
Abstract
Deep neck infections (DNIs) are still emergency conditions in otorhinolaryngology. Due to rapid disease progression and life-threatening complications, the accurate surgical and medical treatment must be promptly applied. In the present study, we analyzed treatment protocols of 46 adults to assess efficacy of the treatment and search for prognostic factors of the outcomes. We performed retrospective analysis of medical data of 46 patients, who underwent surgical treatment in our department due to purulent DNI in the period from 2009 to 2017. Data investigated included age, sex, hospitalization time, duration of symptoms before drainage, comorbidities, selected laboratory tests results, location and the number of abscesses, results of microbiological cultures, and antibiotic treatment options. The study group consisted of 33 (71.7%) men and 13 (28.3%) women. Patients age ranged from 18 to 82 years. The mean duration of hospital stay was 13.2 ± 8.4 days. The most common site involved was submandibular space (43.5%), followed by parapharyngeal space (28.3%). The majority of patients had single abscess (81.2%), the multiple abscesses were revealed in 8 (18.8%) cases. The mean size of the abscesses was 42 mm. C-reactive protein level was increased in 96.7% patients (mean level 155.5 ± 146.7 mg/L), but the white blood cell count exceeded the normal in 60.9% cases (mean level 16.89 ± 5.59 × 109/L). Staphylococcus aureus (20.7%) and Peptostreptococcus (20.7%) were the most common species cultured from swabs. The antibiotic treatment included most commonly a combined ceftriaxone and metronidazole (n = 23). Two patients died due to complications. The correlation between different variables and the duration of hospitalization revealed only the hemoglobin level below 12.5 g/dL, a significant predictor of longer hospitalization (16.23 days vs 12.09 days, P = .017). Patients with purulent DNIs and decreased hemoglobin level are predisposed to prolonged recovery following the surgical drainage.
Introduction
Deep neck infection (DNI) is defined as bacterial infection in the potential spaces and fascial planes of the neck, including submandibular, lateral cervical, visceral, carotid, parapharyngeal, and retropharyngeal spaces. The critical aspect in DNI is the possible obstruction of the airway passage and the rapid spread of the infection continuously from the neck to the mediastinum. The availability of the antibiotics and improved dental care decreased the incidence and mortality due to DNI. However, the DNI is still an emergent condition in otolaryngology, which can lead to serious complications such as airway obstruction, jugular vein thrombosis, carotid artery erosion, cranial nerve paresis, meningitis, mediastinitis, vertebra osteomyelitis, and sepsis. 1 -4 Deep neck infections are usually originating from upper aerodigestive tract diseases, especially tonsillitis and dental infections. In children, the predominant focus of DNI is infection of the tonsils and pharynx, while in adult patients, the increase in the dental etiology is observed. High number of the unknown primary origin of the DNI is an important aspect and, according to the literature, may reach up to 50% of cases. 5 -7 The ultrasonography (US) and computed tomography (CT) of the neck are standard imaging methods to confirm the diagnosis and evaluate the extension of the infection prior to surgical management. 8,9 The treatment plan of DNI includes surgical drainage of the involved space to ensure adequate ventilation and systemic administration of broad-spectrum antibiotics. Usually, the result of microbiological culture proves the presence of mixed flora. Streptococcus is the most commonly isolated pathogen in nondiabetic group and Klebsiella is most common in diabetic patients. 5,10 The unfavorable course of the disease and complications are related to comorbidities such as diabetes, alcohol, or drug abuse. 11 In the present study, we analyzed treatment protocols of 46 adults to assess the effectiveness of the treatment and to identify the prognostic factors that contribute to complications and prolonged hospitalization.
Material and Methods
We performed retrospective analysis of medical records of 46 patients, who underwent surgical treatment in our department, due to purulent DNIs in the period from 2009 to 2017. Patients with superficial skin abscesses, infected lateral cysts, peritonsillar abscesses, epiglottis abscesses, cellulitis, and infected or necrotic head and neck tumors were excluded from the study. The protocol of the study was approved by the local ethical review board.
Data extracted and analyzed include age, sex, hospitalization time, duration of symptoms to drainage, comorbidities, the level of hemoglobin, C-reactive protein (CRP), fibrinogen, white blood cell (WBC) count, location and the number of abscesses, microbiological results, and antibiotic treatment options.
Data were analyzed using GraphPad Prism 5 (GraphPad Software Inc, San Diego, California). For pairwise comparisons, the Mann-Whitney U test or Kruskal-Wallis test with post hoc Dunn test was used. A P value less than .05 was considered statistically significant.
