
Abstract
Keywords
Introduction
Despite the widespread use of antibiotics to treat early infections of the head and neck, bacteria continue to cause abscesses in the infected organ. Parapharyngeal abscess (PPA), one of the most common abscesses of the deep head and neck, is difficult to diagnose and largely treated in hospital. The PPA patient usually complains of sore throat, dysphagia, and fever with physical findings of trismus, displacement of the lateral pharyngeal wall, and occasional external swelling.1-3 In general, PPA only accounted for approximately 2.7% of deep neck abscesses in previous studies.4,5 However, PPA should be treated immediately because it can be life-threatening. Many problems, such as etiology, predisposing factors, and therapeutic methods, are still controversial.3,6 The recommended treatment of PPA has been early open surgical drainage in the traditional view. 7 However, in some studies, PPA was treated conservatively without the need for early open surgical drainage if the PPA was localized to the parapharyngeal space.8,9
For a patient suffered from PPA, which method should be used, the conservatively antibiotic-only method or the surgical drainage method? How to determine the timing of surgery? Given the incomplete understanding of this disease, this study aimed to better understand the characteristics of PPA and to evaluate the therapeutic effects of the 2 methods.
Materials and Methods
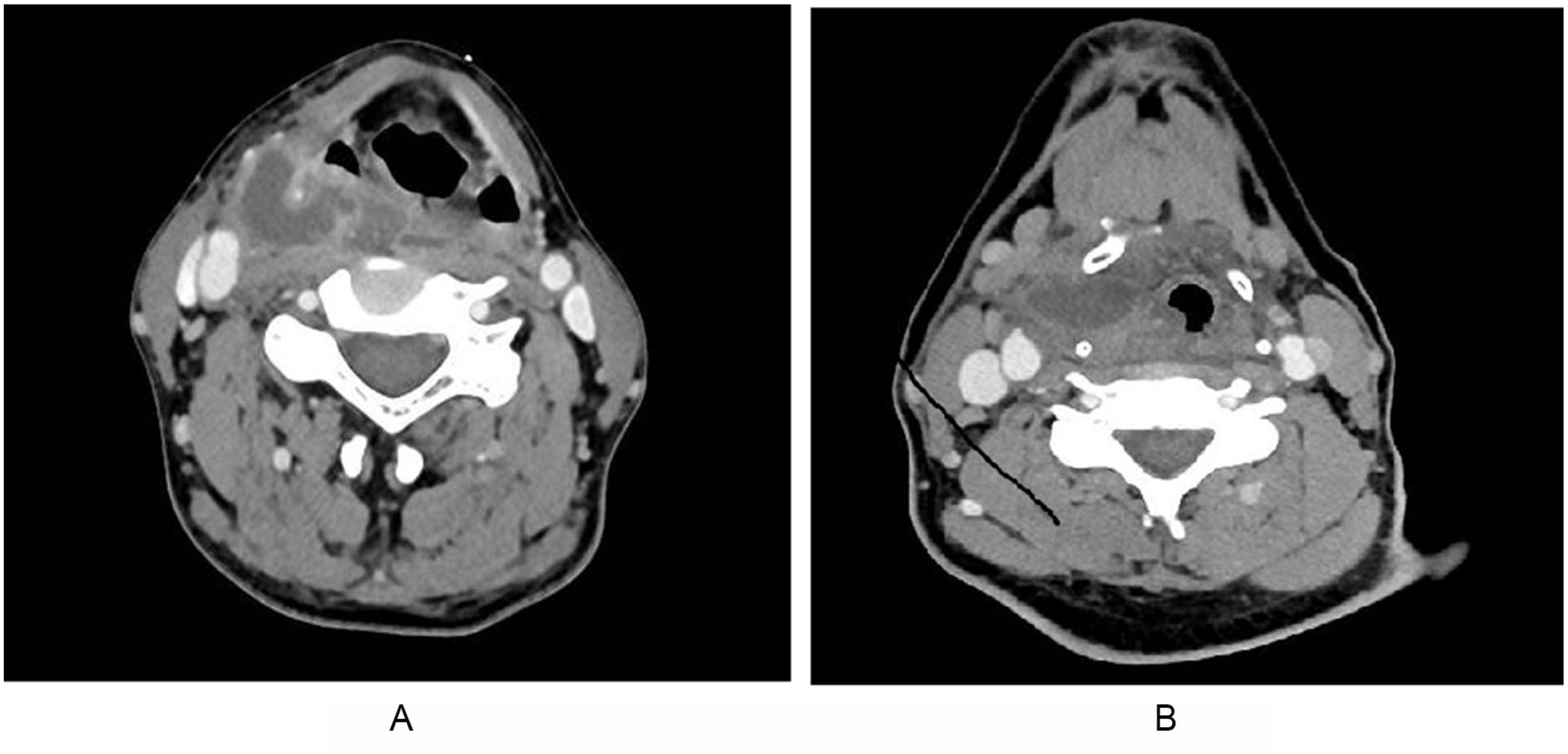
We retrospectively collated the medical record reviews of 49 PPA patients who were treated as inpatients at the Department of Otorhinolaryngology between April 2013 and May 2021. A retrospective chart review was performed, and data were collected, including demographic characteristics (age, sex, smoking, and alcoholism), medical history (diabetes mellitus and hypertension), clinical symptoms and signs, white blood cell count, contrast-enhanced computed tomography (CT) results, antibiotic usage, and operation methods. Surgically drained pus was used to culture bacteria and find sensitive antibiotics. For the PPA patients who were treated with antibiotics, throat swabs were used. PPA was diagnosed by contrast-enhanced CT (Figure 1). Patients who had superficial infection with cellulitis, patients with parapharyngeal space tumors, patients with postsurgical infections, patients with severe mediastinal abscesses, or patients who were unable to comply with treatment were excluded from the study. Finally, 49 patients were enrolled in the study. The PPA patients were divided into 2 groups according to whether they underwent surgery: the surgery group (n = 35) and the antibiotic-only group (n = 14).
