
Abstract
Cavernous hemangioma is a noncancerous vascular growth that arises from different parts of the head and neck region. However, parapharyngeal space contributes a very small percentage for its occurrence. We present a case of right parapharyngeal cavernous hemangioma, a very rare clinical presentation. This is a 57-year-old female presented with throat discomfort for 3 months. Examination finding showed a soft, diffuse, and non-pulsating mass over the right upper jugulodigastric region. A contrasted computed topographic scan revealed multiple calcifications in right parapharyngeal space. T2-weighted magnetic resonance imaging showed right parapharyngeal space mass with high signal and multiple phleboliths and dynamic angiogram unremarkable. Surgical resection done via transcervical approach and histopathological report revealed cavernous hemangioma with calcified thrombi. In conclusion, surgical intervention is the mainstay treatment and transcervical approach which is adopted in this case is the commonest approach used in surgical resection of cavernous hemangioma.
Introduction
Cavernous hemangioma is a nonmalignant vascular tumor. 1 The brain is the most common site for its occurrence. However, cavernous hemangioma has been reported to arise in the head and neck region despite being unconventional. 1 Although the incidence of cavernous hemangioma occurring in the head and neck is uncommon, it has been found to arise particularly in the oropharynx and larynx region. 1 However, to this date, parapharyngeal space has been an unusual site for cavernous hemangioma, with limited cases reported. 1 We report a case of a female presenting with a nonpulsatile mass from the right upper jugulodigastric region, with postsurgical removal histopathological diagnosis of cavernous hemangioma.
Case Report
A 57-year-old female presented with throat discomfort for 3 months. Physical examination revealed a soft, diffuse, and non-pulsating mass over the right upper jugulodigastric region. A contrasted computed topographic scan reported multiple calcifications in the right parapharyngeal space, possibly a malignancy (Figure 1). Magnetic resonance imaging (MRI) showed a right parapharyngeal space mass measuring 5.9 × 5.1 × 2.9, displacing the right submandibular gland anteriorly and right carotid posteriorly (Figure 2). The mass returns a high signal on a T2-weighted sequence with multiple phleboliths seen within. The dynamic angiogram showed no obvious tumor blushes or feeder vessels. The mass was entirely removed via a transcervical approach without complications (Table 1). The pathological analysis reported a cavernous hemangioma with calcified thrombi (Figure 3). She was well postoperatively. Repeated MRI scans showed no evidence of residual or recurrent (Table 1).
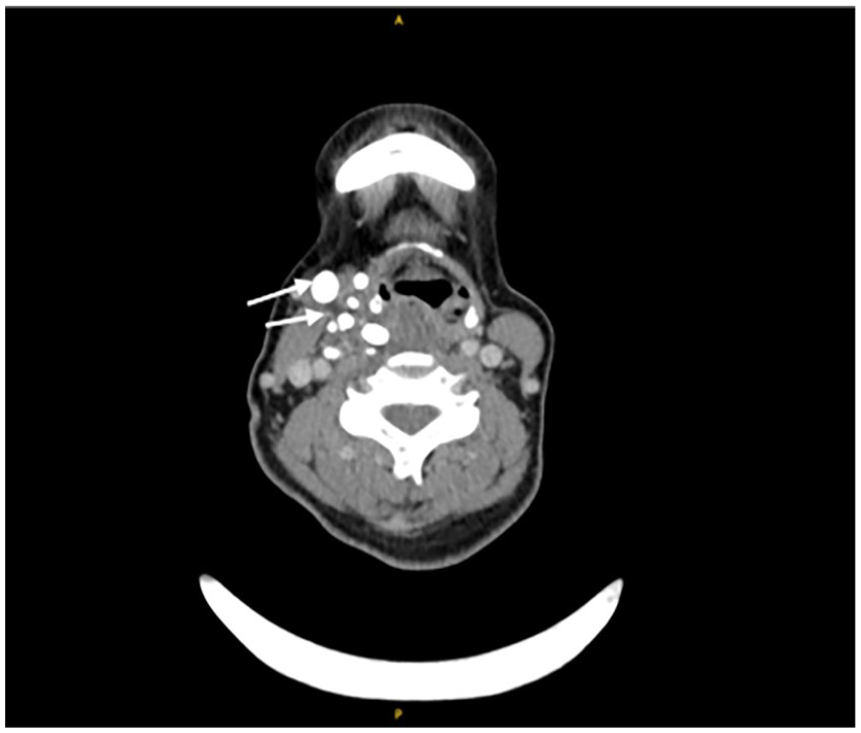
Multiple phleboliths (arrow) on the right parapharyngeal space.