Results
A total of 33 (71.7%) men and 13 (28.3%) women were included in the analysis. Patients age ranged from 18 to 82 years (mean age: 47.4 ± 17.1 years). The major complain was neck swelling (98%) and pain, ipsilateral to the DNI (86.9%; Figure 1).

Neck swelling and skin redness due to purulent infection of deep neck space.
A higher percentage of patients (45.6%) had dysphagia and odynophagia. Trismus was diagnosed in 13% of cases. Fever was the symptom in 41.3% of patients. Four patients had severe dyspnea at the admission. An acute dental inflammation was diagnosed in 14 (30.4%) patients. A history of pharyngitis preceding DNI was found in 12 (26%) patients. Twenty (43.5%) patients had unknown origin of DNI. The CT and US were performed under routine investigation: both methods in 16 patients, only US in 9, and only CT in 21 (Figures 2 and 3).
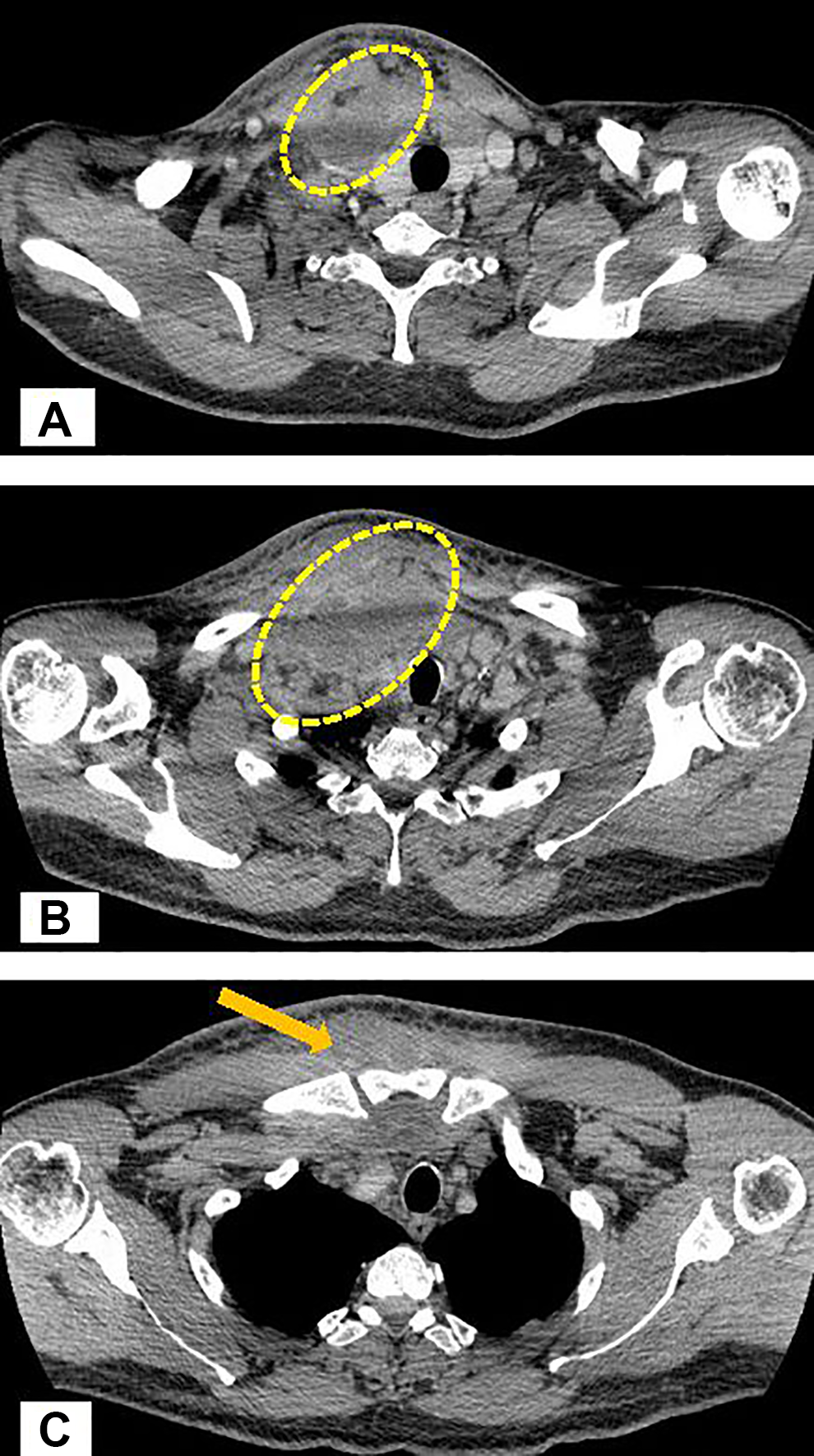
Contrast-enhanced computed tomography (CT) revealed massive edema of neck tissues due to inflammatory process, upper edge of the inflammation localized at the level of facial vein descending to the jugular notch of the sternum. Larynx and trachea pushed to the left. Thrombosis of the jugular vein at the level of inflammation. A and B, Deep neck tissue abscess marked on CT images lateral to trachea. C, Tissues edema anterior to sternum (marked with arrow).
