
Abstract
Pterygopalatine fossa (PPF) abscess is an exceedingly rare occurrence. Typically, it has been reported in association with odontogenic infections or hematogenous dissemination. In this report, we present the first case of PPF abscess where no obvious underlying cause or primary infection was evident. The patient initially presented with a 2-week history of left ptosis and persistent headaches, which were subsequently accompanied by fever and limited mouth opening. Based on elevated inflammatory markers and imaging findings, the diagnosis of a PPF abscess was established. Successful treatment was achieved through surgical drainage using an external cervical approach. Cultures from the aspirated pus identified Streptococcus constellatus as the causative agent. This case highlights the importance of considering PPF abscess in patients presenting with ptosis as an initial symptom. When diagnosed, surgical drainage should be considered as a viable therapeutic option.
Keywords
Introduction
The pterygopalatine fossa (PPF) is a narrow, clinically inaccessible, cone-shaped depression situated in the anteromedial region of the infratemporal fossa, positioned between the maxilla and the pterygoid process, in proximity to the orbital apex. Although it does not serve any specific functions, this space maintains connections with various anatomical structures: it links to the middle cranial fossa via the foramen rotundum and the pterygoid canal posteriorly, communicates with the orbit through the inferior orbital fissure anteriorly and superiorly, connects to the nasal cavity and nasopharynx through the sphenopalatine foramen and palatovaginal canal medially, joins the infratemporal fossa through the pterygomaxillary fissure laterally, and extends to the oral cavity through the greater palatine canal inferiorly.1 -5
Within the PPF, primary lesions are predominantly benign in nature, encompassing conditions such as schwannomas, juvenile angiofibromas, and meningoencephaloceles.6,7 Meanwhile, due to the intricate network of con-nections between the PPF and deep neck spaces, this region can potentially serve as a natural conduit for the local and regional spread of various tumors and infectious diseases through direct diffusion or neurovascular pathways. Tumors originating outside the PPF and infiltrating it are typically malignant, including nasopharyngeal carcinoma, sarcomas in the masticator space, as well as cancers of the palate, maxillary sinus, and the cheek. Infectious diseases, primarily invasive fungal sinusitis and bacterial sinusitis, and less frequently in inflammatory conditions like inflammatory pseudotumor, can also affect the PPF. 5
Nonetheless, the occurrence of abscesses within the PPF remains exceedingly rare, primarily because this anatomical region lacks lymphoid tissue. However, paradoxically, the absence of lymphatic drainage and the presence of numerous soft tissue spaces can facilitate the establishment and extension of a PPF abscess once it develops. Only 3 instances of orbital infections stemming from dental infections have been documented in the literature. These infections originated in the maxillary premolar and molar teeth, spread to the PPF and infratemporal fossa, and subsequently extended into the orbit through the inferior orbital fissure.8 -10 Additionally, there is a single reported case of PPF abscess formation resulting from hematogenous spread, which was a complication of chemotherapy. 11
In this case report, we describe the first reported case of a PPF abscess characterized by a negative blood microbial culture and the absence of any evidence of an underlying primary infection. This case was successfully managed with surgical drainage using an external cervical approach.
Case Report
A 43-year-old male presented to an outside institution with left ptosis and persistent headaches, particularly localized in the left occipital lobe. The discomfort worsened during chewing. He had no known prior significant medical illness other than a history of toothache 6 months ago. Laboratory assessments indicated elevated white cell count (14.3 × 109/L), neutrophil percentage (85.1%), and C-reactive protein (CRP) levels (30.77 mg/L). Cranial computed tomography (CT) angiography did not reveal any evidence of vascular abnormalities. Ten days after his initial presentation, subsequent laboratory tests indicated an increased white cell count of 18.9 × 109/L and a CRP level of 157.95 mg/L. Electronic nasopharyngoscopy did not reveal any remarkable findings apart from the identification of a cyst-like neoplasm in the posterior wall of the left nasopharynx. CT with iodinated contrast revealed a patchy mixed-density shadow within the left PPF. The boundary of this shadow was indistinct, with predominant enhancement at the periphery, consistent with characteristic imaging features of abscesses. Magnetic resonance imaging (MRI) with gadolinium contrast also confirmed the presence of a substantial abscess within the left PPF. Based on the patient’s clinical presentation and additional diagnostic findings, the diagnosis of a PPF abscess was established. Initial treatment involved intravenous antibiotic therapy, which did not yield significant relief.