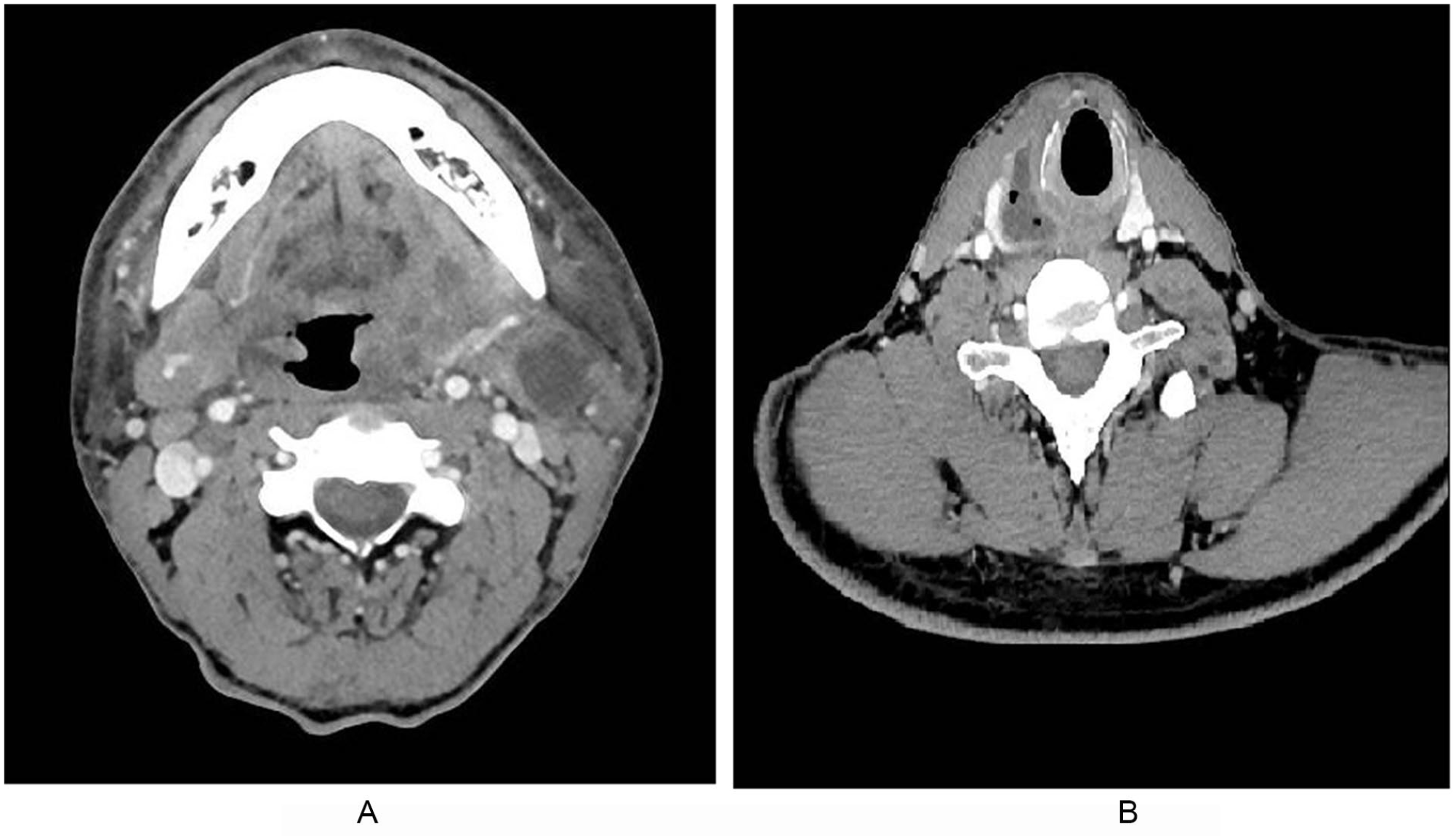
The abscess could be found in parapharyngeal space. A: Parapharyngeal abscess can be drained via external cervical approach. B: Parapharyngeal abscess can be drained via caliber approach.
Treatment Protocol
When a patient was hospitalized and diagnosed with PPA, third-generation cephalosporins (ceftriaxone sodium or ceftazidime), ornidazole, and dexamethasone were used as empiric therapy. If the PPA patient was diabetic, dexamethasone was used in reduced doses or not used, following the advice of the endocrinologist. The empiric antibiotics were used for 2 days. If these drugs were effective and the abscess was localized, the medication was continued, and the operation was postponed. If the drug treatment was ineffective, the abscess was large, or the disease continued to progress, surgical treatment was adopted. However, the surgical treatment was performed immediately if the PPA was progressive or dyspnea was found. In the surgery, pus was obtained and used to culture bacteria and find sensitive antibiotics. Antibiotics were selected according to the results of bacterial culture. The treatment protocol is shown in Figure 2.