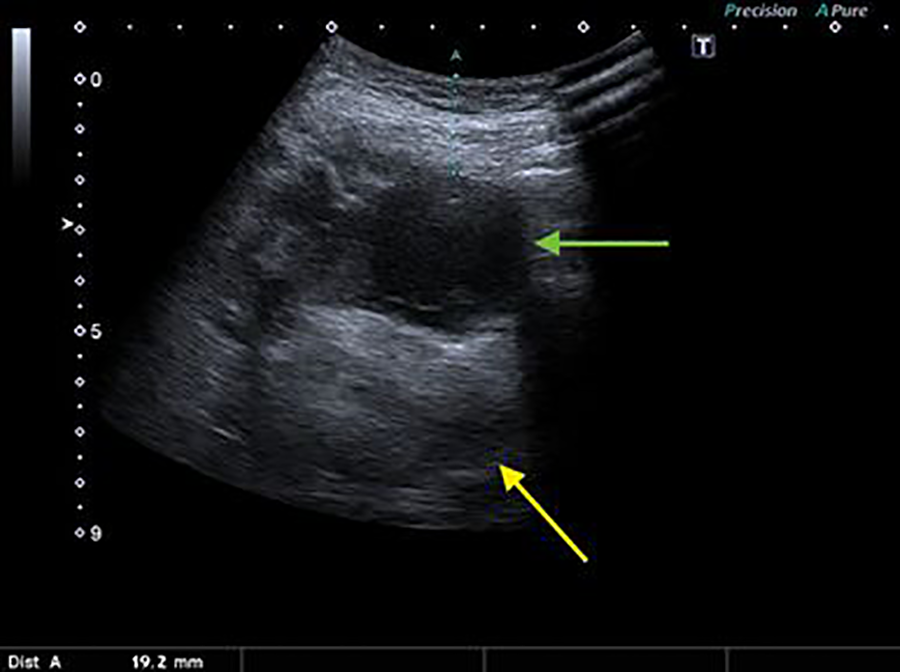
Ultrasound image of submandibular space abscess visible heterogeneous, hypoechoic lesion at a depth of 20 mm (green arrow) displacing submandibular gland due to mass effect (yellow arrow).
The most common site involved was submandibular space (20/46), followed by parapharyngeal space (13/46) and carotid space (9/46). The abscesses were more common on the left side of the neck (57.8%). The majority (81.2%) of patients had single abscess, multiple abscesses were revealed in 8 (18.8%) cases. The mean dimensions of abscesses were 35.2 ± 37.5 mm × 40.4 ± 89.5 mm, ranging from 10 to 130 mm. Blood tests revealed increased levels of CRP in 96.7% of patients, with the mean level of 155.5 ± 146.7 mg/L (range: 1-478 mg/L). Reference number of WBC count (normal range: 4-8 × 109/L) was increased in 60.9% of patients, with a mean count of 16.89 ± 5.59 × 109/L (range: 7-170 × 109/L). The mean hemoglobin level was 11.5 ± 3.9 g/dL, ranging from 8.3 to 15.2 g/dL. The mean fibrinogen level was 487.8 ± 742.7 mg/dL (range: 149-1294 mg/dL; Table 1).