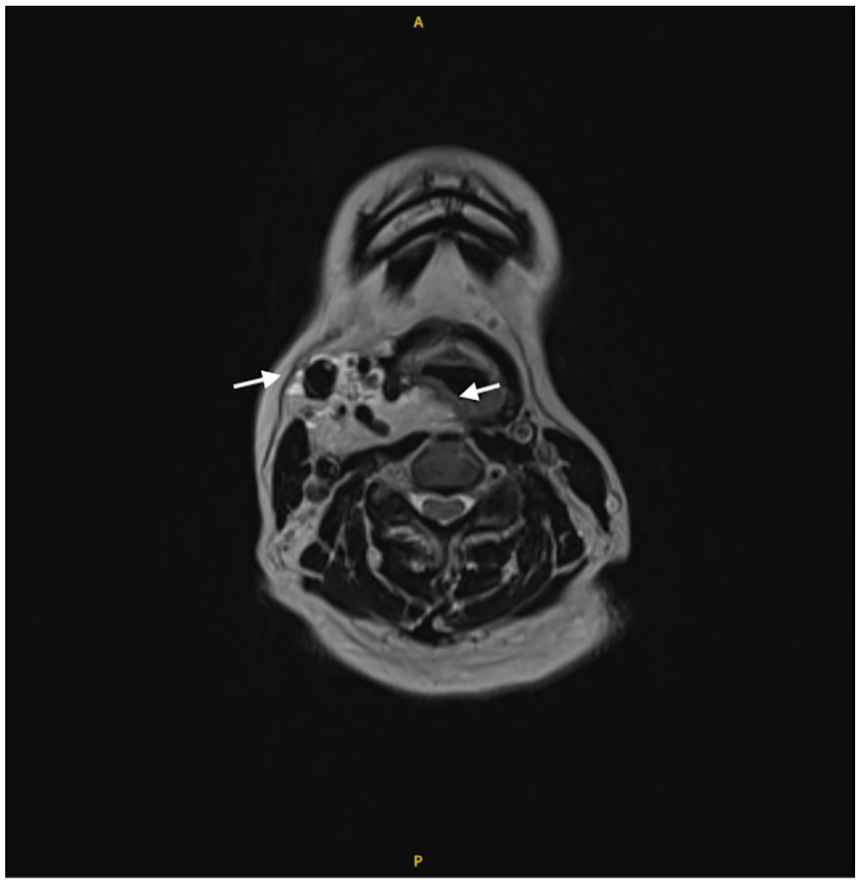
Right parapharyngeal mass extending to the right retropharyngeal space (arrow).
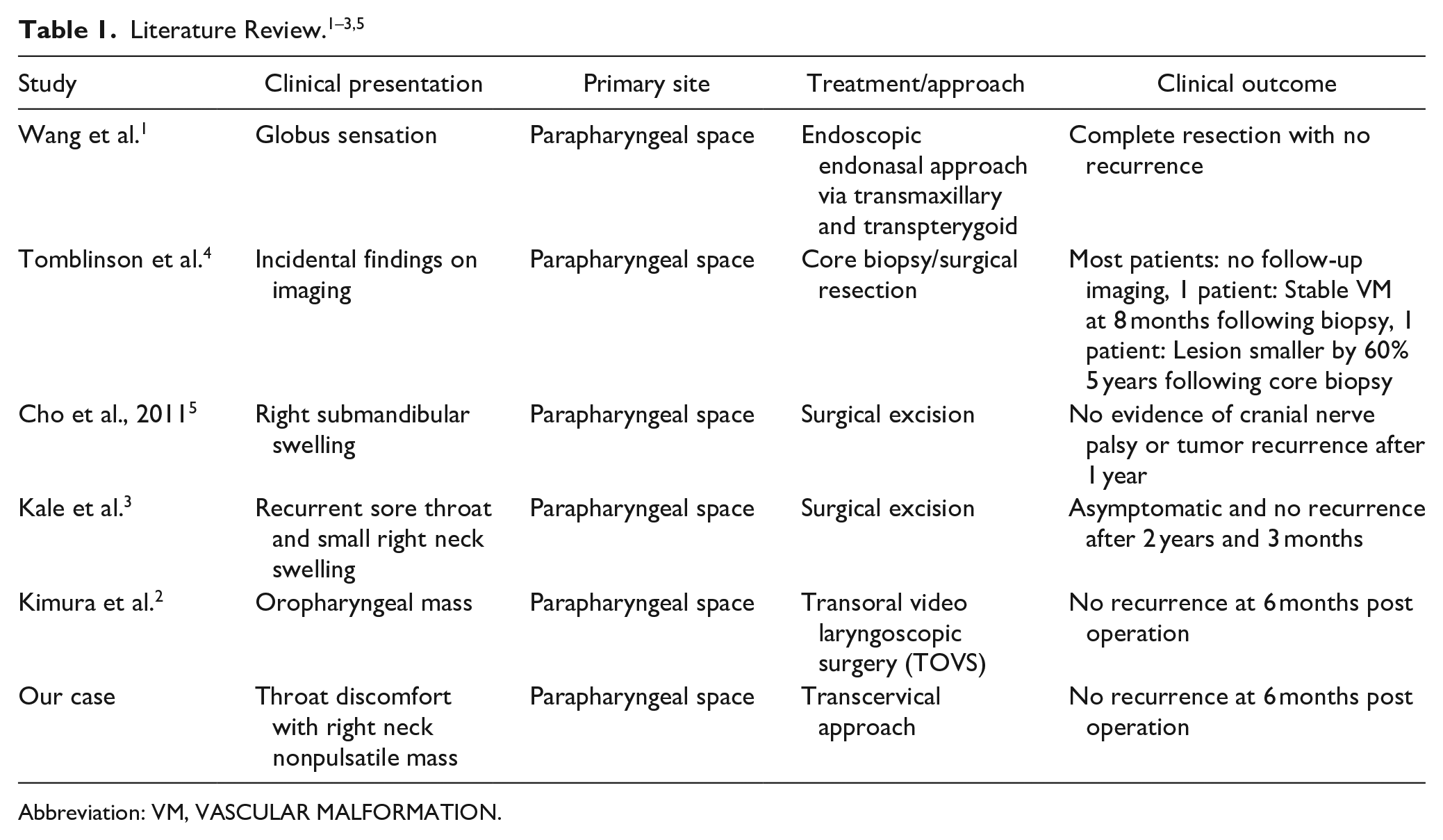
Abbreviation: VM, VASCULAR MALFORMATION.