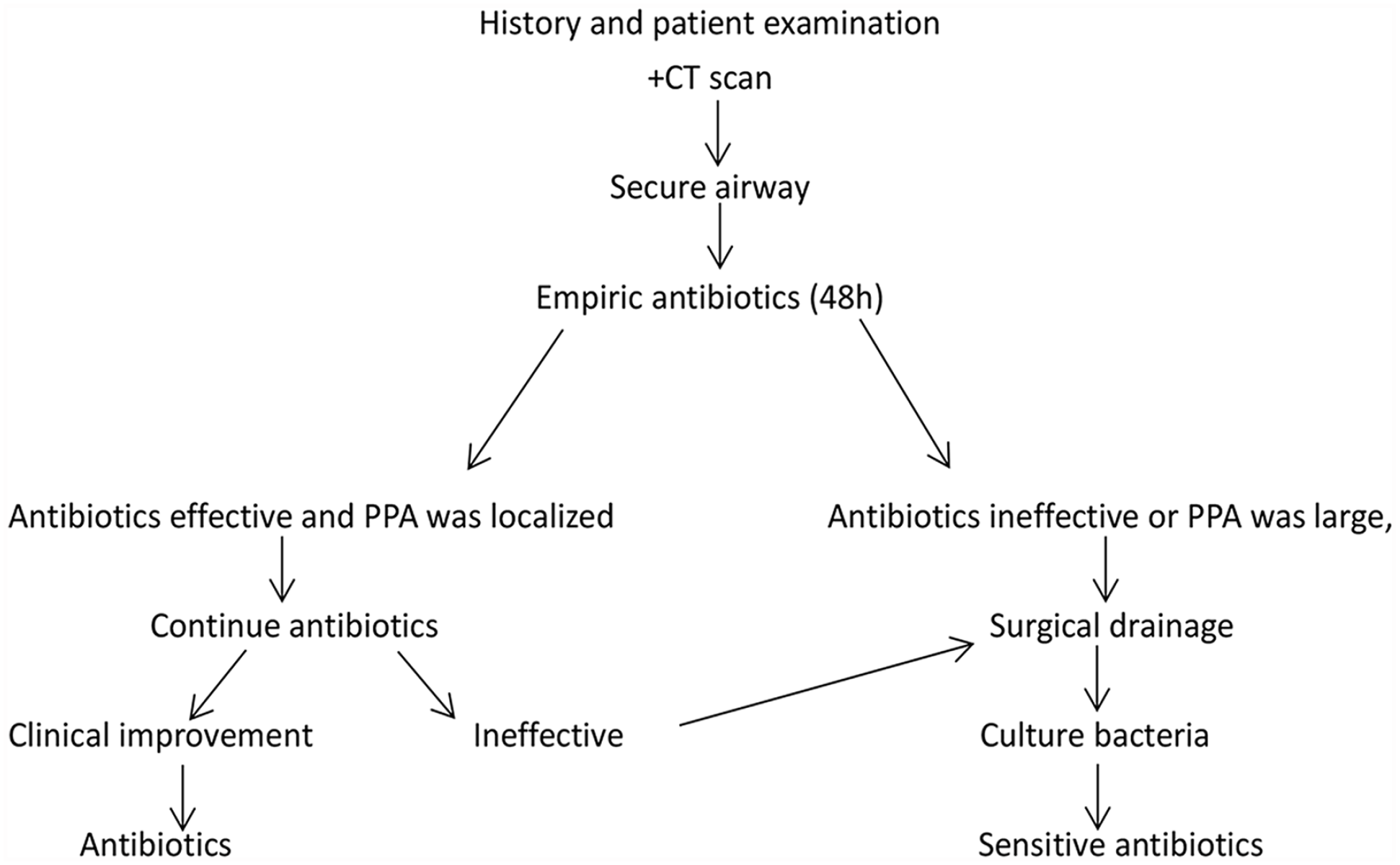
Treatment protocol for patients with parapharyngeal abscess.
Surgical Procedures
Prior to surgery, all patients underwent a complete evaluation including chest radiography, renal function tests, electrocardiogram, and blood examinations to exclude systemic diseases. All the operations were performed under general anesthesia in the supine position.
Incision and Drainage of PPA via the Caliber Approach
After the general anesthesia, a direct laryngoscope was introduced to expose the laryngeal cavity, and a microscope was placed. At the most prominent part of the abscess, a puncture needle was used to puncture and suck the pus. Then, a longitudinal incision was made, the mucosa and submucosal tissues were cut, the muscle tissue was separated with the pus cavity so that the pus overflowed, and the pus was sucked up with a suction device.
Incision and Drainage of PPA via the External Cervical Approach
If the abscess was deep and not close to the lateral pharyngeal wall, surgery via the external cervical approach was undertaken (Figure 3), using the following steps:
A cervical skin incision is made along the front edge of the sternocleidomastoid muscle, which starts form the lower edge of mandibular angle and arc and downward to the level of the hyoid bone.
