
Abstract
Objectives
Descending necrotizing mediastinitis (DNM) developing after deep neck infection (DNI) is a potentially lethal disease of the mediastinum with a mortality rate as high as 40% prior to the 1990s. No standard treatment protocol is available. Here, we present the outcomes of our multidisciplinary approaches for treating DNM originating from a DNI.
Methods
Between June 2016 and July 2021, there were 390 patients with DNIs admitting to our tertiary hospital. A total 21 patients with DNIs complicated with DNM were enrolled. The multidisciplinary approaches included establishment of airway security, appropriate surgery and antibiotics, extracorporeal membrane oxygenation, and intensive care unit management. The clinical variables were analyzed.
Results
Two patients died and 19 survived (mortality 9.5%). The patients who died had a higher mean C-reactive protein (CRP) level than did those who survived (420.0 ± 110.3 vs 221.8 ± 100.6 mg/L) (P = .038). The most common pathogens were Streptococcus constellatus and Streptococcus anginosus. From 2001 to 2021, the average mortality rate of studies enrolling more than 10 patients was 16.1%.
Conclusion
Multidisciplinary approaches, early comprehensive medical treatment, and co-ordination among departments significantly reduce mortality. Patients with severe inflammation and high CRP levels require intensive and aggressive interventions.
Keywords
Introduction
Descending necrotizing mediastinitis (DNM) is a severe-to-fatal infectious disease of the mediastinum in which a deep neck infection (DNI) spreads along the cervical fascia and the neck spaces and then down to the mediastinum. 1 -3 DNM is often fatal; this is usually a complication of an odontogenic infection or a peritonsillar abscess. 4 -6 Management is difficult, with delayed diagnosis and incomplete mediastinal drainage causing most deaths. 7,8 The mortality rate was as high as 40% prior to the 1990s. 3,9 No standard treatment protocol has yet been established because the causes and locations of infection vary widely. 10
However, based on our experience and reports published over the past 20 years, we considered that the mortality rate may have fallen. Here, we explore that possibility, and describe our multidisciplinary approaches toward treatment of DNM arising from a DNI.
Materials and Methods
We retrospectively reviewed the medical records of 390 patients with DNIs and 21 consecutive patients with both DNIs and DNM admitted to Chang Gung Memorial Hospital, Linkou, Taiwan, between June 2016 and July 2021. Diagnostic imaging based on computed tomography with or without ultrasonography (US) was performed.
We applied the diagnostic criteria for DNM as (1) clinical evidence of severe oral/oropharyngeal infection; (2) establishment of the relationship between DNM and the oral/oropharyngeal process; (3) characteristic radiographic features of mediastinitis. 11,12
