
Abstract
We introduce here our surgical approach for the removal of a huge parapharyngeal tumor in 3 cases. Surgery was done under general anesthesia using transnasal intubation. Transoral manipulation was performed first. Using a tongue retractor and an angle widener, a wide surgical field was provided. Incision was made on the palate around the tumor. Tumor was separated from the surrounding tissue, preserving the tumor capsule. Then, a 5-cm small skin incision was made. Both parotid and submandibular glands were pushed upward, and the parapharyngeal space was opened. The tumor was also separated from the surrounding tissue. These manipulations were done under endoscopic observation. Finally, the tumor was pushed laterally and safely removed intraorally. After removal of the tumor, the wounds were closed, and vacuum drainage was settled for a few days. No apparent problems, such as malocclusion and facial palsy, occurred, and the patients were free from disease for more than 10 years. For the removal of a large parapharyngeal tumor, the mandibular swing approach is usually used; however, this approach is invasive, and certain sequelae, such as facial wound and malocclusion, may occur. Our technique enables the safe and less invasive removal of such a huge parapharyngeal benign lesion.
Introduction
Various tumors occur in the parapharyngeal space (PS) and show various symptoms.1-10 However, the PS is located deep in the head, and a tumor in the PS is usually asymptomatic and may grow to a huge size. 11 In this article, we introduce our experience of the removal of a large PS tumor using a less invasive technique.
Surgical Technique
A tongue retractor and an angle widener were applied, and a wide surgical field was obtained. Then, the palate was incised and the tumor was carefully separated from the surrounding tissue under endoscopic monitoring. During manipulation, meticulous care was administered to preserve the tumor’s capsule. Then, the tumor was almost separated, but the tumor’s lateral side and the adjacent deep lobe of the parotid gland were still attached. Thereafter, a submandibular skin incision was added. By elevating both the parotid and submandibular glands, the PS was observed. The tumor was safely separated from the deep lobe of the parotid gland. Finally, the tumor was pushed laterally and removed from the mouth. After irrigating the wounds, both oral and neck wounds were tightly sutured and vacuum drainage was settled.
Results
The approach was applied in 3 cases. Case 1 was a 62-year-old man and had noticeable oral mass, but no other symptoms had been noticed. He underwent surgery for colon cancer, and the anesthetist found oral tumor. He underwent tracheotomy, and surgery was safely performed this time. After the surgery, tracheotomy persisted, and the patient was referred to us. A large tumor was observed on his right palate, and biopsy revealed pleomorphic adenoma (Figure 1). Using the combination approach under endoscopic visualization, his tumor was safely removed (Figures 2 and 3). Because of the large palatal defect, skin graft was performed. Surgical time was 3.5 hours, and the amount of bleeding was 100 mL. Case 2 was a 37-year-old man who complained of abnormal pharyngeal sensation. A slight swelling of the palate was observed, but a huge tumor was observed on his left PS (Figure 4). Intraoral biopsy was performed, and a diagnosis of pleomorphic adenoma was made. Endonasal intubation was applied. The combined approach was applied, and the tumor was safely removed. Surgical time was 3.0 hours, and the amount of bleeding was 70 mL. After the surgery, the scar on the neck was not apparent (Figure 5). Case 3 was a 65-year-old man who complained of abnormal sensation of the mouth. A large tumor was observed on his right palate, and biopsy revealed benign adenoma (Figure 6). Endonasal intubation was also applied and surgery was done in the same manner as in cases 1 and 2. A diagnosis of basal cell adenoma was made (Figure 7). Surgical time was 3.0 hours, and the amount of bleeding was 50 mL. All patients had satisfactory postoperative skin and were free from disease for 10 years without facial palsy and malocclusion.