The incision includes skin and subcutaneous tissue. The submandibular gland is exposed and separated upward along the lower edge of it with vascular forceps, followed by separating from the styloid process in the direction of the skull base. Then, detachment can reach up to the front part of the PPA.
Separating backward along the front edge of the sternocleidomastoid muscle, the internal and external carotid arteries and internal jugular vein are exposed and separated along the anterior fascia of cervical vertebra with vascular forceps to drain the posterior part of the pharyngeal space. After draining as much pus as possible, a drainage tube is placed and the incision is sutured.
If the PPA is accompanied by a deep neck abscess, incision and drainage of the deep neck abscess are undertaken together.
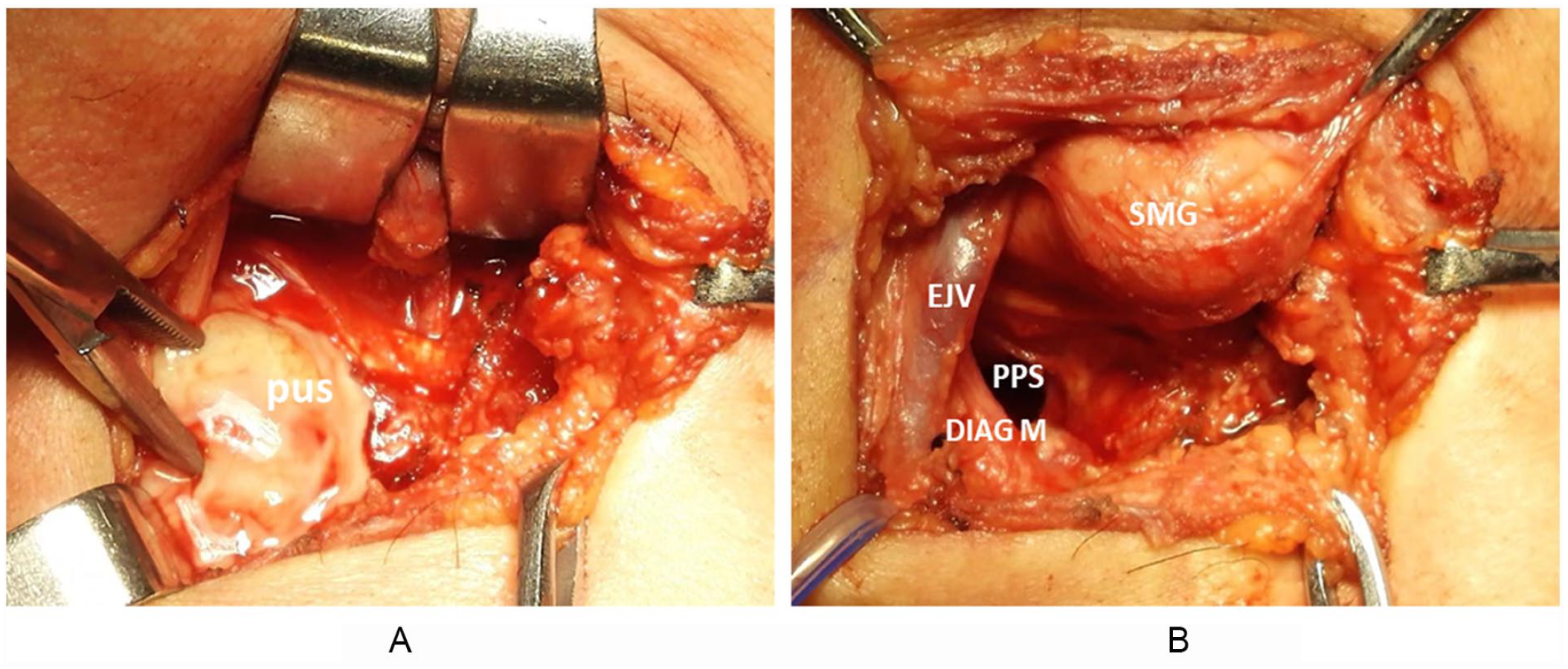
(A) Intraoperative image of abscess (a) before drainage and (b) after drainage.
