
Abstract
Parapharyngeal liposarcoma is a rare malignant tumor, the pathogenesis of which is uncertain. Parapharyngeal liposarcoma often causes nonspecific clinical features, including dysphagia, globus sensation, and/or respiratory disturbances. The parapharyngeal space is a rare location for head and neck liposarcoma, and these lesions may therefore be confused with a variety of other tumors that can originate in this area. Here, we report a case of liposarcoma originating from the prestyloid parapharyngeal space and discuss the possible differential diagnosis on radiographic findings.
Introduction
Although lipomas are the most common mesenchymal neoplasms, they are uncommon in the head and neck area where they account for about 13%–20% of lesions.1,2 Lipomatous head and neck tumors most commonly affect the superficial posterior neck, 2 although the whole head and neck area can be affected. The malignant to benign ratio of lipomatous tumors is reportedly about 1:100. 3
The parapharyngeal space (PPS) is a rare site for neoplasms in the head and neck, representing only 0.5% of head and neck tumors. Parapharyngeal liposarcoma is an extremely rare malignant tumor, the pathogenesis of which is still unknown. These tumors often cause nonspecific clinical symptoms, including progressive dysphagia, globus sensation, and/or respiratory disturbances. 4
Here, we report a 55-year-old man with a liposarcoma arising in the prestyloid PPS, which responded well to surgery and postoperative radiation therapy.
Case
A 55-year-old man was admitted to our institute because of swelling of the right oropharynx that had occurred 1 month earlier. He was treated under a diagnosis of peritonsillar abscess at another hospital, but was referred to our hospital because there was no improvement. The patient had no specific history other than hypertension. A physical examination revealed swelling of the right oropharyngeal wall, and there were no other palpable masses in the neck. Neck computed tomography (CT) showed a mass with a long diameter of 5.3 cm in the right PPS with inhomogeneous contrast reduction and oropharyngeal compression. There were no other abnormal findings in the thyroid gland, parotid gland, or lymph nodes. Neck magnetic resonance imaging (MRI) showed similarly sized lesions in the right PPS with a heterogenous high signal intensity on T2-weighted imaging (T2-WI) (Figure 1A) and iso to high signal intensity on T1-weighted imaging (T1-WI). (Figure 1B) The lesion showed good contrast enhancement, high signal intensity (Figure 1C), and limited diffusion on diffusion-weighted imaging (Figure 1D). MRI showing a right parapharyngeal soft tissue mass with iso to high signal intensity on T1-weighted imaging (A) and a heterogenous high signal intensity on T2-weighted imaging (B). The lesions showed strong enhancement and high signal intensity (C) with diffusion restriction (D).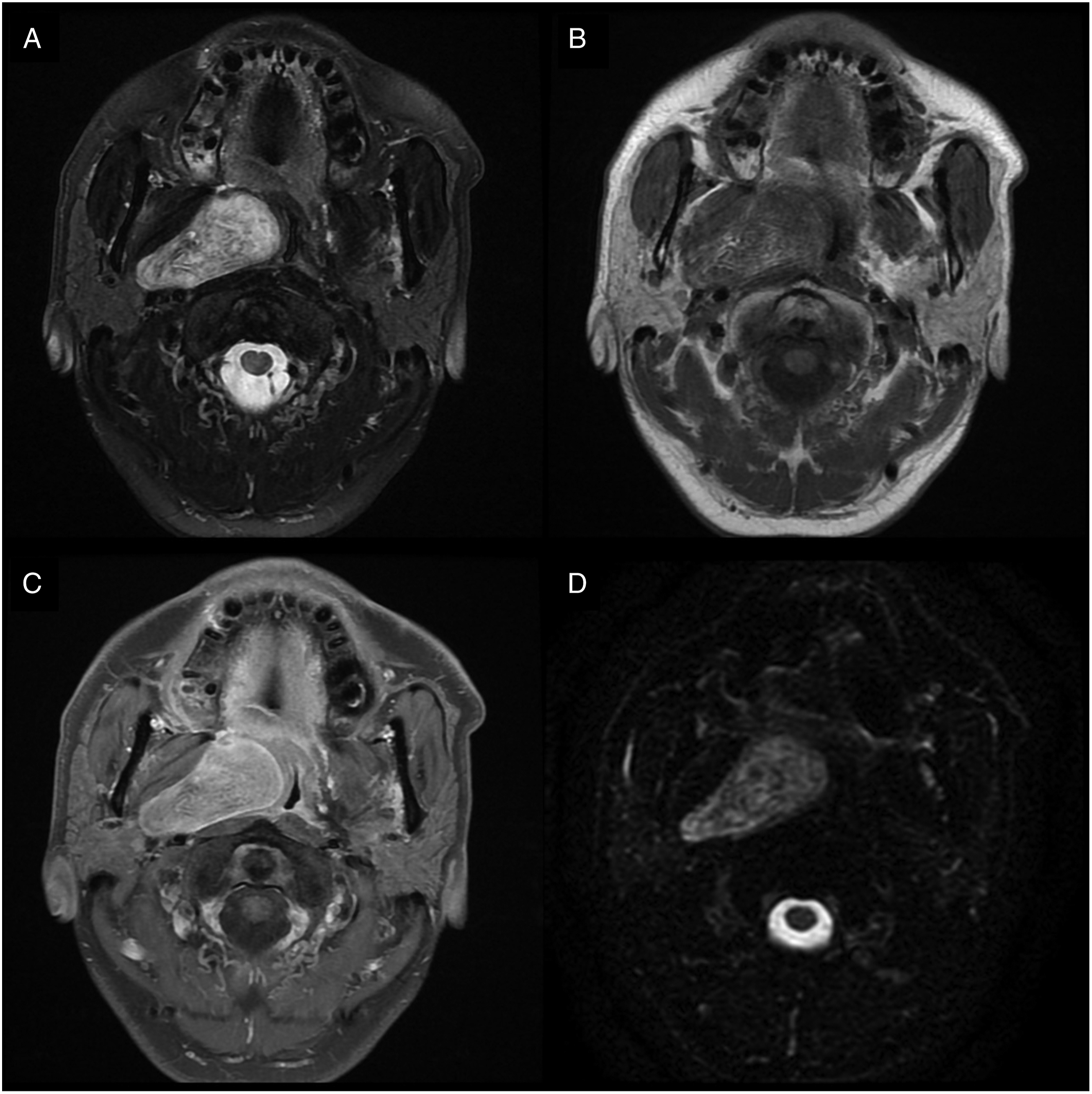
