
Abstract
Primary diffuse cutaneous large B-cell lymphoma, leg type (PCDLBCL-LT), usually affecting one or both lower legs, with a 5-year disease-free survival rate of less than 60%. Solitary facial lesions are extremely rare. Our report is about a 93-year-old woman whose clinical examination revealed a 4 cm × 5 cm × 3 cm mass with a soft texture and smooth margins on the right side of her cheek. Immunohistochemical analyses were consistent with a diagnosis of PCDLBCL-LT. The surgical method for this patient was: extensive resection of the tumor and repair of the defect with an adjacent flap. Neither local recurrence nor systemic invasion was observed during postoperative follow-up (8 months). The clinician must be very careful when making a correct diagnosis based on the clinical and immunohistochemical findings of PCDLBCL-LT. For this type of PCDLBCL-LT isolated in 1 site without invasion of the rest of the body, extensive surgical resection may result in a favorable prognosis.
Keywords
Introduction
Primary diffuse cutaneous large B-cell lymphoma, leg type (PCDLBCL-LT) is a rare, skin-originating non-Hodgkin lymphoma. 1 PCDLBCL-LT is a moderately aggressive subtype of primary cutaneous B-cell lymphoma (PCBCL), accounting for approximately 10% to 20% of all PCBCL. 2 PCDLBCL-LT primarily affects older patients (median age, 70 years), with a female predisposition. Relapse and extracutaneous progression of PCDLBCL-LT are common and can also involve the central nervous system, with a 5-year disease-free survival rate of 40% to 60%. 3 Clinically, PCDLBCL-LT presents as a reddish brown to blue nodule or tumor on one or both of the lower extremity skin. Although known as PCDLBCL-LT, 10% to 15% of patients have lesions in anatomic areas other than the legs, compared with 2.5% to 8.6% in the head and neck region, according to previous studies. 4 The clinical manifestations are also diverse, and the occurrence of maxillofacial skin is even rarer. We report a case of PCDLBCL-LT with a buccal lesion presenting as a solitary solid and rapidly progressive mass that underwent only extended surgical resection in contrast to conventional radiotherapy and chemotherapy. To our knowledge, this is the first report of surgical treatment of facial PCDLBCL-LT.
Case Report
Eight months ago, a 93-year-old female patient came to our hospital for treatment of a subcutaneous mass on the right cheek for 6 months, which had been growing rapidly for 1 month. A spherical red raised mass was observed on the right cheek measuring approximately 4 cm × 5 cm × 3 cm in size, with a clear boundary, soft texture, and poor mobility. The deep surface infiltrated the buccal muscle and the corresponding buccal mucosa could be moved. The skin on the mass’s surface was intact, dark red in color, had low skin temperature, and exhibited no obvious tenderness. No lesions were observed on the remaining skin and mucous membranes (Figure 1A). The patient exhibited no palpable enlargements of superficial lymph nodes in the neck, armpit, and groin.