Correlation of Different Variables With the Duration of Hospitalization in the Study Population.a
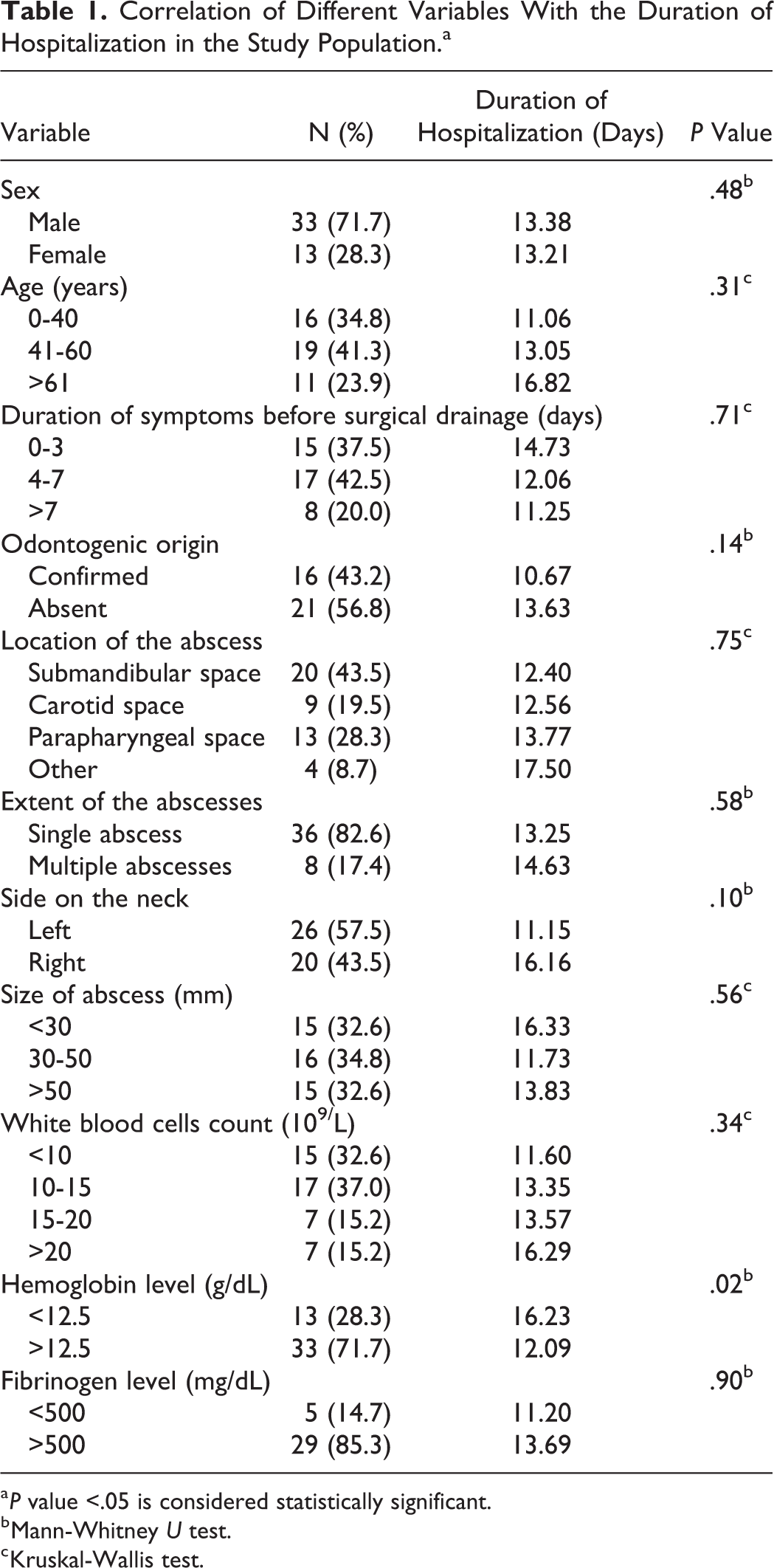
a P value <.05 is considered statistically significant.
b Mann-Whitney U test.
c Kruskal-Wallis test.
All patients underwent a surgical drainage of the neck abscess under general anesthesia. During the procedure, a silicone drains were inserted into the wound to allow later abscess rinsing with local disinfectants twice a day (Figure 4).