Two weeks following the initial onset of symptoms, the patient was referred to our institution. By this time, there was a progressive deterioration in the ptosis of the eyes (Figure 1), and the headache had intensified, radiating throughout the head, and causing sleep disturbances. The patient also developed a fever (38.0 °C) and experienced noticeable restriction in mouth opening for the first time. Upon evaluation at our institution, a comprehensive ophthalmic examination was conducted, which revealed no apparent abnormalities in binocular vision, no diplopia, no limitations in extraocular motility in all directions, no impact on light reflexes, and no abnormal findings in optical coherence tomography and visual field assessments. Neurological examination did not indicate any sighs of meningeal irritation, and all other cranial nerves were functionally intact. Blood tests indicated a white cell count of 18.0 × 109/L, a neutrophil percentage of 85.5%, and a CRP level of 119.8 mg/L. Iodinated contrast CT and gadolinium-guided cranial MRI were repeated (Figure 2), confirming the progression of the abscess but no evidence of intracranial infection.

Preoperative photo showed the left ptosis half a month following the onset.
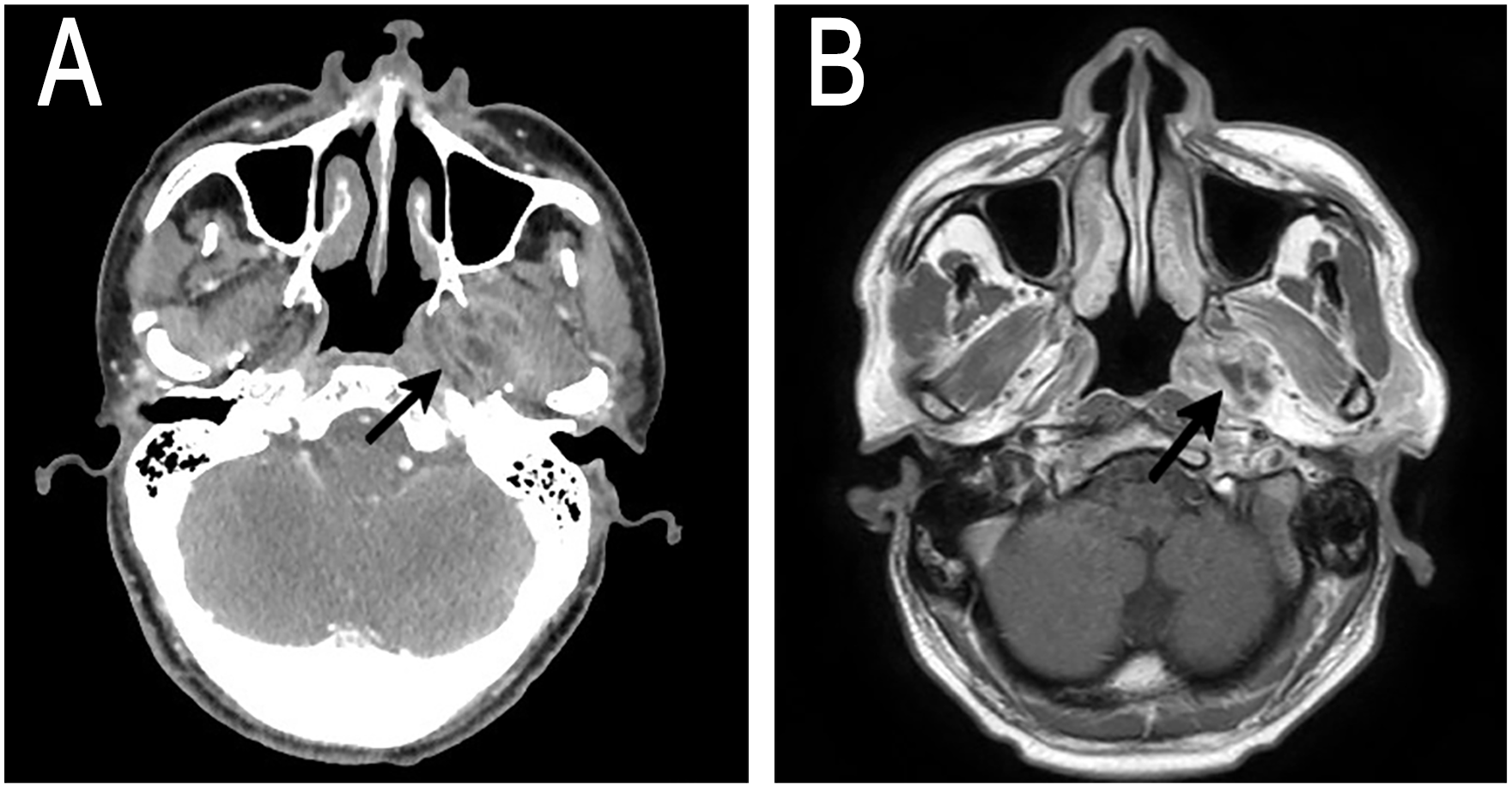
(A) Contrast-enhanced CT showed a patchy mixed-density shadow with peripheral enhancement in the left PPF (arrow). (B) T1 postcontrast axial MRI. Arrow pointed to the mass lesion.
Due to the persistent elevation of inflammatory markers and the poor prospects for conservative treatment, the patient underwent an immediate surgical exploration and drainage of the abscess. The surgical approach employed was an external cervical approach from the digastric muscle to the infratemporal fossa performed under general anesthesia, primarily for infection control. During the surgery, bloody purulent fluid and necrotic tissues were observed within the PPF, with an extension into the left parapharyngeal space and the skull base. Subsequent postoperative pathological analysis revealed significant infiltration of acute and chronic inflammatory cells and exudation of inflammatory necrosis. Three days following the surgery, culture results confirmed the growth of S. constellatus.