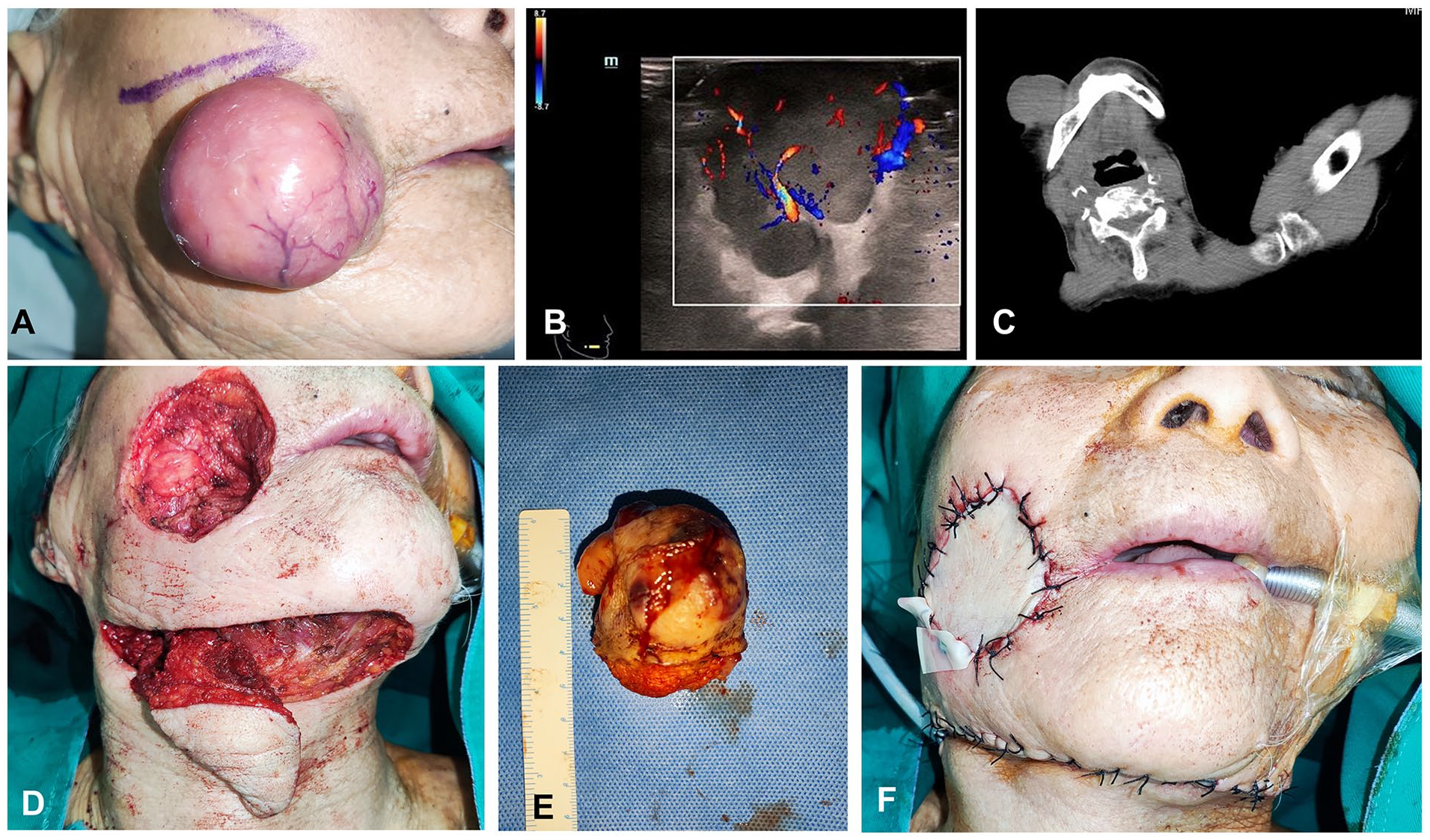
(A) Clinical findings at the first visit. Infiltrating mass located on the right cheek. (B) Color ultrasound showed a solid, hypervascular mass in the cheek. (C) Computed tomography showed that the buccal tumor was solid, and the outer surface was adhered to the epidermis with unclear boundaries; the deep surface was adhered to the buccal muscle with clear boundaries. (D and E) Extensive resection of tumor and preparation of submental island flap. (F) Repaired cheek defect.
A color ultrasound examination of the tumor revealed a solid mass with a distinct subcutaneous boundary in the cheek, a strong echo in the deep surface, and abundant internal blood flow. Neoplastic lesions were considered (Figure 1B). Cheek Computed Tomography: solid mass in the right cheek, with unclear boundary with epidermis, deep surface adhered to buccinator muscle, with clear surrounding boundary, considered as mesenchymal tumor (Figure 1C).