Treatments included antibiotics, US-guided needle drainage, and open-surgery incision and drainage. The broad-spectrum antibiotics ceftriaxon (1 g Q12H) and metronidazole (500 mg Q8H) were prescribed as empirical therapy for aerobic and anaerobic bacteria before culture results were available. The antibiotics were modified based on the culture data.
The treatment unit included an otorhinolaryngologist, a thoracic surgeon, a radiologist, an infectious disease physician, an intensive care unit (ICU) team, and an anesthesiologist.
We utilized the classification of Endo et al 13 for DNM as Type I: DNM is localized in the upper mediastinum above the tracheal bifurcation; Type IIA: DNM extends to the lower anterior mediastinum; Type IIB: DNM extends to the anterior and lower posterior mediastinum.
The surgical procedures included tracheostomy and cervical surgery with or without mediastinal drainage performed by an otorhinolaryngological and/or thoracic surgical team according to the classification of Endo et al. Repeat surgery was considered if a residual abscess, necrotic tissue, or unsatisfactory drainage was evident 2 to 3 days after primary surgery. If the infection was controlled, and circulatory and/or respiratory assistance was no longer needed, the patient was transferred from the ICU to a general ward. The flow chart of management algorithm was shown as Figure 1. The flow chart of management algorithm.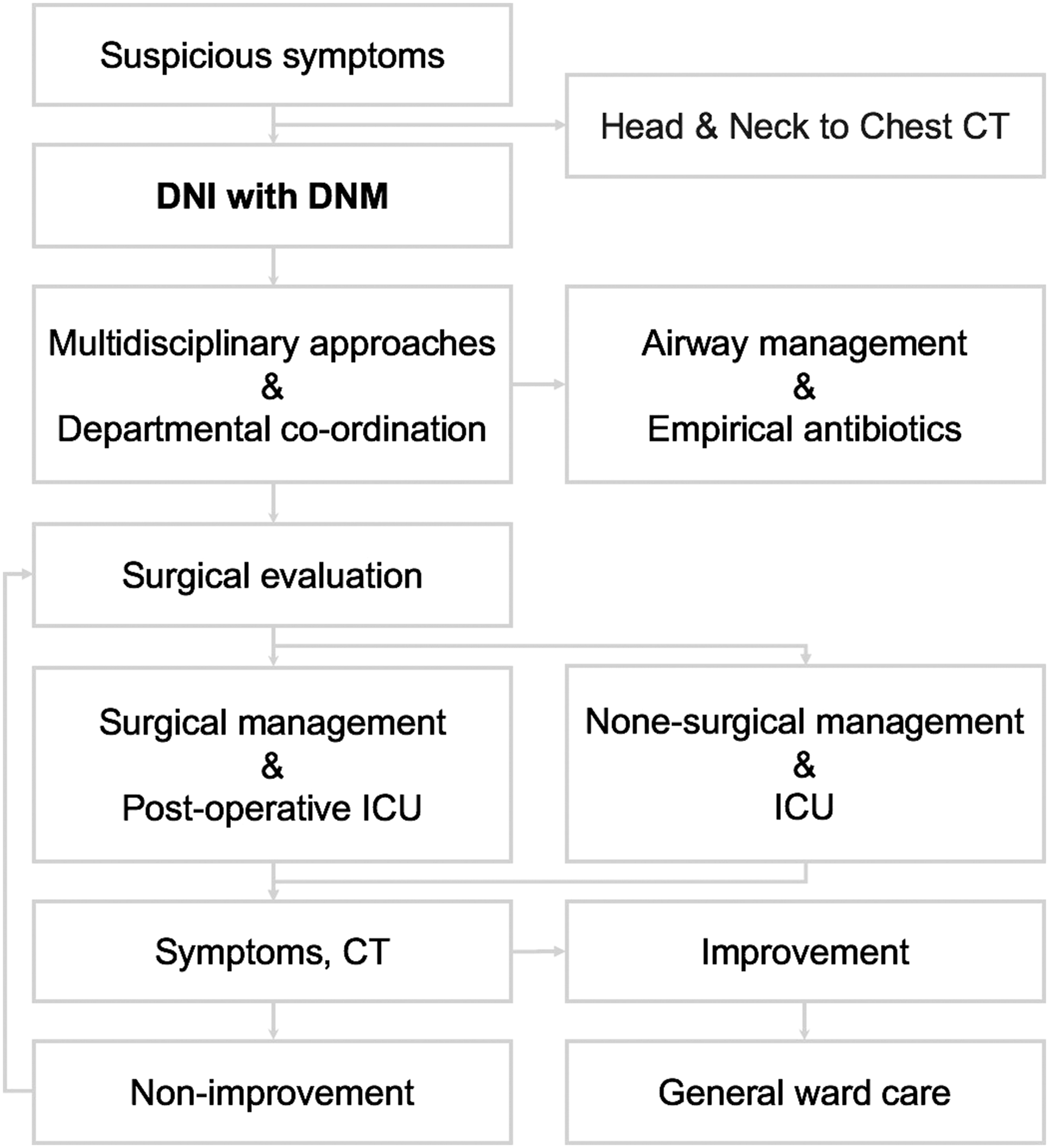
We recorded the patient age (range 2–86 years), duration of illness (range 1–14 days), length of hospital stay (range 2–86 days), intubation period (range 0–26 days), length of ICU stay (range 0–44 days), white blood cell (WBC) count (range 5200–32900/μL), C-reactive protein (CRP) level (range 2.7–480 mg/L), blood sugar level (range 103–522 mg/dL), diabetes mellitus (DM) status, number of involved deep neck spaces, US-guided drainage status, surgical incision and drainage status, tracheostomy and mediastinotomy status, use of extracorporeal membrane oxygenation (ECMO), morbidities, and mortality. Categorical variables are presented as proportions and continuous variables as means ± standard deviations. Specimens for bacterial culture were obtained during surgery or by drawing blood.
Exclusion Criteria
We identified 28 patients with DNIs complicated by DNM. However, those with a pneumomediastinum, trauma-related mediastinal perforations, or a history of head-and-neck cancer and those who were immunocompromised were excluded. Finally, 21 patients were enrolled.
Statistical Analysis
All data were analyzed using MedCalc software (ver. 18.6; MedCalc, Ostend, Belgium). The Kolmogorov–Smirnov test revealed that the data were not normally distributed. We thus used Fisher’s exact test to compare categorical variables and the Mann–Whitney U test to compare continuous variables. A P-value < .05 was considered to reflect statistical significance.
Results
Clinicopathological characteristics of 21 patients with DNIs complicated with DNM.