Tracheotomy was undertaken in 2 patients who had dyspnea when the surgery was performed.
Patient Outcome Measures
All patients were evaluated for clinical symptoms and signs during hospitalization. The duration from onset to treatment was recorded. Discharge criteria included the following: (1) The pain symptoms were significantly reduced, and other symptoms such as dysphagia, dyspnea, and restricted mouth opening disappeared completely. (2) The abscess disappeared completely, systemic symptoms such as increased temperature disappeared, the neck was soft without swelling, and the physical examination was normal, with no swelling of the pharynx and larynx.
Statistical Analysis
The SPSS 21.0 program (SPSS Inc, an IBM Company) was used for the statistical analysis. The continuous variables were analyzed by the independent t test, and the categorical variables were analyzed by the Mann–Whitney U test. Linear regression was used to analyze the relationship between the hospital stay and other relevant factors (binary classification variables were converted to dummy variables). All continuous data were presented as mean ± SD. A P value less than .050 was considered statistically significant.
Results
In total, 49 patients who met the research criteria were identified. All the patients were diagnosed by contrast-enhanced CT (Figure 1). The inclusion and exclusion criteria were based on a chart review described previously. Six patients were excluded, 2 due to having cellulitis, 2 due to having parapharyngeal space tumors, and 2 due to having a severe mediastinal abscess concurrently. Of the 49 patients, 34 were males and 15 were females. Patients age ranged from 6 to 84 years. The mean age of the patients was 53.5 ± 18.1 years. Four patients were younger than 18 years old, 11 patients were 18-49 years old, 28 patients were 50-69 years old, and 6 patients were over 70 years old. Presenting symptoms were sore throat, dysphagia, odynophagia, cervicodynia, trismus, displacement of the lateral pharyngeal wall, dyspnea, external swelling, and occasional fever.
Among the 49 PPA patients, 13 (26.5%) suffered from diabetes, with a higher prevalence than that of the general population (9.3%). 10 Twelve (24.5%) among the 49 patients suffered from hypertension. Six patients had a history of accidental swallowing prior to onset. Five patients swallowed fish bones by mistake, and the other swallowed a chicken bone. A fish bone was found in the parapharyngeal space in only 1 patient through surgery and contrast-enhanced CT. One patient with PPA was diagnosed with tuberculosis by pathological examination. The patient was a nurse who worked in the flexible bronchoscopy department with a history of bronchoscopy in tuberculosis patients. The patient received anti-tuberculosis therapy after surgery. This patient was studied alone. The other patients with bacterial infection were studied as follows.
In the 48 patients with bacterial infection, 6 (12.5%) had complications of peritonsillar abscess and 17 (35.4%) had complications of deep neck abscess (Figure 4). Only 25 (52.1%) PPAs were isolated abscesses without other neck abscesses. In addition, 34 patients were treated by surgery, and 14 were treated by antibiotics only. Among the patients treated by surgery, 2 underwent tracheotomy at the same time due to dyspnea. In the surgery group, 26 patients underwent incision and drainage of PPA via the external cervical approach, and 8 via the caliber approach (Figure 5). Surgically drained pus was used to culture bacteria. A negative culture was seen in 58.8%. Bacterial cultures were positive in 14 patients (41.2%). Among these positive patients, Streptococcus was the most common organism (71.4%), followed by Klebsiella pneumoniae (21.4%) and Enterobacter cloacae which was found in the parapharyngeal space with the fish bone (7.1%). Streptococcus was found in 10 patients, 5 with Streptococcus constellatus, 4 with group A Streptococcus, and 1 with group D Streptococcus. One patient’s culture was positive for Streptococcus constellatus and anaerobes at the same time. In the antibiotic-only group, only 1 was positive for Streptococcus constellatus and 1 for group A Streptococcus in the throat swab test.