Surgical treatment: The patient underwent submental island flap repair after enlarged resection of the right cheek mass under general anesthesia, which recovered well after surgery (Figures 1D, 1E, and 1F). Histopathology revealed that all incisions were negative, and diffuse infiltration of tumor cells was observed in the whole dermis and subcutaneous fat, with large round cells and round nuclei, and obvious destruction of hair follicles and sweat glands (Figure 2A). Immunohistochemistry revealed that tumor cells were CD20 (+), CD79a (+), Bcl-2 (+80%), Bcl-6 (+70%), MUM1 (+), c-Myc (+30%) Ki-67 (+70%), and P53 (+, 5%) (Figures 2B, 2C, and 2D). CKpan, S-100, ALK(5A4), CD3, CD10, CD5, CD30, Cyclin D1, and EBER (in situ hybridization) were all (−).The histopathological diagnosis was PCDLBCL-LT.
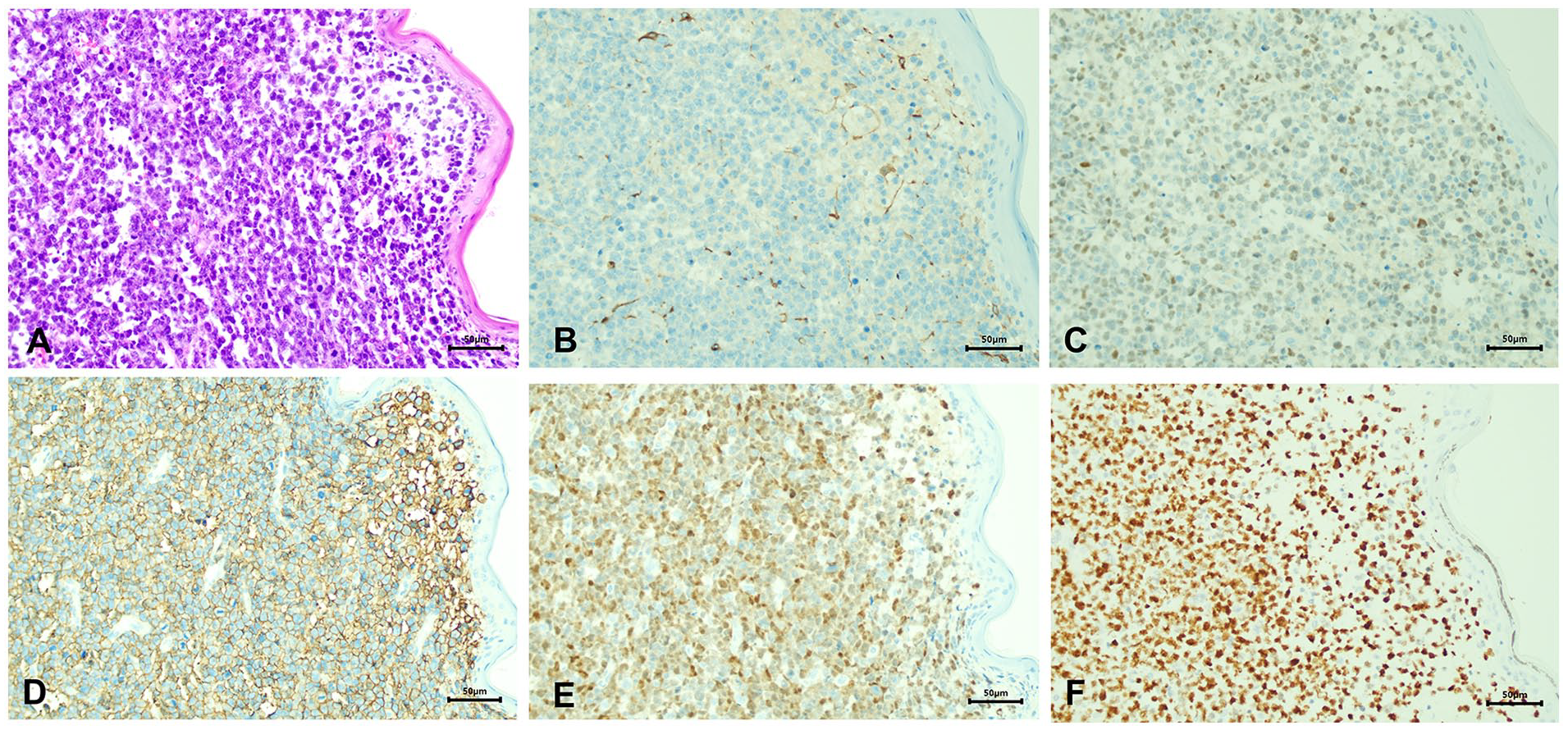
(A) Diffuse infiltration of large lymphoid cells in the dermis and subcutaneous fat (H & E, ×200). (B) Neoplastic cells are immunnegative for CD10 (IHC, ×200). (C–F) Neoplastic cells are immunpositive for Bcl-2, CD20, MUM1, and Ki67 (IHC, ×200). H & E: hematoxylin–eosin staining. IHC: immunohistochemistry. Scale bar: 50 μm.