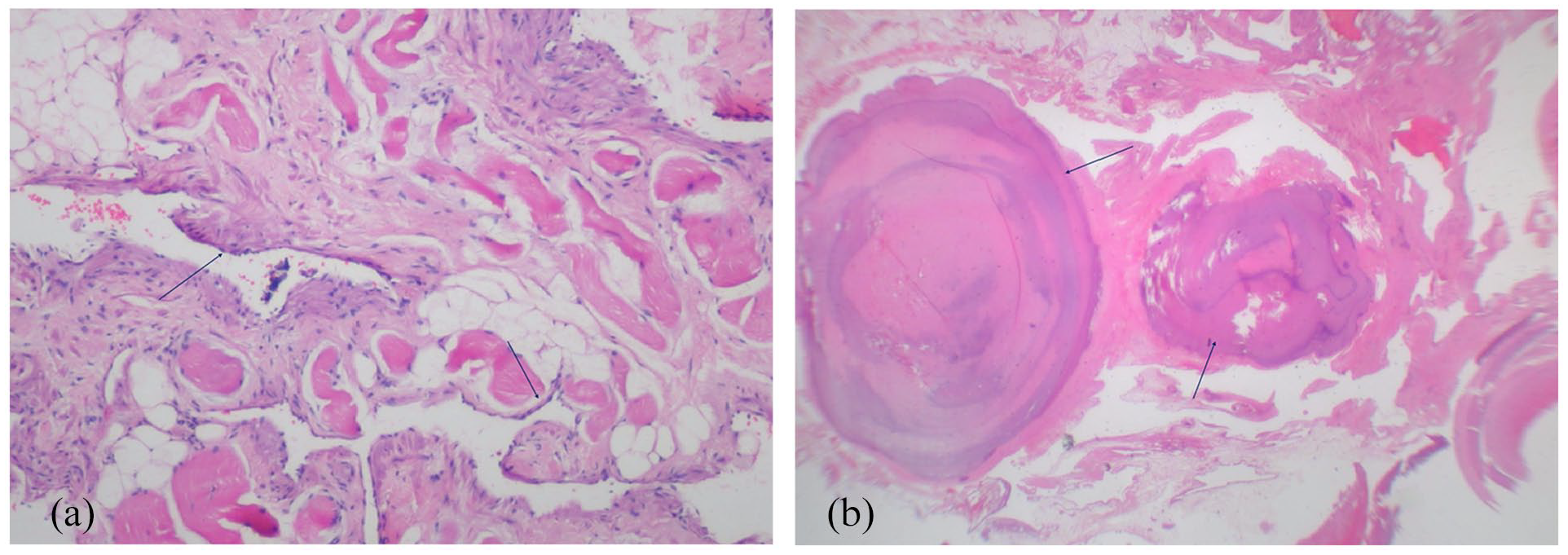
(a) Higher magnification shows flattened vascular endothelial lining (arrows). (b) Vessels with calcified thrombi/phleboliths (arrows).