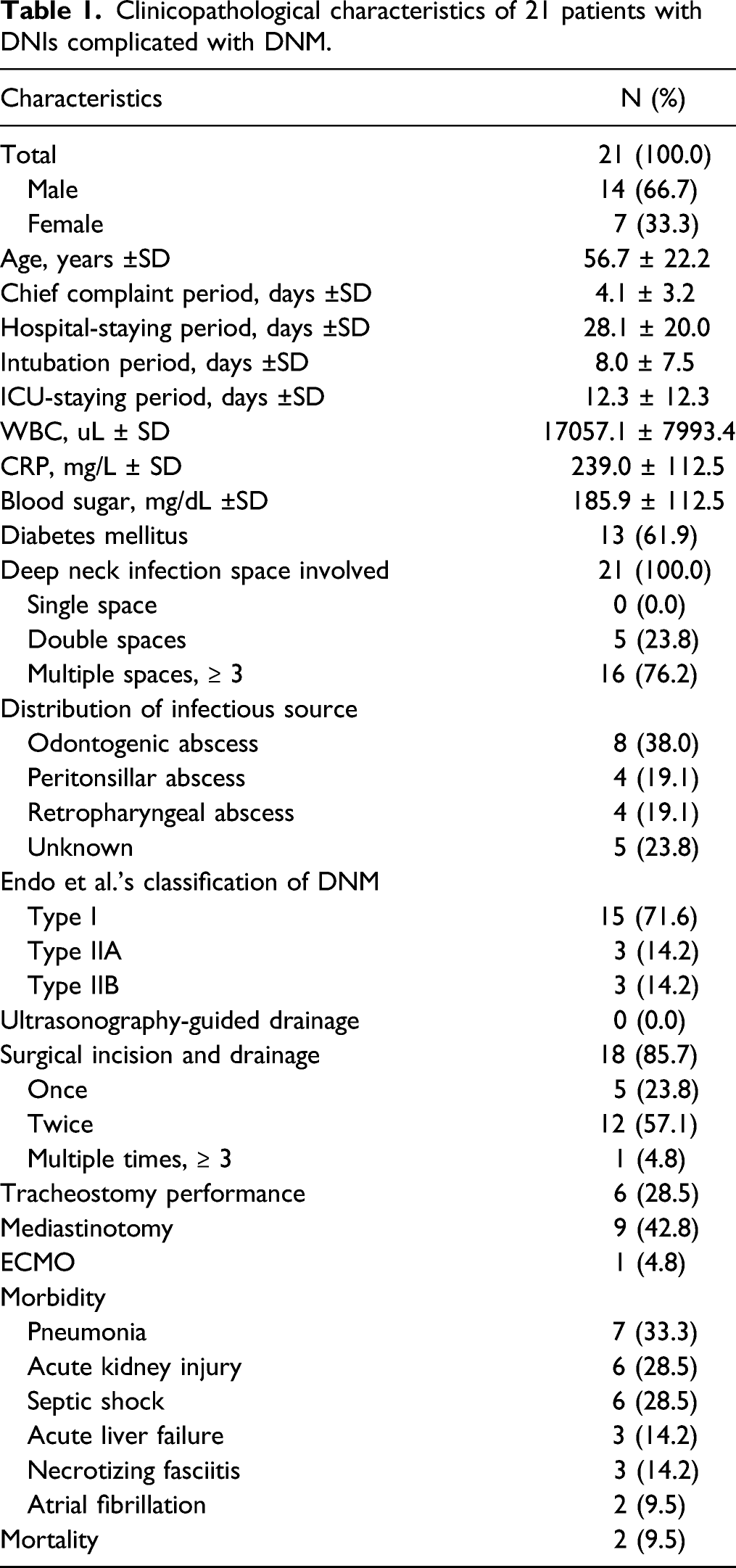
In terms of treatment, no patient (0%) underwent US-guided drainage, but 18 (85.7%) required surgical drainage. Of these, 5 (23.8%) underwent open surgical incision and drainage once, 12 (57.1%) underwent such treatment twice, and 1 (4.8%) underwent such treatment 3 times. Tracheostomy was performed for 6 patients (28.5%) and mediastinotomy for 9 (42.8%). One patient (4.8%) required ECMO during surgery. No intraoperative or immediate postoperative death was recorded.
In terms of morbidities, pneumonia developed in 7 patients (33.3%), acute kidney injury in 6 (28.5%), septic shock in 6 (28.5%), acute liver failure in 3 (14.2%), necrotizing fasciitis in 3 (14.2%), and atrial fibrillation in 2 (9.5%). Two patients died and 19 survived (mortality rate 9.5%).
The comparison between survival group and mortality group.