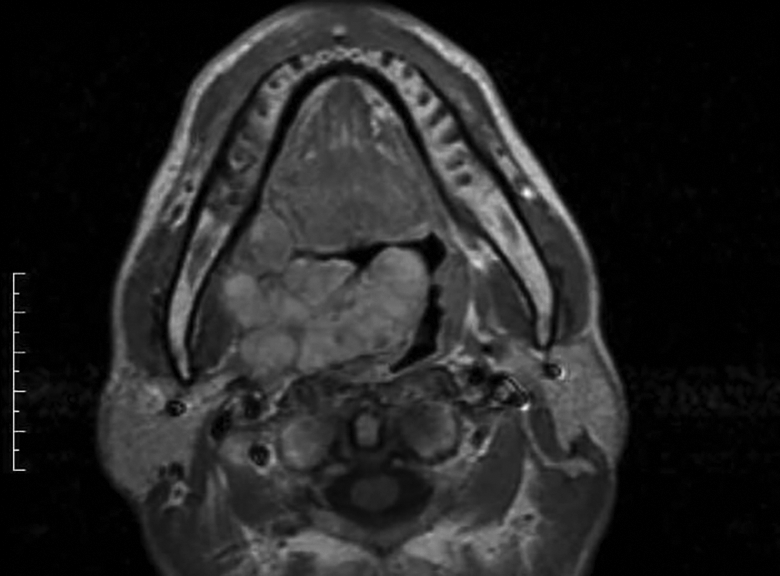
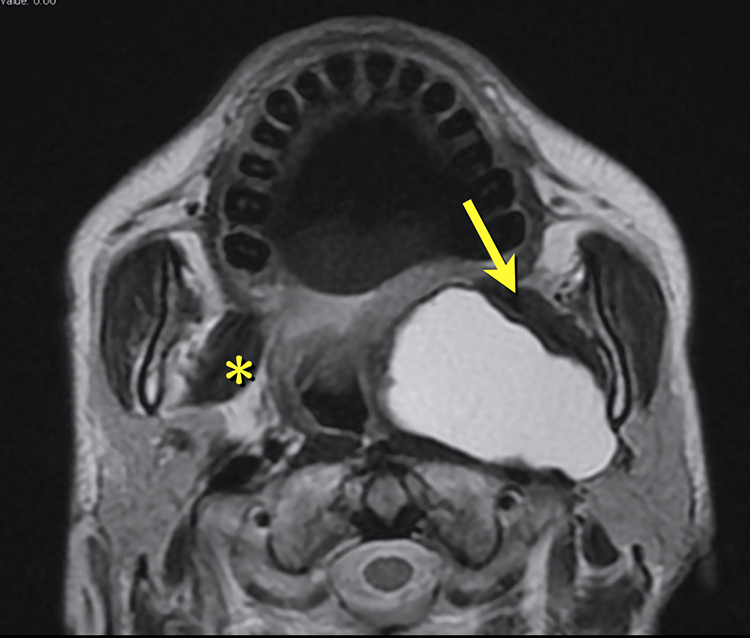
T1-weighted magnetic resonance (MR) image of case 1. This tumor measured 7 cm on the longest diameter. The tumor might have originated from the deep lobe of the right parotid gland and is difficult to access from either oral or cervical aspect.