Discussion
Parapharyngeal space tumors are generally nonmalignant, mainly in the form of salivary gland tumors followed by neurilemmomas. 2 Hemangiomas arising in head and neck region are mainly congenital and rarely seen in adults. 3 Wang et al. 1 reported that out of more than 1000 cases, cavernous hemangioma occurrence in the head and neck region includes only 0.5% to 1%, and only 8 cases have been reported to occur distinctively in parapharyngeal space. Hemangioma can be further divided into 3 subtypes which are capillary, mixed, or cavernous. 1 Cavernous hemangioma is a noncancerous vascular growth with typical histology characteristics, large, cystically dilated vessels with thin walls in which intravascular thrombosis and calcification are prevalent. 1 Female predominance with middle-to-late-age onset is demographically typical for cavernous hemangioma, corresponding to our reporting case. 1 The usual clinical presentations are dysphagia, otalgia, facial pain, foreign body sensation, and dysphonia. 1 Interestingly, our patient only presented with neck swelling without any associated symptoms. Moreover, one of the literature reviews also reported a case of parapharyngeal space cavernous hemangioma presenting with nontypical clinical signs which are recurrent sore throat and right neck swelling. 3 Symptoms suggestive of malignancy include referred otalgia, facial pain, trismus, and cranial nerve involvement, which are not evident in this case. 4
The gold standard imaging for cavernous hemangioma is MRI which reveals multi-lobulated soft tissue growth with an intermediate signal on T1, hyperintense signal on T2, and homogenous enhancement with contrast similar to our MRI finding. 1 Both MRI and Computed Tomography (CT) scans provide the utmost information on surgical approach and proximity of nearby structures for hemangioma resection. 1 A signal void is present in phlebolith, a diagnostic feature of vascular tumors. 4 This finding is seen in our case. However, very few case reports have shown evidence of phlebolith as a diagnostic feature.
Surgical resection is the mainstay of treatment. 2 The approach can be via transcervical, transparotid, mandibular swing, transoral video laryngoscopic, or endonasal transpterygoid/transmaxillary approach (Table 1). 2 The choice depends on site, size, tumor characteristics, and extension. 2 If surgical resection is not possible due to tumor size and location, as well as patient comorbidities, other treatment options are sclerotherapy, steroids, ionizing radiation, and laser surgery. 2 We had successfully excised our parapharyngeal cavernous hemangioma via the transcervical approach, which is the conventional surgical approach used in most literature reviewed (Table 1).
Conclusion
Cavernous hemangioma is a benign vascular lesion with a rare incidence in the head and neck region, especially the parapharyngeal space. Given the vast differential diagnoses that exist for parapharyngeal space mass, its distinct radiological findings, with MRI being the gold standard investigation, are essential to prevent missing this diagnosis in hand. The main management of cavernous hemangioma is surgical intervention and the approach used mainly depends on tumor location, ex-tension and involvement, and proximity of major vessels.
Footnotes
Acknowledgements
None.
Authors’ Contributions
S.E.R. drafted the article. S.G. and L.Y.T. supervised the drafted article. D.B-L.O. prepared and analyzed histopathology slide for this case.
Availability of Data and Material
Not required.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
Not required.
Consent for Publication
Not required.