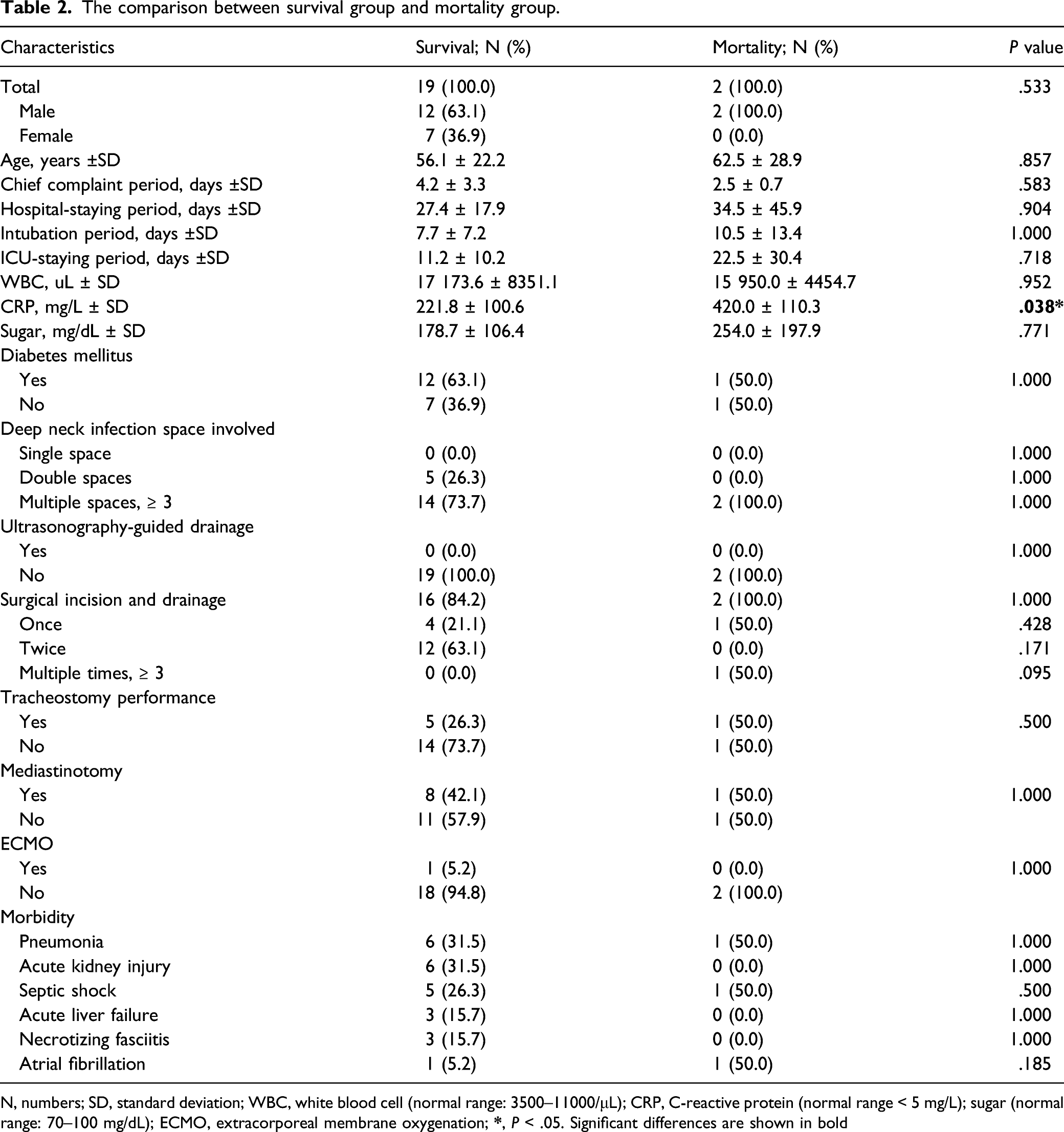
N, numbers; SD, standard deviation; WBC, white blood cell (normal range: 3500–11000/μL); CRP, C-reactive protein (normal range < 5 mg/L); sugar (normal range: 70–100 mg/dL); ECMO, extracorporeal membrane oxygenation;
Analysis of pathogens in 21 patients with DNIs complicated with DNM.