For diagnosis and removal of the mass, surgery was performed using a cervical approach under general anesthesia. The mass was confirmed in the right PPS after securing the field by removing the right submandibular gland. Due to the size and location of the tumor, the resection margin was not sufficiently secured and only the encapsulated tumor was removed. A pathological examination showed that the tumor consisted of atypical fibrotic and adipocytic components. It also showed amplification of MDM2, which can distinguish a lipoma from a well-differentiated liposarcoma (Figure 2). The tumor consisted of fibrotic and adipocytic components (A). Atypical, hyperchromatic stromal cells (arrowhead) were present in the fibrotic area (B). A few adipocytes showed atypical nuclei (C). The tumor cells showed diffuse nuclear expression of MDM2 (D).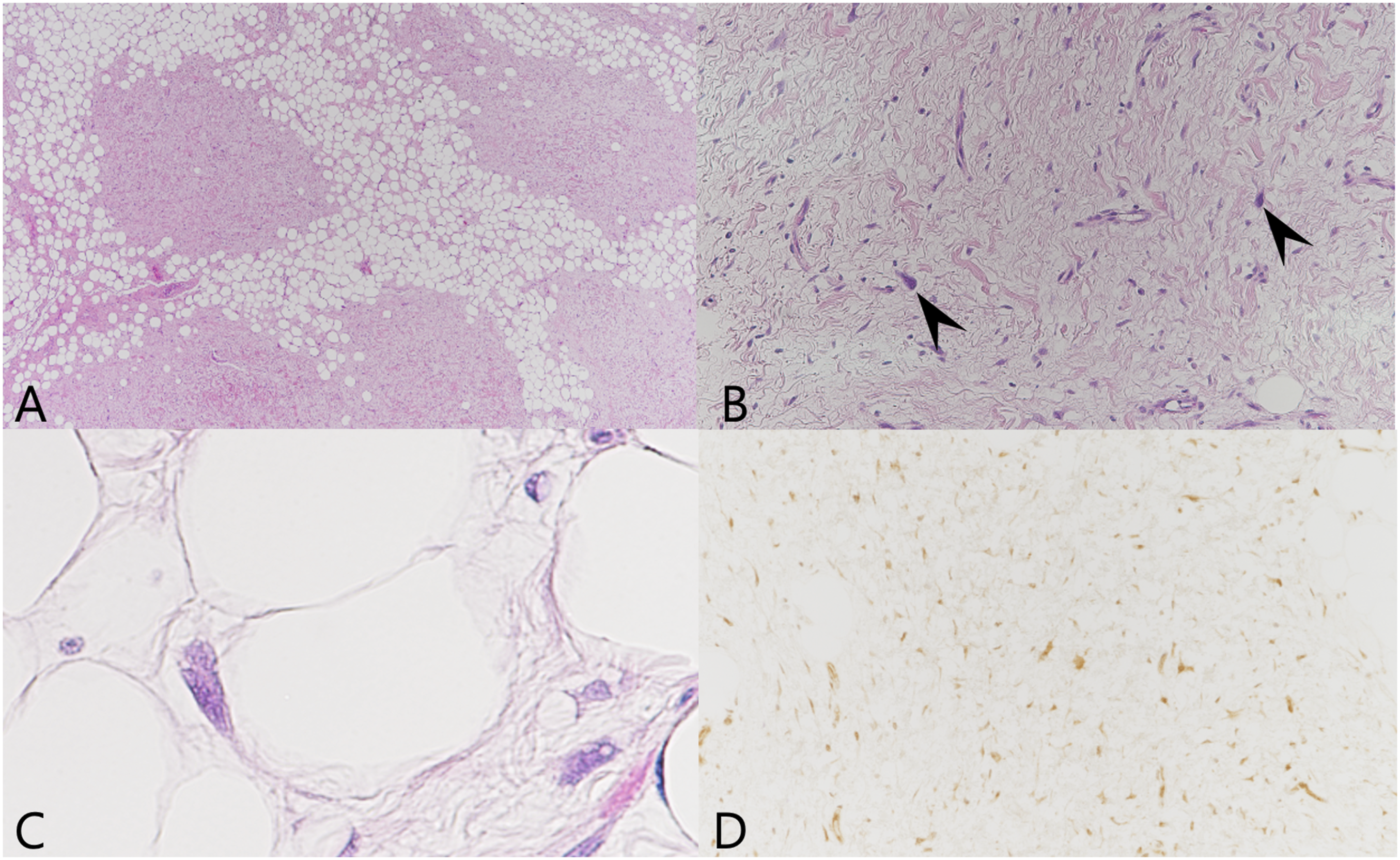
The patient was discharged without complications 1 week after surgery. During an outpatient physical examination 1 month after surgery, there was no evidence of specific findings, such as bulging of the lateral oropharyngeal wall or complications. Radiation therapy was subsequently performed at another hospital for 2 months. There was no evidence of recurrence or metastasis in the oral cavity, trachea, and neck during the 5-year follow-up period in this case.
