
Abstract
Lipomas are benign soft tissue tumors frequently observed throughout the body. Lipomas rarely cause health concerns; however, when symptomatic, it is often related to their location and size. A 65-year-old male patient presented with a non-tender, enlarging mass in the anterior floor of the mouth, which was otherwise asymptomatic. Computed tomography evaluation revealed an unusually large hypolucent mass, posterior to the inner table of the right anterior mandible. Surgical excision was uncomplicated. Upon follow-up, the right anterior floor of the mouth wound healed without compromise of the lingual or hypoglossal nerves or Wharton’s duct. This discussion highlights the infrequent occurrence of lipomas in the oral cavity, particularly in the floor of the mouth, including patient presentation, preoperative evaluation, and surgical planning.
Keywords
Introduction
Lipomas are common soft tissue tumors that appear throughout the body; however they infrequently occur in the mouth. Usually occurring between the ages of 40 and 60 years, they are generally slow-growing and cause minimal symptoms. There are conflicting reports of gender distribution being approximately equal versus 3:1 distribution, male to female. Lipomas account for approximately 1.0% to 4.4% of benign intraoral neoplasia.1 -3 Oral and maxillofacial lipomas most often occur in the parotid region, followed by the buccal mucosa. 1 These oral mesenchymal tumors are less common on the floor of the mouth accounting for only 4% of these lesions. Sizes range from 0.5 to 8.0 cm, with a mean of 2.2 cm. 1 Histologically, there are many classifications of lipomas: simple lipoma, adenolipoma, angiolipoma, chondroid lipoma, fibrolipoma, myelolipoma, myolipoma, myxolipoma, ossifying lipoma, sclerotic lipoma, and pericallosal lipoma. 4 Histopathologically, between 45% and 50% of intraoral lipomas fall into the subclassification of classic lipoma.1,2,5 The differential diagnosis of intraoral tumors includes dermoid, epidermoid/lymphoepithelial cysts, ranula, pleomorphic adenoma, mucocele, and mucoepidermoid carcinoma. Although malignant transformation is rare, treatment requires surgical excision while considering nearby structures. Neuromonitoring and imaging are techniques that assist in precise diagnosis, surgical planning, and complication prevention.