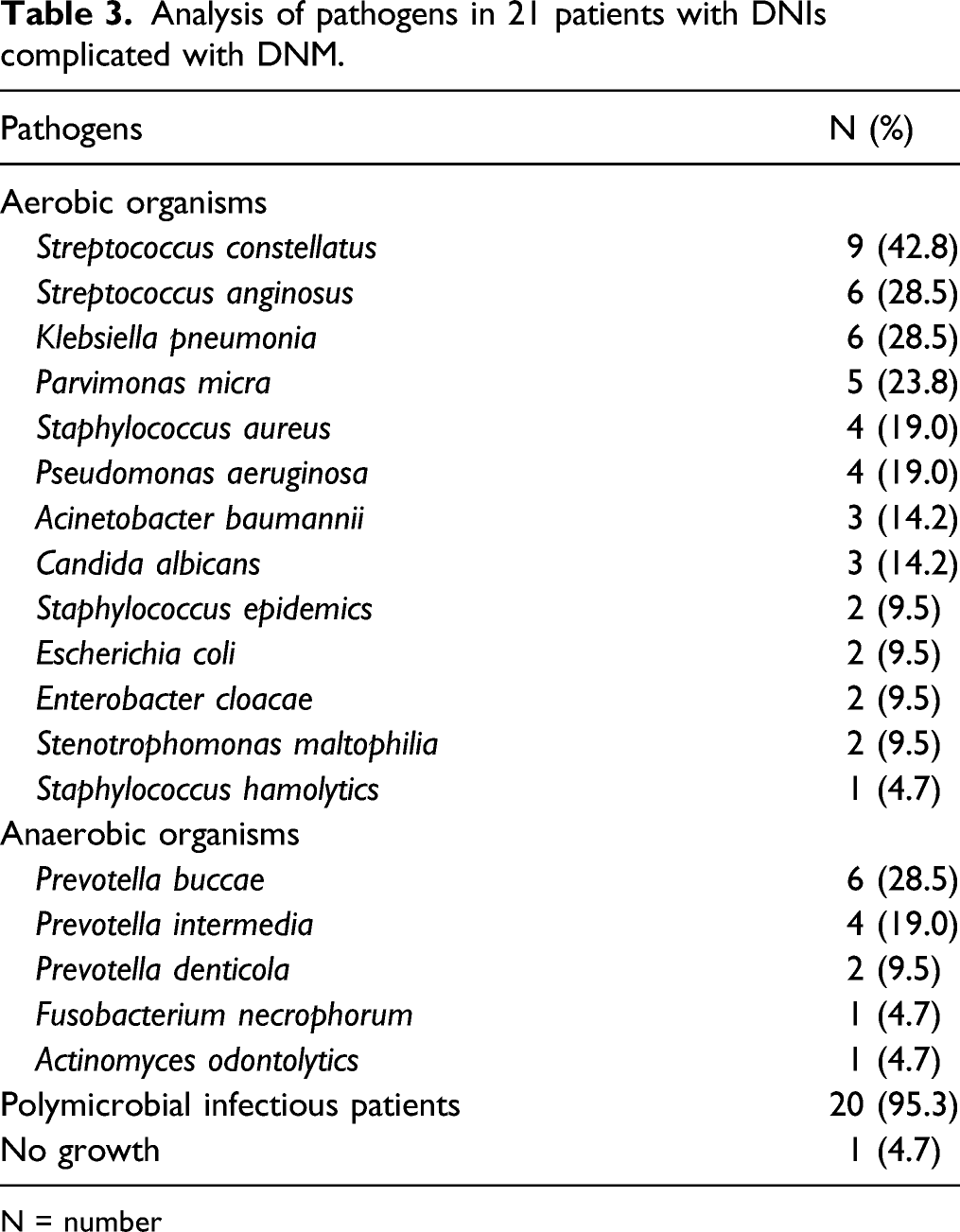
N = number
Studies with at least 10 patients enrolled with DNIs complicated with DNM.
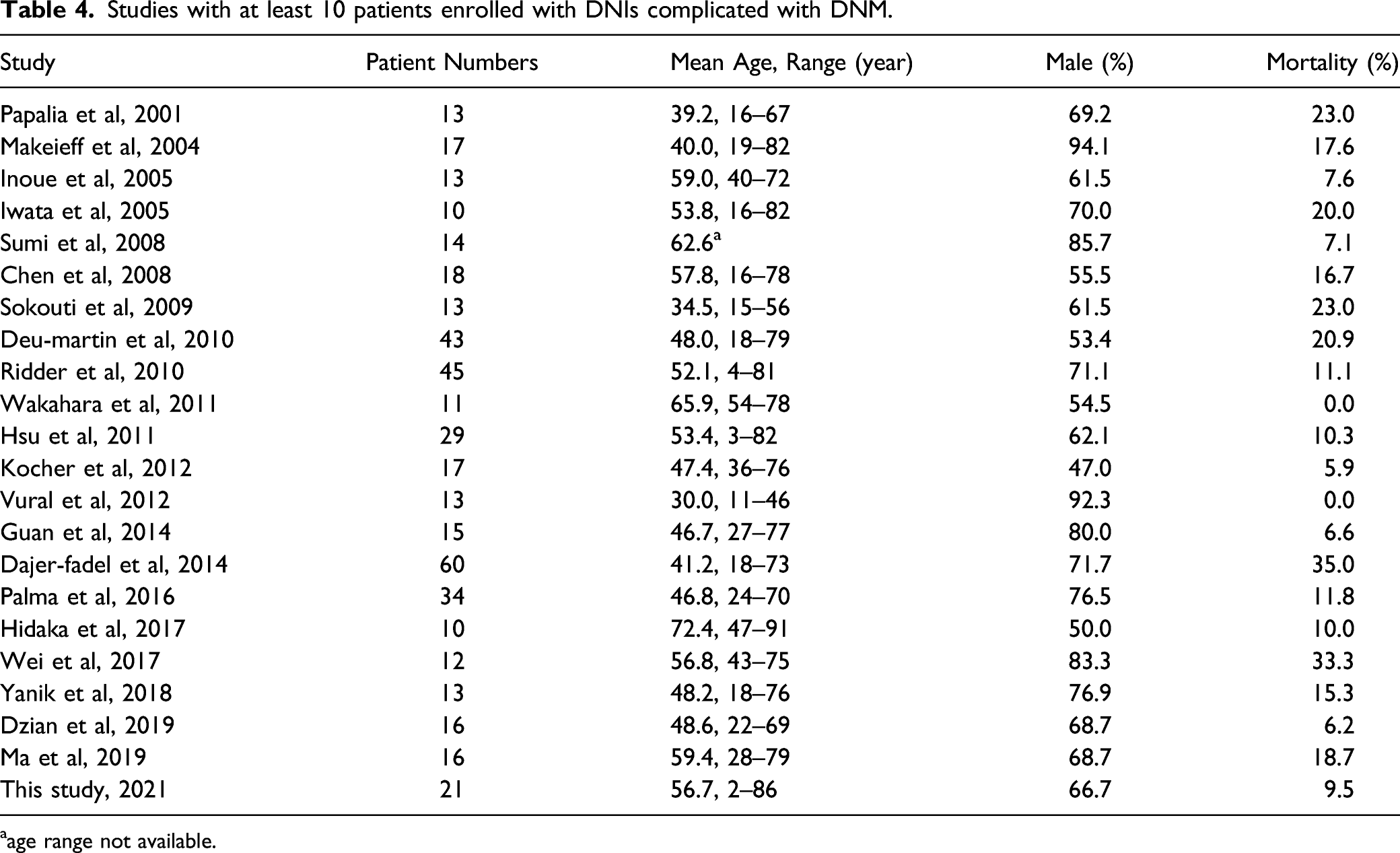
aage range not available.
Discussion
Descending necrotizing mediastinitis is a severe soft tissue infection of the interpleural spaces and central thoracic organs, 14 in which an oropharyngeal infection progresses to the cervical region and spreads along the fascia to the mediastinum. The infection exploits the regional anatomical continuity between the cervical spaces and the mediastinum, as well as the effects of gravity and negative intrathoracic pressure during inspiration. 4,15,16 The most fatal form of mediastinal infection is DNM, which was well defined by Estrera et al. with the definition later refined by Wheatley et al. 11,17,18 The DNM rate associated with DNI is 1.7% to 5.4%. 19,20 Our rate was 5.3% (21 of 390 patients). DNI aside, DNM is also caused by infection after sternotomy during cardiac operations or esophageal perforations. We explored the clinical manifestations of 21 patients and compared these to those reported previously, finding that it is critical to deliver appropriate treatment when patients present with this life-threatening condition.
Table 1 shows that male patients predominated (66.7%; females 33.3%). Most patients were middle-aged (56.7 ± 22.2 years) as in previous studies. 18 CRP, synthesized principally by liver hepatocytes, but also by smooth muscle cells, macrophages, endothelial cells, lymphocytes, and adipocytes, serves as a marker of acute inflammation; the level thereof is elevated by pro-inflammatory cytokines. 21 Wang et al. 22 found that DNI patients with CRP levels >100 mg/L required longer hospital stays (P = .002). The CRP level predicts DNI progression to DNM. Kimura et al. 1 sought clinical predictors of DNM developing secondarily to DNI; a CRP level ≥30 mg/dL (thus ≥300 mg/L in the present study) was a risk factor. Inshinaga et al. found that DNM was associated with a higher CRP level than was DNI without mediastinitis (P < .005). 