On the fifth day following surgery, the patient’s temperature and white blood cell count had normalized, and there was a substantial reduction in CRP levels, which decreased to 19.2mg/L. As a result of this positive progress, the patient was discharged from the hospital in good health on the 8th day after the surgical procedure. Over the course of 3 months, a gradual and consistent improvement in clinical symptoms was observed. A follow-up MRI was conducted, confirming the complete resolution of infection without any signs of recurrence.
Discussion
Diagnosing a PPF abscess solely based on clinical symptoms can be challenging due to its nonspecific nature. The primary symptoms typically encompass pain, fever, sore throat, dysphagia, odynophagia, restricted mouth opening, and facial numbness, primarily depending on the affected nerve. Consequently, it is often mistaken for conditions such as trigeminal neuralgia and maxillofacial tumors, leading to delayed treatment. In our case, the patient initially presented with left ptosis, indicative of left third cranial nerve palsy, and experienced headaches. Subsequently, fever and noticeable mouth opening limitations developed. CT and MRI scans revealed the presence of an abscess within the left PPF. The extension of this abscess into the medial and lateral pterygoid muscles and cavernous sinus resulted in clinical manifestations of ptosis and restricted mouth opening. This case highlights the importance of considering PPF lesions in patients who present with ptosis and headache as initial symptoms. Cranial nerve in-volvement can occur when there is direct extension into the skull base.
A typical diagnostic approach involves employing both imaging studies and pathological examinations. CT scans serve to pinpoint the disease’s location and assess the degree of its invasion. Furthermore, MRI proves to be a valuable instrument in assessing potential intracranial implications associated with PPF abscesses.