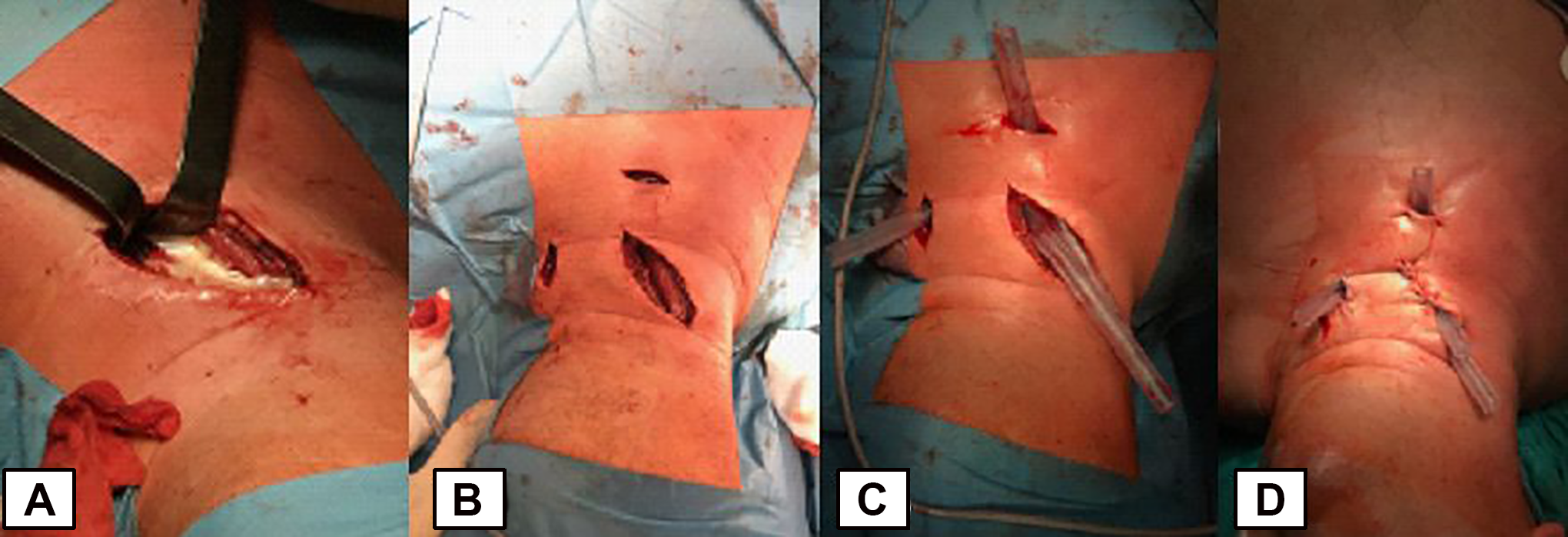
Steps of surgical drainage of cervical abscess. A, Vertical incision medial to the sternocleidomastoid muscle and drainage of abscess with pus evacuation. B, Central vertical and additional lateral incision for placement of rinsing drains. C, Intraoperative rinsing drains placement. D, Drains localization after skin suturing.
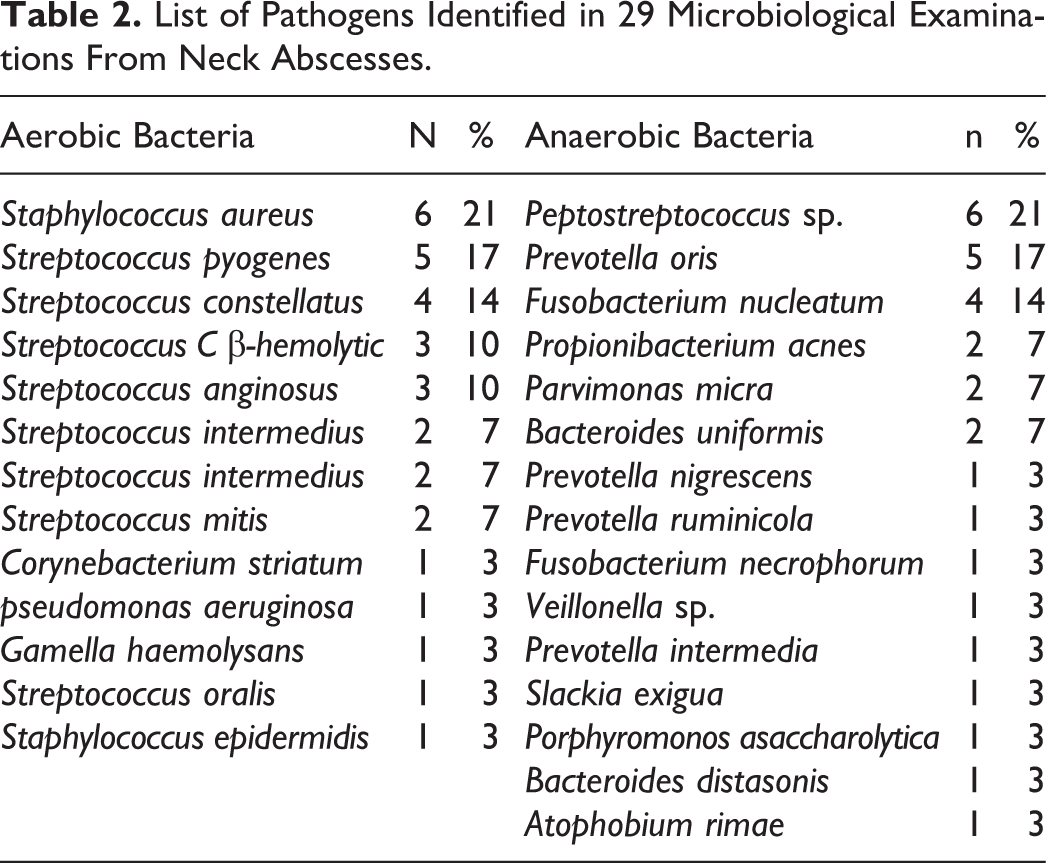
Drains were removed after 2 days, with no purulent content found during rinsing. The patients were discharged 2 days after the removal of drains. In 2 cases, there was a second revision operation necessary with redrain, due to the reoccurrence of the symptoms post drainage removal and radiological confirmation of reformation of the abscess. Both reoperated patients had primary multiple space process. The mean hospital stay was 13.2 ± 8.4 days. The material for microbiological culture was collected during surgical drainage in 29 (63%) patients. The aerobic bacteria were isolated in 13 cases, anaerobic in 4, and the mixed flora in 12 patients. Staphylococcus aureus (n = 6) was the most commonly isolated aerobic bacteria and Peptostreptococcus sp. (n = 6) were the most common anaerobic bacteria. The results of bacterial cultures were polymicrobial in 16 patients. Overall, 28 different pathogens were isolated (Table 2).
