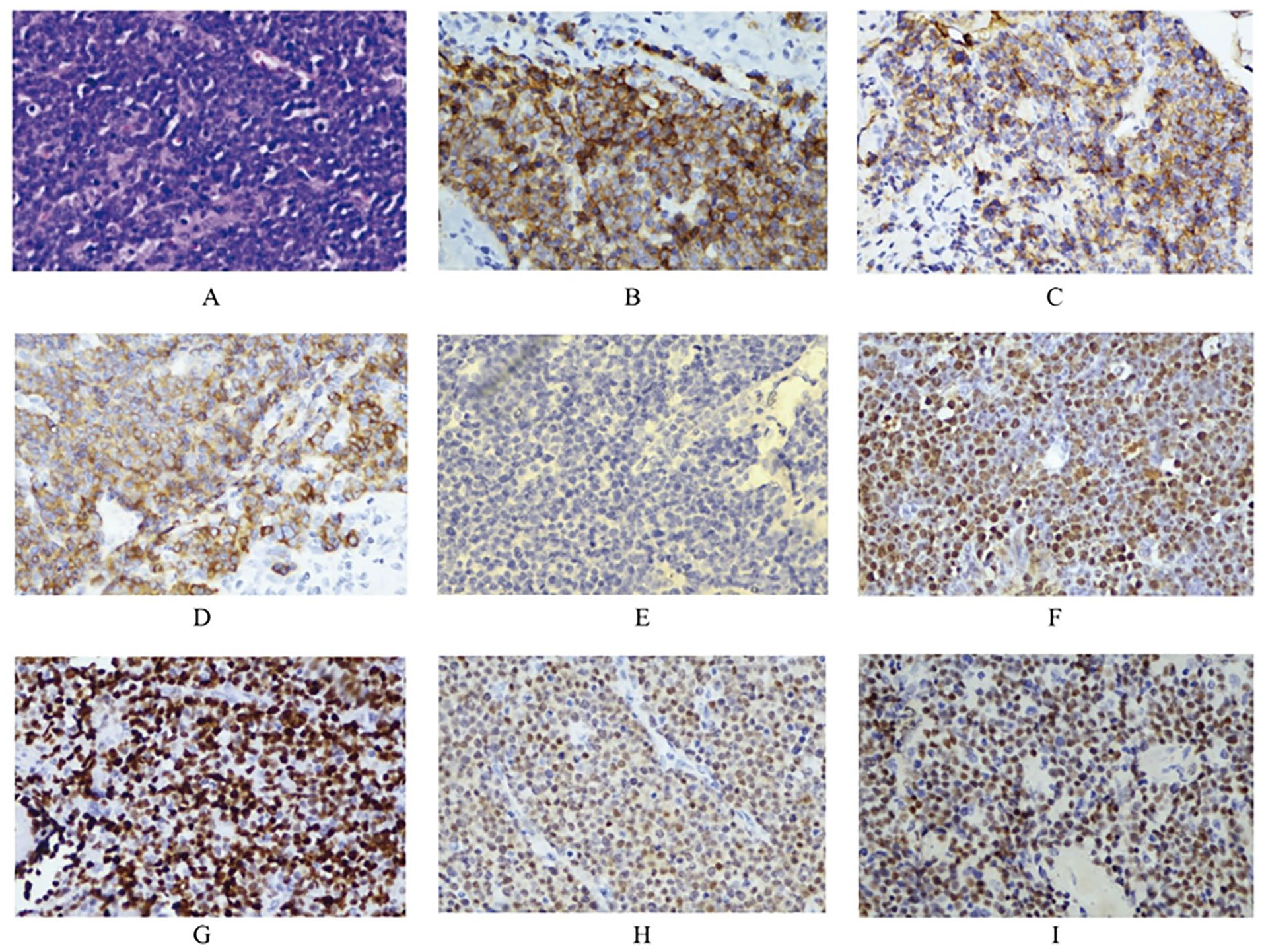
Postoperative immunohistochemical results showed that the immunophenotype was consistent with PBL. (A) Hematoxylin-eosin staining showed diffuse distribution of tumor cells. (B) CD38 (+), (C) CD138 (+), (D) CD79α (+), (E) CD20 (−), (F) EBER (+), (G) Ki67 (about 90%), (H) Mum-1 (+), (I) C-myc (90%, +). All images were observed under a 400× microscope. PBL, plasmablastic lymphoma.
No tumor tissue involvement was found in the bone marrow puncture. The CHOPE protocol (cyclophosphamide, 1.4 g on day 1; pirarubicin, 90 mg on day 1; vincristine, 2 mg on day 1; etoposide, 0.18 g on days 1–3; and dexamethasone acetate, 100 mg on days 1–5) was formulated for chemotherapy. The patient received 4 cycles of chemotherapy and 22 rounds of radiation therapy over a treatment period of 8 months. At the end of treatment, re-examination by sinus CT revealed no obvious tumor tissue in the nasal cavity and sinuses, suggesting that the treatment was effective. The diffuse soft tissue density in the nasal cavity and sinuses was considered to be related to mucosal swelling and inflammation (Figure 2D–F). At the sixth month after the end of treatment, electronic nasal endoscopy (Figure 1C–F) and nasal sinus CT (Figure 2G–I) showed no local recurrence or distant metastasis of the tumor. The patient was generally in good condition and did not complain of specific discomfort.