10 Table 2 shows that in the survival group, the average CRP level was 221.8 ± 100.6 mg/L, whereas that in the mortality group was 420.0 ± 110.3 mg/L (P = .038). Therefore, the CRP level reflects both the severity of inflammation and disease prognosis.
Descending necrotizing mediastinitis is primarily treated via airway management, intravenous broad-spectrum antibiotics, and surgical drainage of the neck and mediastinum. 18 Table 1 shows that most patients underwent surgery (85.7%), most commonly, two surgeries (57.1%), consistent with the data of Inshinaga et al. 10 Our patients underwent a mean of 1.5 (range 1–3) open surgeries during hospitalization, whereas Hsu et al. 15 reported a figure of 2.1 (range 1–5). The surgical treatments included cervical mediastinal drainage without opening of the chest cavity and combined transcervical and transthoracic mediastinotomy drainage. Several approaches toward transthoracic mediastinal drainage have been described, including subxiphoid and median sternotomy, posterolateral thoracotomy, clamshell incision, and video-assisted thoracic surgery (VATS); however, the optimal treatment remains unclear. 10,15,18,23 Hsu et al. considered that transcervical mediastinal drainage may be sufficient, especially when a thoracic surgeon is not available 15 ; Yanik et al. 4 were of the view that the combination of cervical mediastinal drainage and minimally invasive VATS thoracostomy is optimal. However, less-extensive surgical approaches were associated with unsatisfactory outcomes and high re-operation rates. 24 Eighteen of our patients underwent transcervical (surgical) open drainage (85.7%), accompanied by transthoracic mediastinotomy in nine (42.8%).