List of Pathogens Identified in 29 Microbiological Examinations From Neck Abscesses.
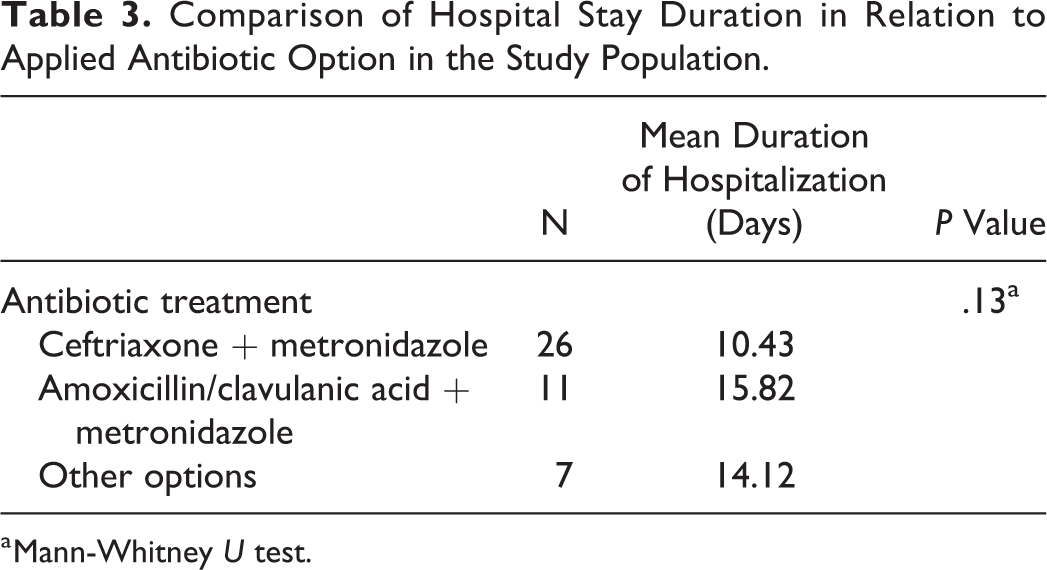
All patients were treated with broad-spectrum intravenous antibiotics. The most commonly used empirical antibiotic therapy option was a combination of ceftriaxone and metronidazole (n = 23). Amoxicillin/clavulanic acid combined with metronidazole was used less often (n = 11). The other treatment options included clindamycin or amoxicillin/clavulanic acid. Neither of these therapeutic options proved to significantly reduce hospital stay; however, patients treated with combined ceftriaxone and metronidazole were hospitalized for 10.43 days and those treated with combined amoxicillin/clavulanic acid and metronidazole for 15.82 days. The correlation result between antibiotic therapy options and hospitalization period is presented in Table 3.
Comparison of Hospital Stay Duration in Relation to Applied Antibiotic Option in the Study Population.
a Mann-Whitney U test.