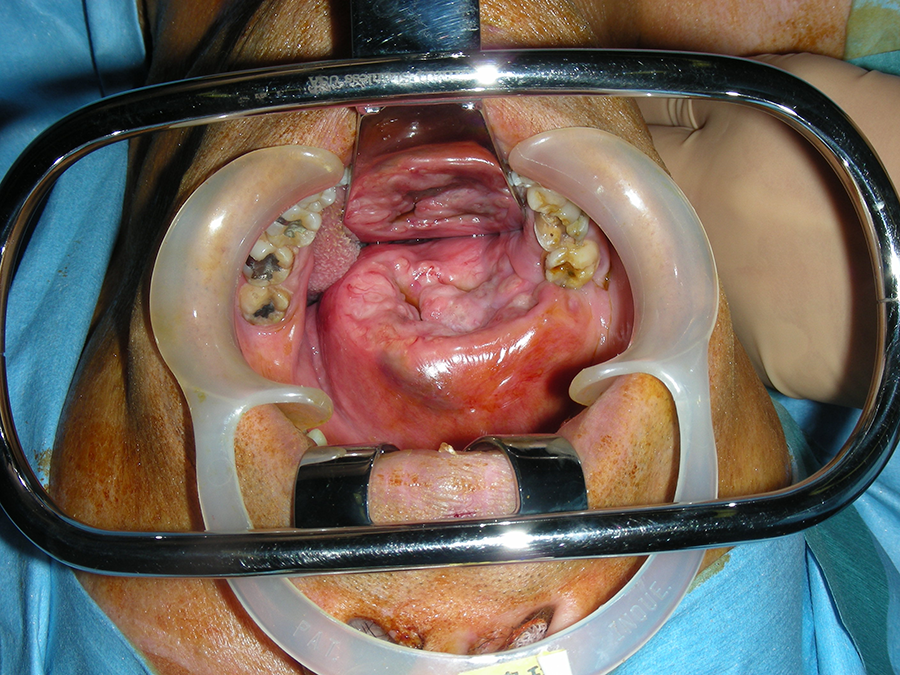
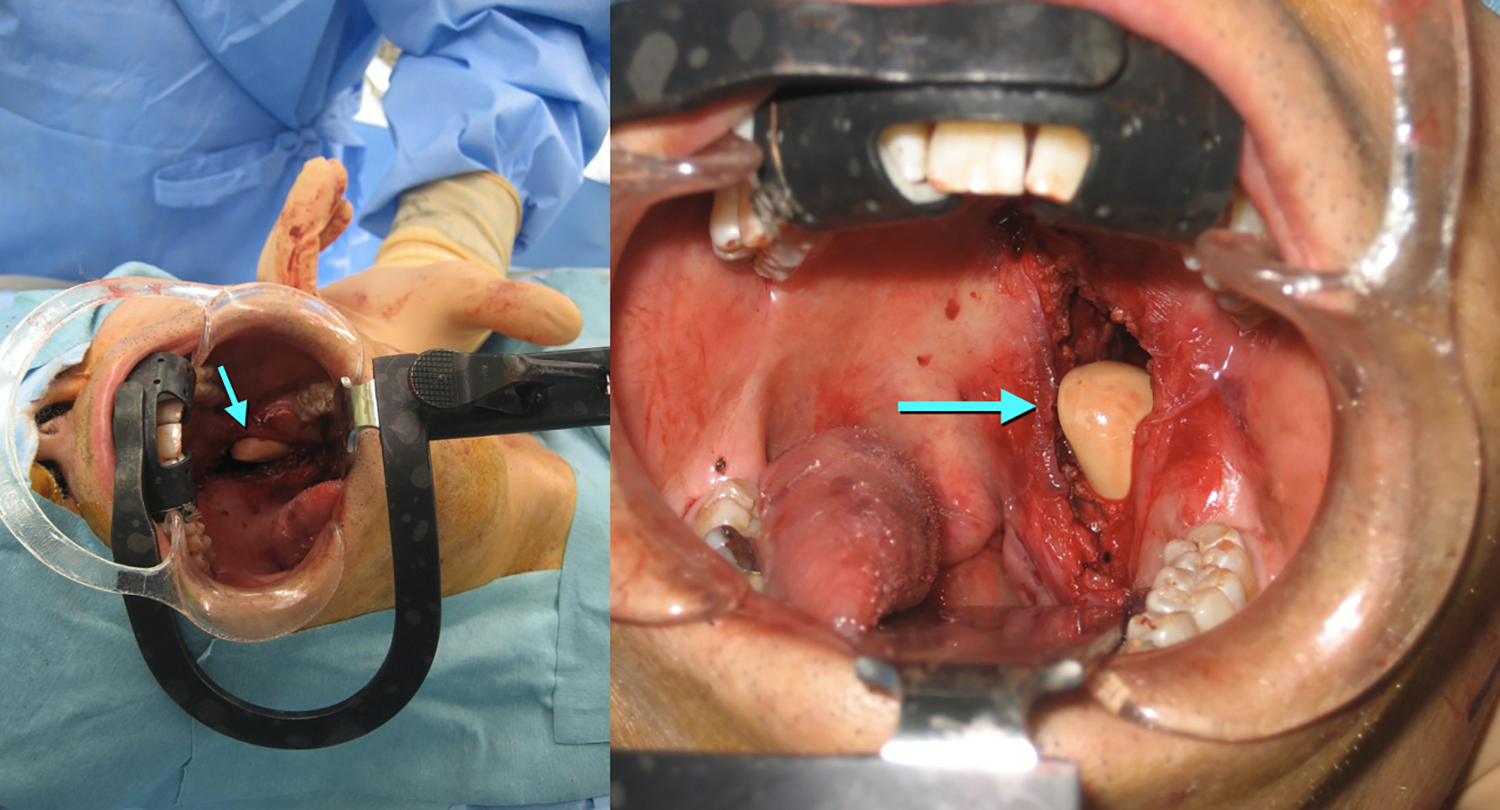
Tumor in case 1. The angle widener helps achieve better visualization.