The optimal treatment of PPF abscesses remains inadequately characterized. Conventionally, the recommended approach involves swift surgical drainage and the administration of empirical antibiotics to prevent the abscess from spreading further. Without prompt and efficient management, the infection could potentially extend into the orbit through the inferior orbital fissure, resulting in impaired extraocular muscle function and reduced visual acuity. The retrograde spread of infection along the optic canal or ophthalmic vein carries the potential for severe complications, including cavernous sinus thrombosis, meningitis, cerebritis, brain abscess, or even fatality. Simultaneously, there is a risk of sepsis and septic shock if microorganisms enter the bloodstream. 7 In our case, the patient’s clinical condition continued to deteriorate, with neurological symptoms that included persistent headaches, blepharoptosis, and restricted mouth opening. Given the deep-seated and concealed nature of PPF, intravenous antibiotics, which had been initialed at an external institution, may prove ineffective and could potentially contribute to the further spread of the infection. Consequently, we promptly carried out surgical drainage and debridement of the abscess once the patient’s temperature was partially controlled. Subsequent follow-up demonstrated the effectiveness of our treatment approach, involving abscess drainage through an external cervical approach.
Microbiological analysis of pus and histology identified a massive occurrence of S. constellatus, which belongs to the Streptococcus anginosus group, also known as the Streptococcus milleri group. The flora includes 3 distinct species: S. anginosus, S. intermedius, and S. constellatus. They are considered commensals in the oral flora, but they can also colonize the throat, nasopharynx, digestive tract, and urogenital system, spreading from the oral cavity. The most important clinical feature of S. constellatus is that they have a propensity to gather information about abscesses in different parts, from the teeth to the deep visceral abscesses, especially in the liver and lungs.12 -14 Abscesses have been documented in various anatomical regions, including the reproductive system,15,16 skin, 17 bone, 18 cardiac circulatory system, 19 brain, 20 and head and neck regions, 21 as reported in the literature. However, there have been no prior reports of PPF abscesses attributed to S. constellatus. In this instance, we describe the inaugural case of a PPF abscess linked to S. constellatus in a 43-year-old male patient.
In our case, the patient did not exhibit any clinical symptoms indicative of a primary infection, and the blood microbial culture yielded negative results. No-netheless, considering the prevalence of S. constellatus in the oral cavity and the patient’s history of toothache 6 months prior, even though there was no ongoing toothache at this time, we postulated that the source might be related to the oral cavity. Consequently, a thorough oral examination was conducted by the dentist to investigate this possibility. Regrettably, the dental examination conducted at present did not reveal any discernible abnormalities. In cases where clinicians opt to explore the potential primary source of infection in patients lacking local symptoms, employing dental X-rays to identify potential dental abscesses or cavities, or resorting to more advanced imaging techniques, may prove to be highly advantageous. 22 Consequently, the dentist meticulously examined the patient’s CT imaging results, but these findings did not align with a diagnosis of dental infections. Accordingly, the exact source of the S. constellatus infection in the patient was not a dental infection and remained undetermined.
Conclusions
PPF abscesses are exceedingly rare, but their potential for severe consequences warrants ongoing vigilance. We present the inaugural case of a PPF abscess stemming from S. constellatus infection in the absence of an apparent primary infection source. Diagnosing this condition can pose challenges due to its typically nonspecific symptoms. Therefore, in a patient presenting initially with ptosis, consideration should be given to the possibility of a PPF abscess. While laboratory assessments can guide diagnostic suspicions, imaging, particularly contrast CT, plays a pivotal role in confirming the diagnosis. The optimal management approach for PPF abscesses remains to be definitively established. In our case, once the diagnosis was established, early surgical intervention was promptly employed, followed by appropriate antibiotic therapy. Subsequent follow-up evaluations confirmed the effectiveness of our chosen treatment regimen.
Early clinical suspicion, accurate diagnosis, and effective management of infections can contribute positively to averting the spread of PPF abscesses and the development of life-threatening complications.
Footnotes
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board (or Ethics Committee) of Sir Run Run Shaw Hospital, College of Medicine, Zhejiang University, Hangzhou, Zhejiang, China (protocol code 2023-411-01). The patient and legal guardian consent to the patient’s information being published in this article.