Discussion
The median age of onset of plasma cell lymphoma is 50 years, and most patients are men, which may be related to HIV and EBV infections. 5 The tumor cells are morphologically similar to B immunoblasts but have immunophenotypes of plasma cells. PBL is usually negative or only weakly positive for expression of CD20, while CD38 and CD138 are strongly positive. CD79α, a broad B-cell marker, is usually positively expressed. 6 In this case, the tumor’s cellular morphology and immunophenotypic characteristics were consistent with the pathological characteristics of PBL; the Ki-67 was 90%, indicating a high degree of malignancy and poor prognosis.
The patient's PBL originates from bilateral sinuses. Diagnosis of HIV/AIDS was negative, and the EBV test showed no obvious abnormality. However, Epstein–Barr early RNA in situ hybridization in tumor tissue cells was positive, histologically proving EBV infection. When the body is infected with the EBV, the virus lurks in memory B cells and persists by evading detection by the host immune system. Additionally, EBV infection may trigger carcinogenic mutations, inducing B-cell transformation and tumorigenesis.7 -9 HIV-positive patients have a higher risk of developing PBL and poor prognosis (median overall survival, <12 months). 7 Some reports showed that HIV-infected patients with PBL have better therapeutic effects with chemotherapy than HIV-negative patients with PBL. Antiretroviral therapy for HIV-related PBL promotes immune recovery.2,10,11 Primary plasma cell lymphoma of the sinuses with EBV infection has rarely been reported; whether this is related to disease prognosis remains unclear. The underlying mechanism is unclear, and further research is required.
For malignant tumors of the nasal cavity and sinuses, CT usually shows a soft tissue mass shadow in unilateral the nasal cavity and sinuses, with locally infiltrating growth, bone erosion, and sinus wall destruction. High-grade B-cell tumors can lead to orbital soft tissue and bone destruction. In contrast, perforation or destruction of the nasal septum is often associated with high-grade T-cell lesions. 12 Magnetic resonance imaging (MRI) has high diagnostic value for determining the nature of nasal and sinus tumors. For example, extranodal natural killer/T-cell lymphoma is mostly located in the nasal cavity with unclear edges, uneven signal intensity, internal necrosis, and significantly enhanced solid components on MRI. Diffuse large B-cell lymphoma is often located in the sinuses, with uniform MRI intensity, mild enhancement, and septal enhancement patterns, and can invade the intracranial or orbital regions. 13 However, the patient had previously undergone internal plate fixation for a right tibial fracture and could not undergo a cranial MRI. Meanwhile, the CT lacks specificity in the tumor diseases of the nasal cavity and paranasal sinus; therefore, the disease could not be accurately evaluated through imaging.
The extranodal sites of PBL were common in the oral mucosa and gingiva, followed by the digestive tract and skin, and the incidence was low in the nasal cavity and paranasal sinus. 14 Bilateral sinus primary PBL is even more rare.15,16 In this case, no bone destruction or defect was found in the frontal sinus septum and nasal septum assessed via imaging examination and nasal endoscopic biopsy. According to pathological examination and immunohistochemistry, bilateral sinus primary PBL was diagnosed. At present, the best treatment strategy for the disease is still unclear. Research shows that patients with the nasal cavity and paranasal sinus lymphoma are mainly treated with medical treatment, including chemotherapy, targeted therapy, and immunotherapy. Anthracycline-based chemotherapy combined with local radiotherapy can reduce recurrence and metastasis to a certain extent, thereby improving the overall survival of patients. It also has less side effects. 17 In this case, the patient received chemotherapy and radiation therapy. Despite the Ki-67% index being 90%, indicating a high degree of malignancy, the patient’s treatment response was positive. During the follow-up period, there was no local recurrence or distant metastasis. The patient was generally in good condition and did not complain of specific discomfort.
Conclusion
The overall survival rates of nasal sinus lymphoma at 2 and 5 years are 67 and 50%, respectively. Despite the progress in imaging, diagnosis, chemotherapy, and radiation therapy, disease progression and mortality rates remain high. 18 Primary plasma cell lymphoma of the sinus is an unusual lesion. Obtaining tumor specimens from the sinuses is challenging, increasing diagnostic difficulty. Additionally, the currently unclear treatment methods for primary PBL of the sinuses pose challenges in its management and treatment. Therefore, early diagnosis and appropriate treatment are crucial for preventing disease pro-gression and achieving optimal treatment outcomes. Considering the high malignancy of PBL in the paranasal sinuses, it is recommended that patients undergo close follow-up, with routine endoscopic nasal examination, and CT scan of the sinuses.
Footnotes
Author Contributions
Author’s Note Li Hou is the corresponding author, and she contributed to the conception of the study. Zhijuan Zhang and Zheng Ma are the co-first authors who contributed to writing this manuscript. Liping Zhang and Kaizhi Zheng ontributed to collecting images. All authors read and approved the final manuscript. Zhijuan Zhang and Zheng Ma contributed equally to this work.
Data Availability Statement
Data supporting the findings of this study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Ningxia Medical University [grant number XM20211041]; Natural Science Foundation of Ningxia Province [grant number 2019AAC03215]; and Science and Technology Department of Ningxia [grant number 2022BEG03105].
Ethical Approval
The research is approved by the Ethics Committee of the General Hospital of Ningxia Medical University (Ethics Number: KYLL-2023-0441). The patient has signed the informed consent form.