Our principles for clinical decisions of the patients undergoing surgical drainage twice or multiple times were based on the points: After the first surgery, the patient’s clinical condition did not improve, or they had progression of symptoms such as persistent redness and swelling of neck, hypotension, tachycardia, tachypnea and dyspnea, or the followed CT showed no improvement after operations and there were residual or recurrent abscess formation. For such patients, we performed the surgical drainage again. In addition, there are several vital organs around mediastinum. Therefore, the small abscesses caused by DNM were difficult to drain, which resulted in the need for repeated surgical drainage. To reduce the times of surgeries and length of hospital stay, we believe that accurate imaging interpretation before surgery, appropriate drainage of each abscess, and the reliable cultures of pathogens cultures are beneficial. Furthermore, choosing the proper antibiotics for targeting specific cultured pathogens can also shorten the course of treatment.
The extent of DNM was scored as suggested by Endo et al. 13 Surgery seeks to completely drain the abscess, and this thus dictates the extent of surgery. Transcervical mediastinal drainage is sufficient if the abscess is limited to the upper part of the mediastinum (above the tracheal bifurcation) (Endo type I). However, abscesses of Endo type IIA (extending to the lower anterior mediastinum) or IIB (extending to the anterior and lower posterior mediastinum) generally require a subxiphoid approach or midline sternotomy, or posterolateral thoracotomy, respectively. 18 Surgical management must be tailored to the condition of each patient.
Our tracheostomy rate was 28.5% (Table 1). Tracheostomy for patients with a DNI and DNM remains controversial. 18 Some clinicians consider that tracheostomy is necessary to avoid difficult intubation and the risk of aspiration, whereas others are of the view that tracheostomy may increase the risk of contamination of the pretracheal space, act as an source of downward infectious spread, and aggravate any subsequent mediastinal infection. 17,25 Wolfe et al. 26 opined that tracheostomy should not be routine for patients with a DNI and compromised airway.
We performed tracheostomy when we considered that intubation might be impossible or prolonged hospitalization might be required.
2,4,18
As shown in Figure 2, one DNI patient with DNM had an abscess that compressed the trachea back to the level of the esophagus. We thus performed tracheostomy to secure the airway. In a patient with a DNI and mediastinitis, an abscess (arrowhead) had compressed the trachea (arrow) back to the level of the esophagus. The sternal notch is indicated (asterisk).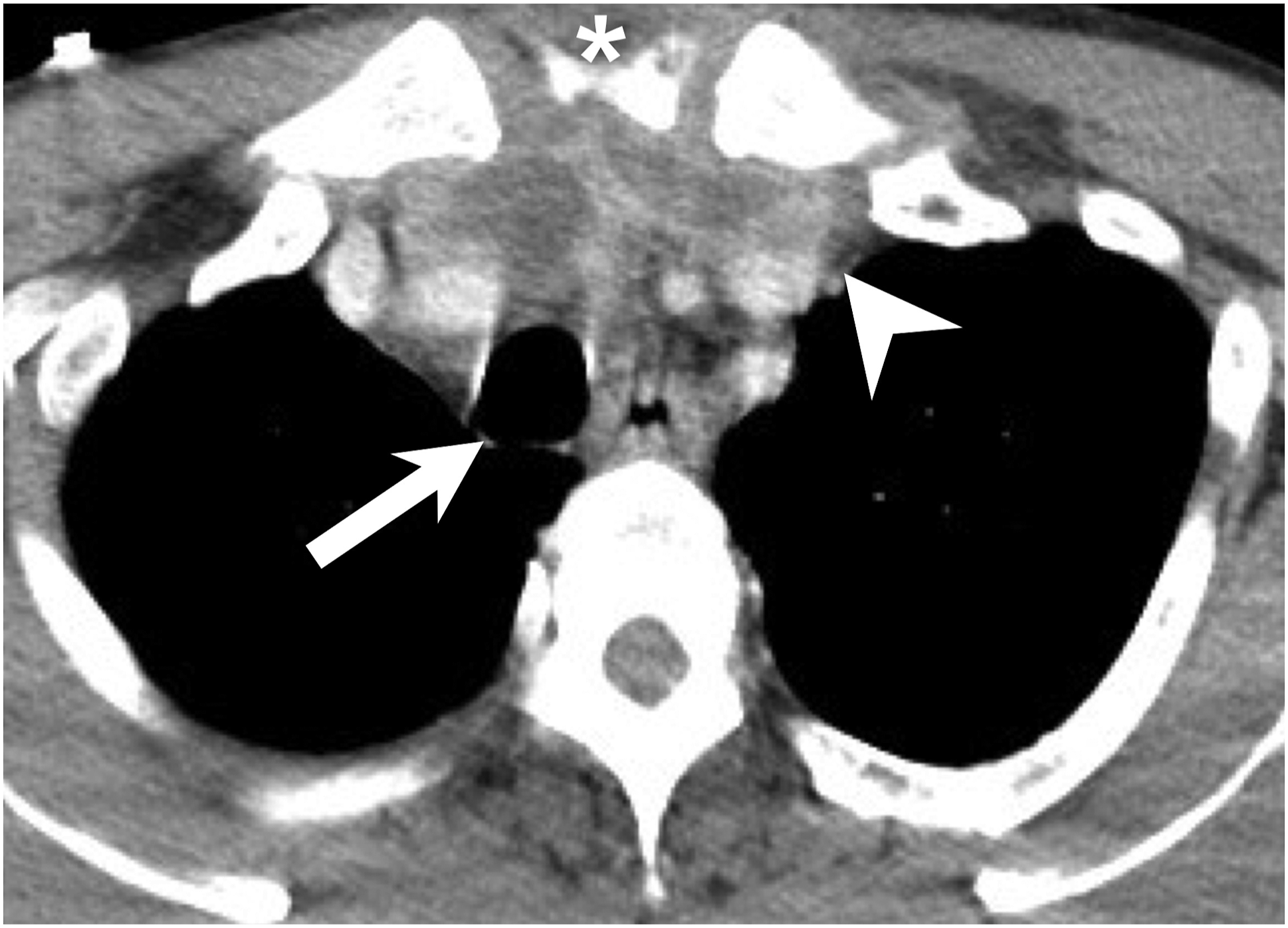
Table 3 shows that most patients (95.3%) were infected with several aerobes and anaerobes. No bacterial growth was observed in only one patient (4.7%), possibly attributable to isolation failure or the pre-isolation antibiotic regime. The initial empirical antibiotic treatment for DNM (which we adopted) is third-generation cefalosporin (ceftriaxon) combined with metronidazole. 27 Other broad-spectrum antibiotics such as ertapenem, carbapenems (imipenem, meropenem), and/or acylaminopenicilin with a β-lactam inhibitor or piperacilin/tazobactam can also be given initially if they are available. 9