Discussion
The PPS is divided into prestyloid and poststyloid compartments separated by fascia from the styloid process to the tensor veli palatini. About 70%–80% of PPS tumors are benign, and most tumors involving the prestyloid PPS are either salivary gland tumors or neurogenic tumors. 5
Liposarcomas account for only 2%–9% of malignant mesenchymal tumors encountered in the head and neck, and only a few cases have been reported in the PPS. 6 Liposarcoma in the PPS was reported to be a slow-growing tumor with no clinical symptoms until reaching a large size.7,8 These tumors often cause nonspecific clinical symptoms, including dysphagia, globus sensation, dyspnea, hoarseness, and obstructive sleep apnea. 9 In our case, the clinical symptoms were nonspecific, and bulging of the right lateral wall discovered by oropharyngeal inspection was the only sign suggesting a PPS tumor.
The differential diagnosis of liposarcoma is based on a combination of clinical, radiological, and histological analyses. A radiological workup, including CT and MRI, is important because the PPS is a difficult anatomical region from which to obtain adequate cells or tissue for preoperative diagnosis. 10
CT findings can be used for differential diagnosis according to the subclassification of liposarcoma; a well-differentiated liposarcoma shows low attenuation, similar to a lipoma and subcutaneous fat, and the fibrous septa may be thicker and more irregular or nodular than in a lipoma. 11 In our case, the findings revealed liposarcoma due to its larger size than a lipoma and inhomogeneous enhancement.
On MRI, a lipoma typically has the appearance of a homogenous fatty mass, with hyperintensity on T1-WI, and it shows a proportional reduction in intensity on T2-WI. 12 In comparison to a lipoma, liposarcomas show a partially inhomogeneous signal intensity and foci of high signal intensity on T1-WI indicating a lipomatous mass, and the intensity of the fat signal is correlated with the degree of differentiation of the liposarcoma. 13 In conjunction with diffusion-weighted imaging (DWI), lower values of the apparent diffusion coefficient (ADC), which can be used to quantify the effect of diffusion restriction, are found in a liposarcoma in comparison to benign soft tissue tumors, although it has proven difficult to determine appropriate cutoff values for the ADC for benign and malignant soft tissue sarcomas.14,15 In this case, a liposarcoma was suspected based on MRI findings: iso to high signal intensity on T1-WI, a heterogeneously high signal intensity on T2-WI, good contrast enhancement, and diffusion restriction on DWI.
Surgical removal of the tumor is the treatment of choice, and it is essential to confirm the diagnosis of a well-differentiated liposarcoma. A number of surgical approaches are available for these lesions, including transcervical, transparotid gland, and cervicoparotid approaches, the selection of which is determined by the location, size, surrounding blood vessels, and malignancy potential of the lesion. 16 In this case, as PPS liposarcomas are rare, a diagnosis of lipoma was initially considered prior to surgery. Due to the tumor location, we chose transcervical excision in conjunction with submandibular gland excision because wider exposure as in the cervicoparotid approach is not helpful to secure the posteromedial margin of the tumor. Liposarcomas are radiosensitive tumors, although the efficacy of radiation therapy in this area is controversial. In locations where wide local excision with a secure margin is impossible or contraindicated by anatomical limitations, radiation therapy can be an adjunctive therapy for liposarcoma. 10
Conclusion
Liposarcoma is a rare tumor that can arise in the PPS. Although differential diagnosis from a benign lipoma is difficult, preoperative CT and MRI may provide diagnostic insight. Based on our experience, MRI is recommended for the evaluation of PPS masses. Complete excision with a secure resection margin for PPS malignant tumors is difficult because of the anatomical characteristics. Adjuvant radiation treatment may be helpful in treatment of a PPS liposarcoma.
Footnotes
Acknowledgment
This work was supported by the Soonchunhyang University Research Fund.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases.
Human and Animal Rights
This article does not contain any studies involving human or animal subjects and the research was conducted by reviewing medical records of patient.
Informed Consent
Informed verbal consent was obtained from the patient reported in this manuscript.