The major comorbidities in our group were cardiovascular diseases (8/46). Only 2 diabetic patients were present. Two (4.3%) patients died during hospitalization due to mediastinitis and sepsis. Patients who died despite treatment were malnourished at the admission, the one had mental disorders and the other was homeless. The sign of the upper and lower mediastinitis was demonstrated in CT scan performed on the fourth day after neck drainage due to reported thoracic pain. The patient underwent thoracic surgery for drainage, complicated with sudden cardiac arrest with ineffective resuscitation. In the second lethal case, although the sensitive antibiotics were administered after neck drainage, deterioration in general condition of the patient was observed with continuous decrease in blood pressure, diuresis, and oxygen saturation. The patient was transferred to the intensive care unit; however, due to multiple-organ dysfunction and disseminated intravascular coagulation, the treatment measures were found to be ineffective. This patient had also history of hematological treatment 5 years ago due to chronic myeloid leukemia and was observed in remission.
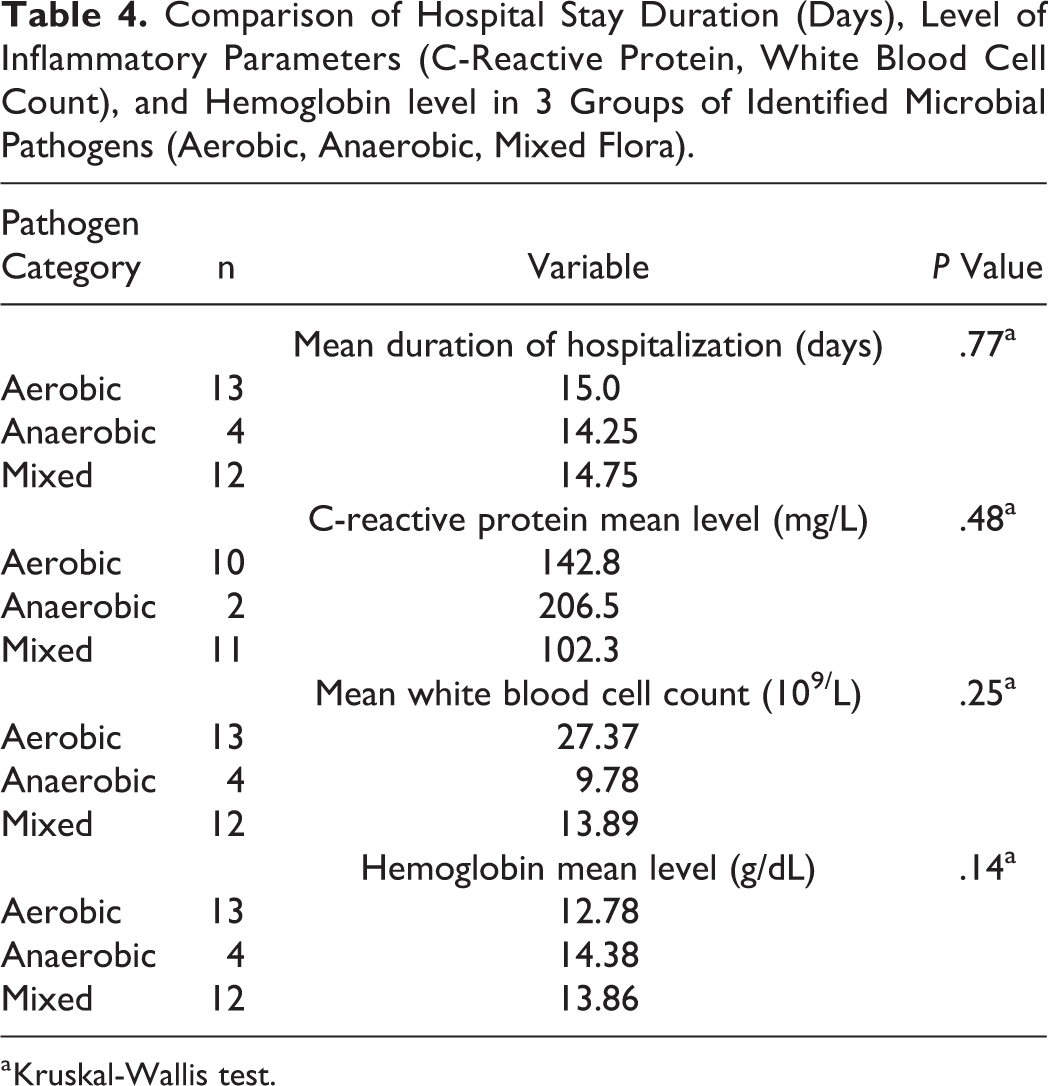
Statistical analysis of variables such as sex, age, dental diseases, location, size, side of abscess, CRP level, hemoglobin level, WBC count, fibrinogen level, the bacterial etiology, and the duration of hospitalization was performed. Table 4 shows that only patients with hemoglobin level below 12.5 g/dL were hospitalized significantly longer (16.23 days vs 12.09 days, P = .02).