Because of the patient’s age, the patient’s family did not agree with local radiotherapy and systematic chemotherapy. During the 8-month follow-up, the operative area healed well, the facial appearance and function were satisfactory, and there were no signs of local recurrence or metastasis to other parts of the body.
Discussion
PCBCL is a group of extranodal B-cell non-Hodgkin’s lymphoma with no evidence of extracutaneous disease at the time of diagnosis. They account for 25% of all cutaneous lymphomas and are divided into 3 main subtypes [World Health Organization (WHO), 2017]: primary cutaneous marginal band lymphoma (PCMZL), primary cutaneous follicular central cell lymphoma (PCFCL), and PCDLBCL-LT.
Among all PCBCL, PCDLBCL-LT exhibited the worst prognosis. It is considered an aggressive lymphoma with a survival rate of 5 years or lower than 60%. Half of the PCLBCL-LT patients developed extracutaneous involvement in the legs compared with other parts, with lymph nodes and the central nervous system being the most vulnerable. The localization on the leg, the presence of multiple skin localizations, the round cell morphology, the high expression of MUM1 and FOX-P1, and the deletion of the CDKN2A locus on chromosome 9p21 seem to be negative prognostic factors. 5 PCLBCL-LT has a low clinical incidence and a lack of randomized controlled trials for treatment. Many aspects of the natural history of PCDLBCL-LT are comparable to those of systemic lymphoma. Therefore, systemic chemotherapy using rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone regimen has been utilized for the treatment of PCDLBCL-LT and may be associated with improved remission and relapse rates. 6
Most of the skin lesions of PCDLBCL-LT occur in the skin of the lower extremities as a variety of lesions. Lesions of the facial skin are rare. Only 5 cases7 -11 were reported in the English literature that we could locate (Table 1). Four of these patients underwent chemotherapy due to multiple lesions or distant lesions. Another case of migratory mass on the forehead was treated with focal radiation therapy. Because of the heterogeneous features of PCDLBCL-LT’s facial clinical features, it is difficult to diagnose PCDLBCL-LT solely based on clinical physical examination and auxiliary examination.
Clinical Characteristics with Primary Cutaneous Diffuse Large B-cell Lymphoma, Leg Type of the Face.
