
Abstract
A 30-year-old female patient with no previous chronic illness underwent hemithyroidectomy unusually complaint of ptosis on first postoperative day. On examination, she also had miosis. Thus, diagnosis of Horner’s syndrome was made on ground of ruling out other complication. As it is caused by nerve insult, with a prolonged observation under close follow-up, the patient is fully recovered. Horner’s syndrome after thyroidectomy is a rare entity. In textbook also, it is not mentioned as complication after thyroidectomy.
Introduction
Horner’s syndrome (HS) is a syndrome of ipsilateral ptosis, miosis, facial anhidrosis, and vascular dilatation of one-half of the face. 1 This is first described in humans by Johann Friedrich Horner in 1869. This is caused by the disruption of oculosympathetic pathway (OSP). OSP supplies innervation to the ipsilateral face sweat glands, dilator muscles of the pupil, and retractor muscles of the eyelids.2,3 Most common causes of acquired HS are cerebrovascular accident, neck and mediastinal tumors, neck trauma, and iatrogenic injury after neck and thoracic surgery 1 . HS after thyroidectomy is very rare with only very few cases reported in the literature.1,2,4,5,7 Due to highly variable relationship between cervical sympathetic trunk and thyroid gland, there is very high risk to damage to sympathetic trunk. 5
Case report
A 30-year-old female with presented with progressive enlargement of right-sided neck for years. She had no any signs/symptoms of hyper of hypothyroidism. Her ultrasonography of neck showed TIRADS 6 3 score with a 3 × 2 cm nodule on the right side. Fine needle aspiration cytology showed the Bethesda system for reporting thyroid cytopathology and category IV Follicular Neoplasm. She underwent right hemithyroidectomy with identified and preserved recurrent laryngeal nerve (RLN) and parathyroid. The surgical cavity was thoroughly washed and necessary hemostasis was secured, and the drain of 12 numbers was secured. On the first postoperative day (POD), she complained of ptosis. On examination, she also had miosis and enophthalmos but no anhidrosis or vascular dilatation in the right side of face. So, the diagnosis of HS was made after ruling out other possible complications, such as hematoma and infection. Thus, HS was a result of damage to the cervical sympathetic chain. Her histopathological report turned out to be follicular adenoma with no evidence of malignancy. She was managed conservatively and no steroid given. Her pictures were taken with due consent on different dates as follows. She recovered fully in 8 months (Figure 1).
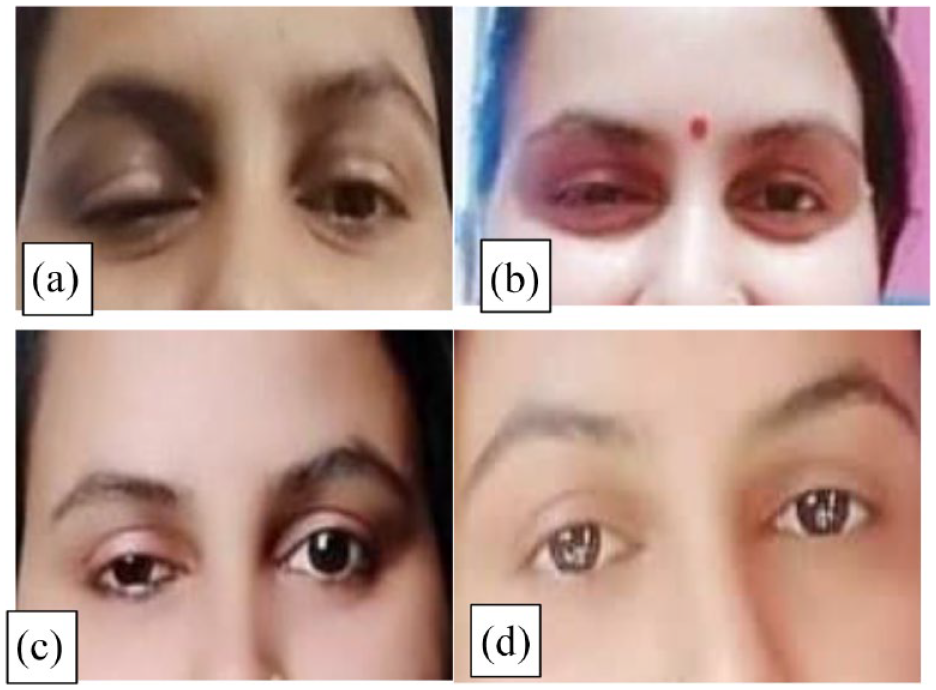
(a) Patient with ptosis of right eye on 1st postoperative day (POD). (b) Patient with gradual improving ptosis of right eye on 1st month POD. (c) Patient with gradual improving ptosis of right eye on 2nd month POD. (d) Patient with fully improved ptosis of right eye on 8th month POD.