Pneumonia was the most common morbidity (33.3%), followed by acute kidney injury (28.5%), septic shock (28.5%), acute liver failure (14.2%), cervical necrotizing fasciitis (14.2%), and atrial fibrillation (9.5%). ICU care, morbidity management, and interventional therapies were all required. One patient required ECMO because refractory septic shock developed during surgical drainage. Although the patient survived, Huang et al. 28 reported unsatisfactory ECMO outcomes for patients with septic shock refractory to medical treatment.
Descending necrotizing mediastinitis is associated with high rates of mortality. Wheatley et al. reported that the mortality rate in 1960–1989 was 34.9%, when surgery was less radical than today. 9,17 Kiernan et al 29 reported a mortality rate of 22.9% for the 1990–1998 period. Many studies concluded that the high mortality was attributable to difficulties in diagnosis and delayed treatment. 30
However, as diagnostic methods, surgical techniques, and ICU protocols improved over time, outcomes and mortality have also improved over the past 20 years. 2,31 The average mortality rate based on 22 studies was 16.1%. Deu-Martin et al. found an overall mortality rate (1996–2006) of 21%. However, when the years were divided into the 1996–2000 and 2001–2006 periods, the figures differed dramatically (40% vs 4.3%). 32 In 2014, Dajer-Fadel et al published a 60-patient study reporting a mortality rate of about 35.0%, but the cited authors focused on DNM below the tracheal carina, thus the type IIA and IIB conditions as defined by Endo et al. that cause the most mortality. 33 Our mortality rate was 9.5% (2/21). One patient died of septic shock, pulmonary hypertension, and multiple organ failure; the other died of severe pneumonia and septic shock. However, multidisciplinary approaches afforded favorable results in over 80% of patients. 18 Palma et al 34 suggested that prompt ICU admission of patients with severe sepsis, as well as aggressive surgery, can significantly reduce mortality.
Limitations
Our work had certain limitations. Our patient number was small; this reduces the power of the evidence. In addition, the most patients were male. Thus, selection bias was unavoidable.
Conclusion
Multidisciplinary approaches and early comprehensive medical treatment significantly reduced mortality caused by DNM. Patients exhibiting severe inflammation and high CRP levels require intensive and aggressive intervention.
Footnotes
Acknowledgments
The authors thank all of the members of Department of Otorhinolaryngology-Head and Neck Surgery, Chang Gung Memorial Hospital, Linkou, for their invaluable help.
Author Contributions
Resources: C-YH, S-LC.
Supervision: S-LC.
Writing—original draft: C-YH, S-LC.
Writing—review and editing: C-YH, S-CC, S-LC
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Statement
This study was approved by the Institutional Review Board (IRB) of the Chang Gung Medical Foundation (IRB no. 202101172B0). The data were collected retrospectively, and the patients were anonymized before data analysis.