Case Report
A 65-year-old man presented to my office, Arizona Coast Ear, Nose, Throat, Allergy & Sleep Medicine, with a 5-year history of a slowly enlarging right sublingual mass. There was no previous radiographic evaluation or biopsy. He denied current or previous history of tobacco use. There was no reported history of difficulty with speech or swallowing; however, the patient reported increasing lump sensation. On physical examination, there was no dysphonia or disarticulation. A soft, non-tender mass on oral bimanual palpation extended into level I neck (Figure 1). There were no other masses. Radiographic evaluation revealed an approximately 6-cm hypolucent right sublingual mass (Figure 1). The patient elected for excision, given enlargement and associated symptoms. Removal of the mass intraorally resulted in no complications (Figure 2). Wharton’s duct was displaced laterally, and the lingual nerve coursed medially to the mass. The mass was not adherent to the sublingual gland. Pathology revealed a well-circumscribed, thinly encapsulated lipoma (Figure 2). Follow-up at 3 months revealed a well-healed floor of mouth without long-term complications.
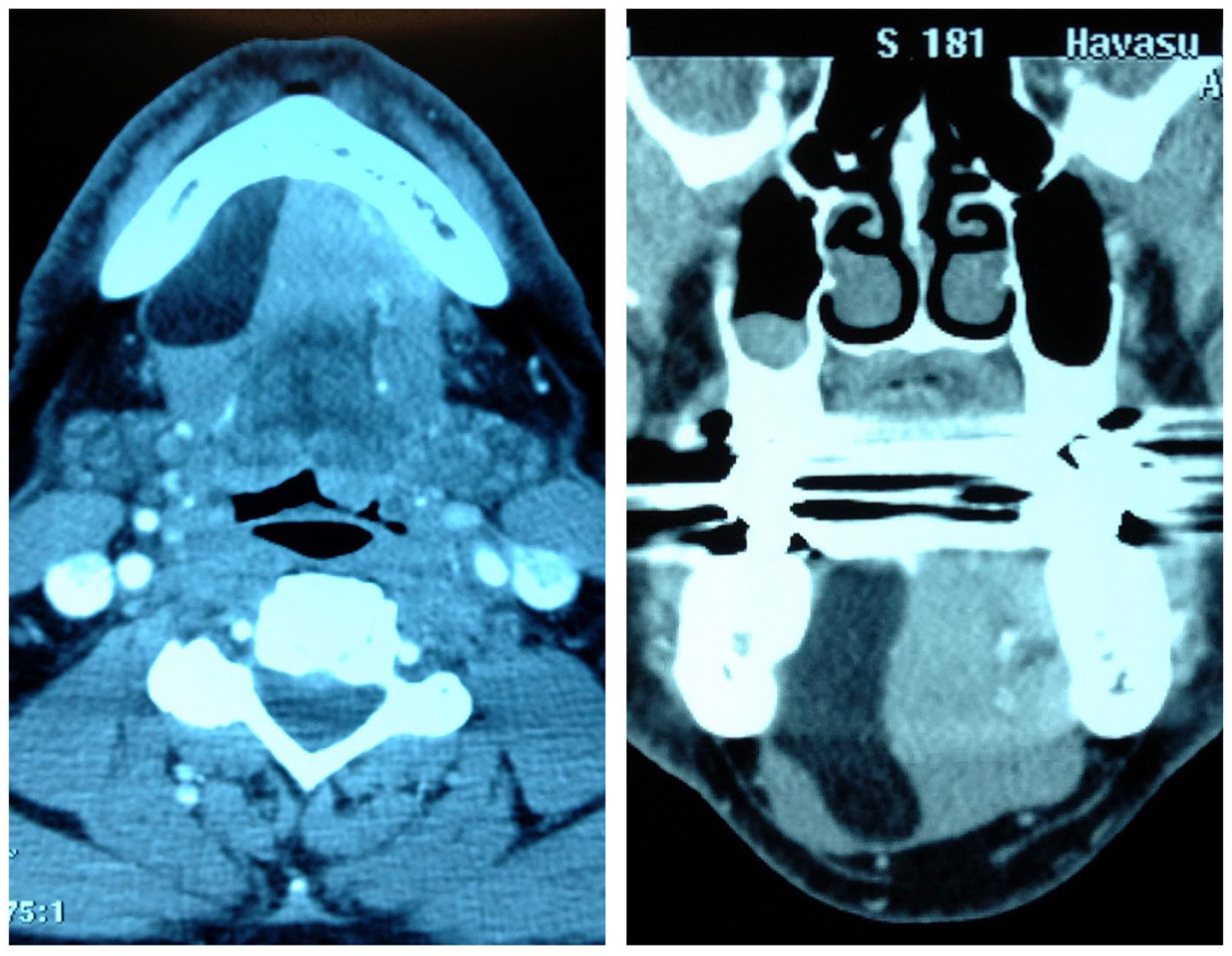
Axial and coronal computed tomography.
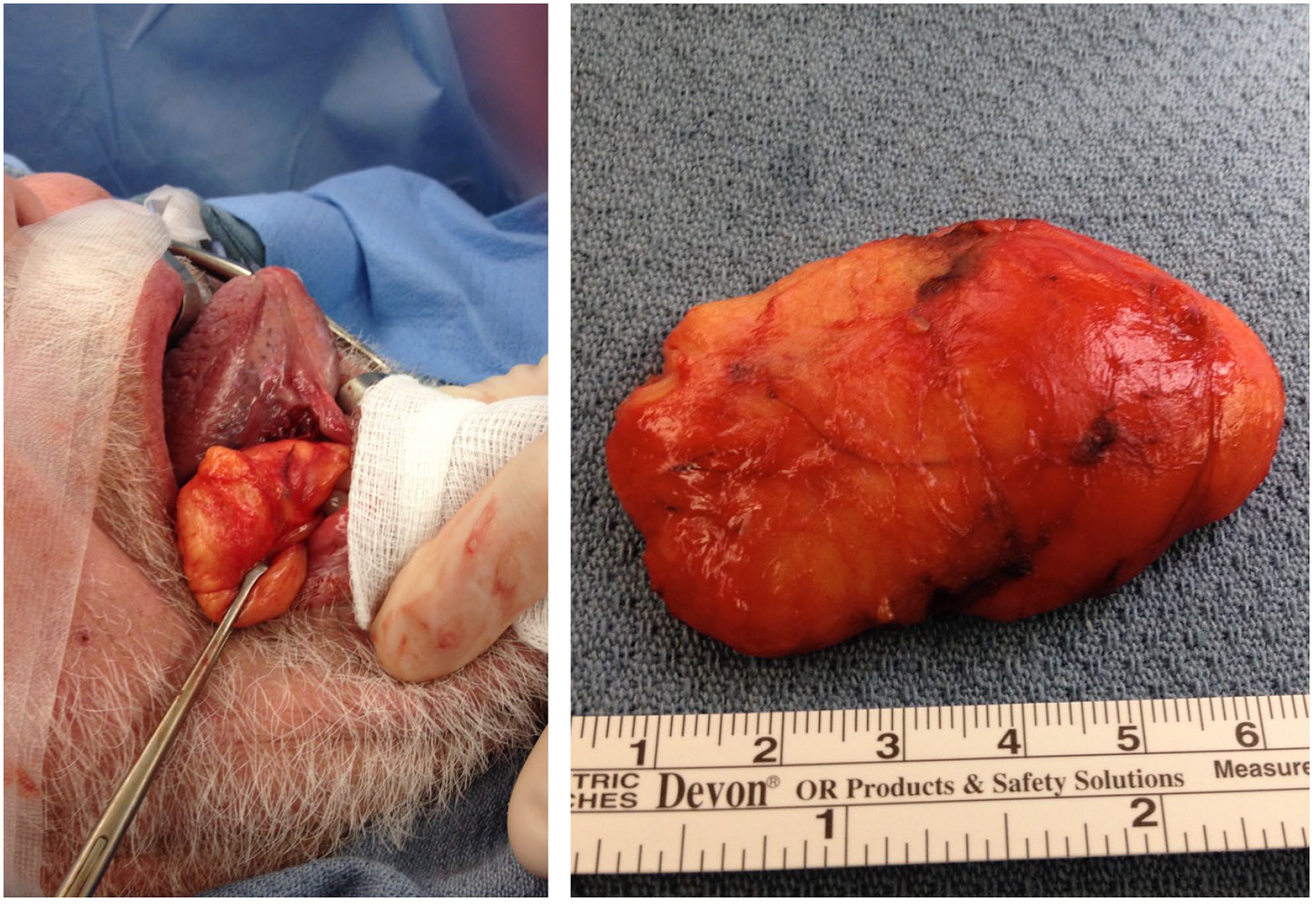
Intraoperative view. Gross pathology.
Discussion
Benign lipomas are the most commonly seen mesenchymal neoplasms, although they are uncommon intraorally. Statistically, lipomas account for approximately 1.0% to 4.4% of benign intraoral neoplasia.1 -3,6 Lipomas affect many sites intraorally, most commonly occurring in the parotid region and buccal mucosa.1,2 Lipomas on the floor of the mouth are rare, comprising only 4% to 11%.1,2
The etiology of lipomas has yet to be fully understood; however, multiple proposed theories exist. Some suggestions conclude that lipomas may be associated with obesity and the unintentional growth of fatty tissue. 7 Lipomas may originate from embryonic sequestrations of multipotential cells activated by hormones in adolescence. 8 Furthermore, trauma or persistent irritation of adipose tissue can lead to the development of lipomas.2,8
Most intraoral lipomas are small, slow-growing tumors, averaging approximately 2 cm, and are typically asymptomatic. 1 However, lipomas occurring on the floor of the mouth can grow more extensively, as evidenced in this case. Large lipomas within the floor of the mouth can cause dysphagia and dysarthria.9 -11 In severe cases, it can cause hypoglossal nerve palsy. 11