Discussion
HS is caused due to injury to the OSP of the cervical sympathetic chain. It was first described in 1853 by Bernard and then in 1869 by Swiss ophthalmologist Johann Horne.4,5 HS presents with miosis and ptosis, enophthalmos of the affected eye, ipsilateral anhidrosis, and vascular dilatation. In some cases, this classic triad is not present.1,7 Interruption of the OSP results in paralysis of the pupillary dilator muscle resulting in miosis. Because of the paresis of the retractor of the upper eyelid, the Mueller’s muscle, ptosis occurs. The vasomotor and sudomotor innervations to the face are interrupted, resulting in unilateral anhidrosis. 1
HS is usually seen when a larger goiter or malignancy of neck causes compression of the cervical sympathetic chain,3,5 but HS as a complication of thyroidectomy is very rare. Iatrogenic causes of HS are major neck surgeries, thoracic surgeries, tube thoracotomy, carotid endarterectomy, etc. 3 The nature of injury determines the prognoses of HS. There were three scenarios, like partially recovered or totally recovered or persistent. 3 Conventional thyroidectomy causing HS is well established; recent reports suggest that HS is also likely to develop after minimal access surgery like minimally invasive parathyoidectommy 8 and minimally invasive video-assisted thyroidectomy. 9
Kappeler was the first to describe HS as a complication of thyroid surgery in 1865, and Kaelin in 1915 published the first case report of HS following thyroidectomy. 10 The possible mechanism causing HS following thyroidectomy is:
The sympathetic chain may get stretched during Lateral retraction. In 1915, de Quervain explained that while retracting carotid sheath laterally, the sympathetic chain might get stretched causing neuropraxia type of injury. 11
Compressed by a hematoma postoperatively.
Ligation of the inferior thyroid artery can cause ischemia-induced damage to neural tissue. Solomon et al. 12 proposed that cervical sympathetic trunk’s vasa nervorum gets its blood supply from the inferior thyroid artery trunk or its branches, and ligation of these vessels may cause ischemia to the sympathetic chain causing HS. Anatomically, the sympathetic truck is very close to the inferior thyroid artery either present in front or behind the inferior thyroid artery. That is why the sympathetic truck is profoundly prone to complications in thyroidectomy.
Communication between sympathetic innervation and RLN may get affected due to its repetitive identification during the procedure.
Cozzaglio et al. 13 described one case (0.2%) of postsurgical HS in a series of 495 thyroidectomies. Ban et al. 14 reported that HS was a rare complication (0.03%) after robotic thyroidectomy for thyroid carcinoma. In a case series by Harding et al., 8 the risk of HS increases with more extensive or complicated thyroid surgery, like thyroid carcinoma with neck dissection and with surgery for goiters with retrosternal extension.
The timing of HS following thyroidectomy has no uniform pattern, and articles showed that most cases have onset between 2nd to 4th postoperative day indicating the possibility of different etiologies,4,5 but the case presented here had onset on 1st POD and features completely relieved after 8 months. This can be explained by injury to the sympathetic chain by retractor stretching and sympathetic regeneration with re-establishment of the original sympathetic pathways after 8 months.1,13 Most cases of HS after thyroidectomy did not have symptoms of ipsilateral facial anhidrosis and cutaneous vascular dilatation. 5 The etiology of this is unclear in many articles and also in this case report.4,5
Conclusion
HS is a rare complication following thyroid surgery. Cautious dissection and good hemostasis, noble traction on retractors, and good anatomical knowledge of the cervical sympathetic chain are mandatory to prevent surgically induced HS.
Surgeons should be aware of the possibility of this syndrome after thyroid surgery as little knowledge may lead to permanent disfigurement of the patient and chances of that spontaneous resolution is high without any treatment.
Footnotes
Acknowledgements
None.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The ethical approval is not required for the case presentation in our institution.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.