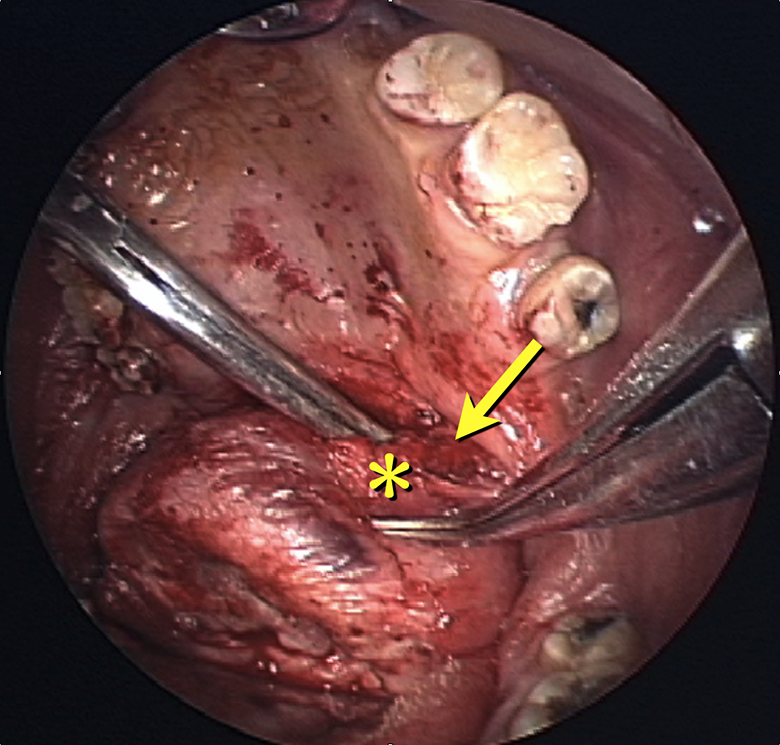
Endoscopic view during surgery (the image upside is inferior). The tumor capsule (*) attached to the medial pterygoid muscle (arrow) and was safely separated under endoscopic view.
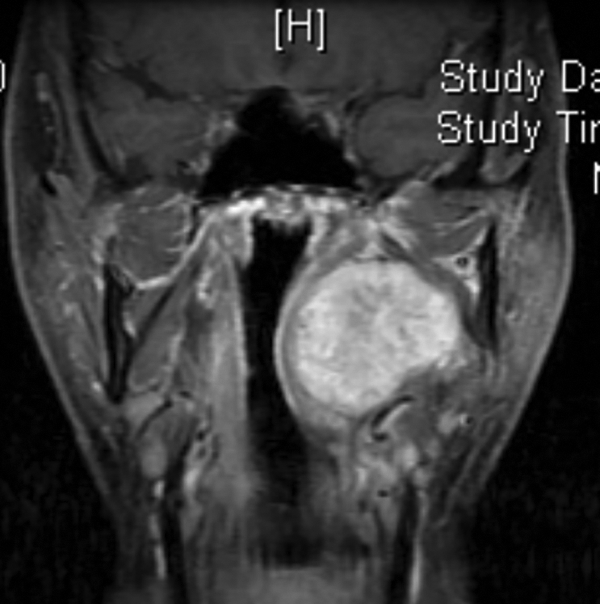
T1-weighted magnetic resonance (MR) image of case 2. This tumor measured 7 cm on the longest diameter and might have originated from the deep lobe of the right parotid gland.