Comparison of Hospital Stay Duration (Days), Level of Inflammatory Parameters (C-Reactive Protein, White Blood Cell Count), and Hemoglobin level in 3 Groups of Identified Microbial Pathogens (Aerobic, Anaerobic, Mixed Flora).
a Kruskal-Wallis test.
Discussion
Deep neck infection seems to be a well-studied issue in otolaryngological practice, but it is still a serious life-threatening disease. Thanks to wide availability of antibiotics that the incidence is much lower than 30 years ago and the treatment results more predictable and controlled. The important aspect is to identify factors that may influence the course of treatment and therefore give some indications for optional or supplementary therapy.
According to the literature, DNI in adult patients moderately predominate in men, with the highest incidence ranging from 40 to 60 years. 12,13 The most common location of DNI is not defined, due to different eligibility criteria in published researches. Some authors present the data such as the peritonsillar abscesses that are of high incidence, but generally not recognized as infection of deep space. The submandibular space is the most commonly identified location of DNI, followed by parapharyngeal space. 12,14,15 These locations predominated in our study group; however, we did not found the difference between the duration of hospitalization and different abscess site. Some authors report that the multiple spaces involved in DNI are prognostic factors for increased complication rate, but not for the long-term hospitalization. 16 In our population, we also did not observe significantly longer hospitalization among 8 patients with more than 1 space involved. The precise identification of the inflammatory process cause may be difficult in some cases due to previous antibiotic treatment and delayed occurrence of DNI. However, the majority of studies confirm odontogenic disease as a most common cause of DNI in adult patients. 7,17 -19 There is an agreement among authors concerning the increasing rate of unknown primary origin of DNI that stands for 16% to 50% of cases. 6,7,16,17 In our study, the patients with confirmed tooth decay have 43.2% of cases and their hospitalization stay was compared to those with other causes of DNI. On the contrary, Staffieri et al found that DNI with odontogenic origin had significantly shorter hospitalization; however, the complication rate did not differ among study groups. 16 Interestingly, the duration of symptoms before admission and therefore the delay in surgical drainage did not correlate in our patients with the final hospitalization period. It is also surprising that the level of inflammatory proteins (CRP, fibrinogen) and the WBC count had insignificant influence on the hospital stay duration in our population with DNI. The multivariate analysis by Staffieri et al found the leukocyte count over 11 × 109/L, a significant predictor of prolonged hospitalization; however, not indicating increased complication rates. 16 The authors did not analyze the level of hemoglobin in their population. The level lower than 12.5 g/dL occurred prognostic variable of prolonged hospitalization in our patients. Regarding the microbial etiology, most of the authors confirm the staphylococci and streptococci as the most frequently isolated pathogens; however, polymicrobial cultures are very common. 7 -14,16 According to the literature, even 14% to 20% of cultures form DNI are negative, which is connected most probably with antibiotic administration prior to surgical drainage. The aerobic, anaerobic, or mixed category of pathogens did not correlate with prolonged hospitalization in our study group. The presence of comorbidities in patients with DNI, especially the diabetes, is regarded as unfavorable predictor of complications and prolonged hospitalization quoted by many authors. However, the multivariate analysis by Staffieri et al found comorbidities significant factor for prolonged hospital stay, but not increasing the complication rate. The malnutrition and poor socioeconomic status are also considered negative predictors of complications. In our population with DNI, the incidence of diabetes and other comorbidities was quite low and insignificant. However, both lethal complications (mediastinitis and sepsis) occurred in malnourished patients, the one with mental disorders and the other homeless.
Both US and/or CT imaging are helpful to differentiate between the abscess and cellulitis and to take decision about possible treatment options. Computed tomography has advantages over US in visualization of exact extension of inflammation, diagnosis of parapharyngeal space abscesses, and identification of complications. The widely accepted therapeutic method in neck abscesses is surgical drainage of pus from external incisions combined with empirical, broad-spectrum intravenous antibiotic. The first-line treatment recommended is amoxicillin with clavulanic acid or other β-lactam–resistant antibiotic combined with a drug of high efficacy against anaerobes (such as metronidazole and clindamycin). 5,7 Rare practice is conservative treatment with intravenous antibiotics combined with CT-based monitoring. However, Boscolo-Rizzo et al presented successful therapeutic results of such approach in 226 of 365 adult patients with DNI. 13 Another custom method is US-guided drainage of deep neck space abscesses. Several authors recommend US-guided technique as an effective, less invasive, and cost-effective procedure; however, we do not have experience with the method. 20,21
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.