Lipomas are composed of adipose tissue surrounded by a thin layer of fibrous tissue, as seen through histology. Diverse, subclassified variants include classical/simple, adenolipoma, angiolipoma, chondroid lipoma, fibrolipoma, myelolipoma, myolipoma, mycobiome, ossifying lipoma, sclerotic lipoma, and pericallosal lipoma. 4 In the case reported, the histopathological analysis revealed a classic lipoma, the most common variant of intraoral lipomas, consisting of between 45% and 50% of all intraoral lipomas.1,2,5 However, specifically located within the floor of the mouth, classic lipomas and fibrolipomas are equally present.
The most common treatment is conservative surgical excision. Surgical removal of a lipoma of this size within the floor of the mouth can be challenging due to the dense neurovascular and glandular tissue present. When planning a surgical excision, it is crucial to consider the salivary glands, associated ducts, lingual nerves, hypoglossal nerves, and blood vessels. Inadvertent trauma during the procedure may also lead to ranula formation. 5 Neuromonitoring has been used to prevent damage to the lingual nerves. Some surgeons are incorporating neuromonitoring, despite the absence of established guidelines. 12 Preoperative imaging, computed tomography, and magnetic resonance imaging, assist in accurate diagnosis and surgical planning.
Summary
Lipomas occurring in the oral cavity are uncommon, particularly within the floor of the mouth. Lipomas rarely cause pain, although mild discomfort is occasionally reported. While rare, these benign tumors can potentially develop into malignancies. The standard treatment is removal via surgical excision.
Footnotes
Acknowledgements
Bert Daugherty, MD, pathologist at Havasu Regional Medical Center.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Sponsorships
None.
Third Party Submissions
None.
Writing Assistance
None.
Clinical Trials
None.
Research Data
None.
Ethical Statement
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Written informed consent was obtained from the patient for anonymized information to be published in this article.
Supplemental Material/Data Availability
None.