The scar on the neck (arrow) was not apparent in case 2.
T2-weighted magnetic resonance (MR) image of case 3. This tumor measured 6 cm on the longest diameter. Medial pterygoid muscle (*) is located anterior to the parapharyngeal space (PS) and is good landmark for oral management under endoscopic observation (arrow).
Surgical view after tumor removal. Oral and cervical wounds were communicated and well visualized. The arrow indicates the digit of the surgeon. As shown in this figure, this approach offered good surgical field. However, the wound should be thoroughly irrigated to prevent postsurgical infection.
Discussion
Symptoms of parapharyngeal tumor vary, and malignant lesions tend to occur with otitis media with effusion. In contrast, most benign lesions are asymptomatic. 5 Therefore, PS tumors sometimes grow huge in size in the PS. Especially, the key for the safe removal of pleomorphic adenomas is total removal without damage to its capsule, otherwise, local recurrence may occur. In addition, these tumors sometimes show malignant change. This condition is frequently seen in pleomorphic adenoma patients with a long history and residual tumor after the inappropriate removal of the tumor. To avoid capsular damage, a wide and sufficient surgical field is required. Therefore, the mandibular swing approach is done for huge tumors; however, surgery itself is invasive to the patient, and malocclusion may occur.12-14 The transoral approach is less invasive for the extirpation of tumors in the PS, and an assistance of endoscopy facilitates the surgery. 15 The use of an angle widener, formerly used in the dental clinic, facilitates the surgical procedure. 16 However, the lateral side of the PS is a difficult area under intraoral manipulation alone. Especially, the PS contains carotid artery, jugular vein, and vagus nerve, and intraoral surgical removal is thought to be difficult even under endoscopic observation. 10
The combination of intraoral and cervical approach allows safer manipulation. 17 However, areas behind the tumor tend to be blind areas. An excessive elevation of the tumor may cause damage on the tumor capsule, leading to tumor recurrence. Pushing a tumor medially from the neck facilitates oral management. In the present cases, however, tumors were too large and deeply situated to remove oral management alone even pushing tumor from the neck. Using an endoscope and an adequate surgical device, the tumor can be safely resected under clear observation. Especially, during manipulation on the lateral side of the tumor, both cervical and intraoral resections can be visualized. This allows safe tumor removal without damaging the tumor capsule.
The surgical indication of this surgery should be based on magnetic resonance images. Like in these cases, the surgical field posterior to the medial pterygoid muscle is very limited and hazardous even under endoscopic manipulation. In these situations, the cervical approach is very helpful even with small skin incisions. However, sufficient margins could not be obtained, so this approach is not suitable for malignant tumors. Before surgery, histological assessment, at least fine needle aspiration cytology, is indispensable for this approach.
Recently, a combined approach under robotic surgery has been reported. 18 Although robotic surgery achieves safer surgery, it requires a robot surgical device and is very expensive. Our method only needs a nasal endoscopic system and conventional devices and therefore can be performed by a regular Ear Nose and Throat clinic.
Although the present cases are rare, this method is unsuitable for malignant lesions, and preoperative image and pathological assessments are necessary. 17 However, our method is safe and less invasive for the treatment of huge PS tumors.
Supplemental Material
Supplemental Material, permission - Endoscopy-Aided Combined Intraoral and Cervical Approach for a Huge Parapharyngeal Benign Tumor
Supplemental Material, permission for Endoscopy-Aided Combined Intraoral and Cervical Approach for a Huge Parapharyngeal Benign Tumor by Atsunobu Tsunoda, Seiji Kishimoto, Miri Tou, Takashi Anzai, Fumihiko Matsumoto, Shinichi Oba and Katsuhisa Ikeda in Ear, Nose & Throat Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.