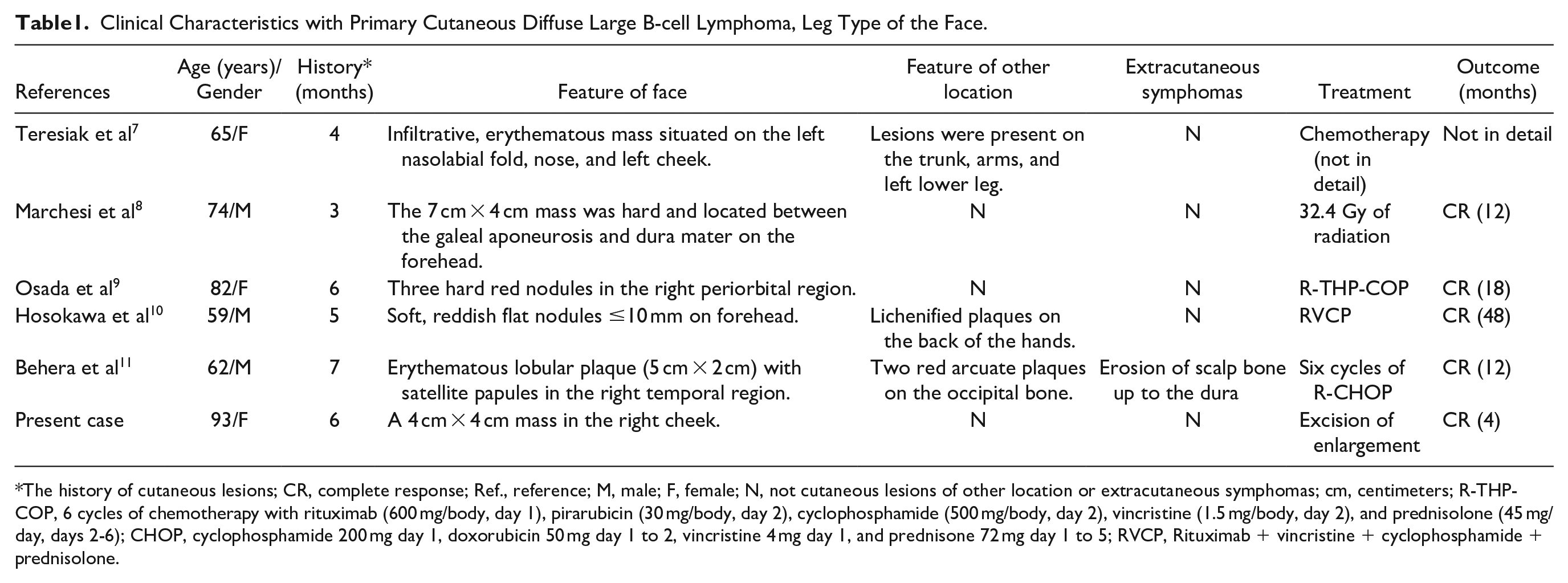
The history of cutaneous lesions; CR, complete response; Ref., reference; M, male; F, female; N, not cutaneous lesions of other location or extracutaneous symphomas; cm, centimeters; R-THP-COP, 6 cycles of chemotherapy with rituximab (600 mg/body, day 1), pirarubicin (30 mg/body, day 2), cyclophosphamide (500 mg/body, day 2), vincristine (1.5 mg/body, day 2), and prednisolone (45 mg/day, days 2-6); CHOP, cyclophosphamide 200 mg day 1, doxorubicin 50 mg day 1 to 2, vincristine 4 mg day 1, and prednisone 72 mg day 1 to 5; RVCP, Rituximab + vincristine + cyclophosphamide + prednisolone.
Unlike the aforementioned cases, our case presents solitary skin masses on the face without skin lesions or extra dermal invasion. It is easily misdiagnosed as mesenchymal tumors and small salivary gland tumors of the buccal mucosa. In our opinion, patients with isolated or limited disease in a single anatomical site are candidates for complete surgical resection compared with patients with systemic disease, refractory disease, or extracutaneous involvement. Considering the patient’s old age, the patient’s family did not accept local radiotherapy or visit the hemato-oncology department for systematic treatment. No local recurrence or invasion of other parts of the body was found in the patient’s 8-month follow-up.
Conclusion
This case highlights that PCDLBCL-LT can develop in the face in a highly localized manner and broadens the range of clinical presentations observed in patients with PCDLBCL-LT. For isolated PCDLBCL-LT that has not invaded other parts of the body, extensive surgical resection may result in a favorable prognosis.
Footnotes
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Statement
The studies involving human participants were reviewed and approved by the ethics committee of the Affiliated Hospital of Qingdao University. The patients/participants provided their written informed consent to participate in this study.