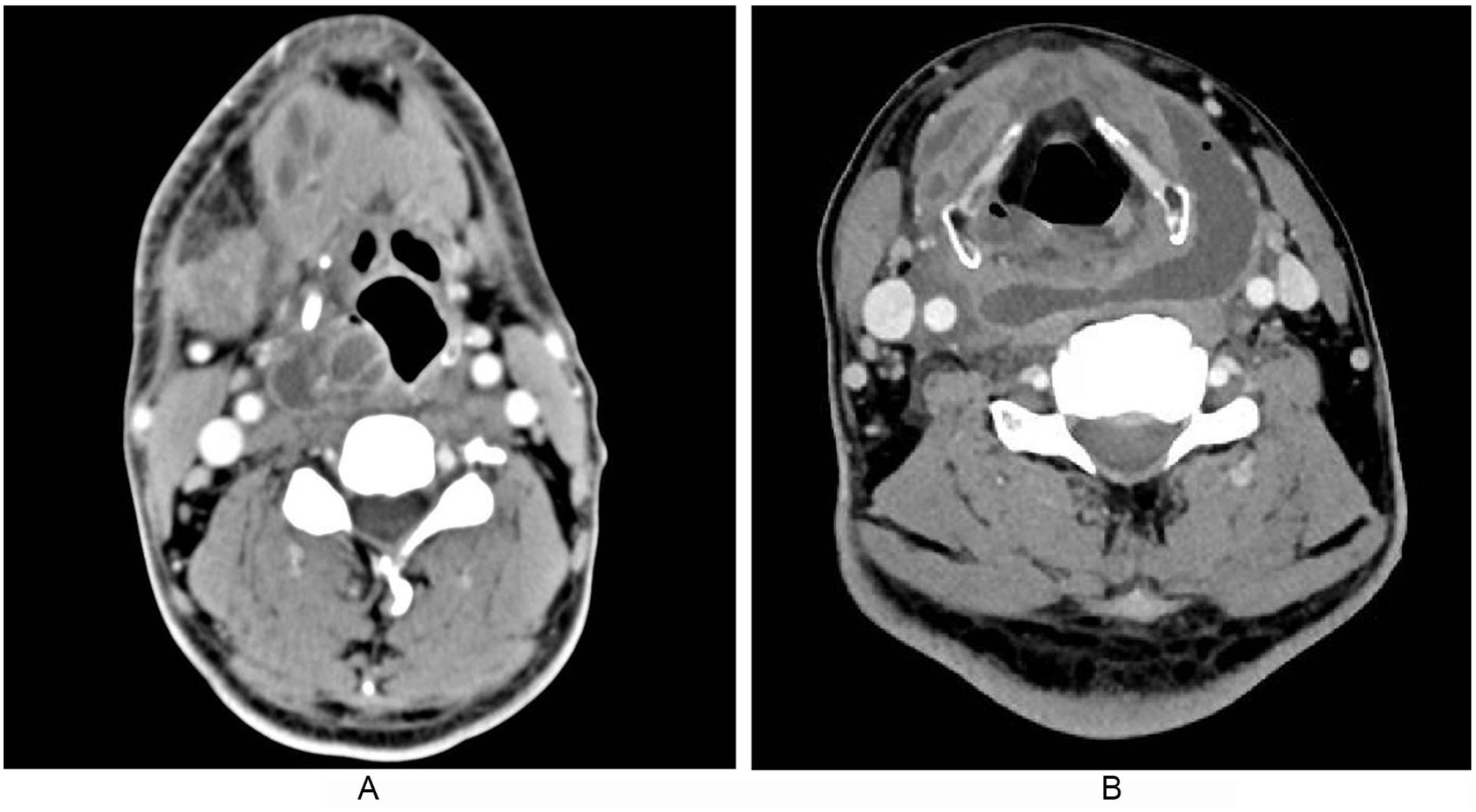
(A) Parapharyngeal abscess with peritonsillar space abscess was seen in 1 patient. (B) Parapharyngeal space abscess with deep neck abscess was seen in 1 patient.
(A) Parapharyngeal abscess patient would be treated by incision and drainage of PPA via external cervical approach. (B) Parapharyngeal space abscess patient would be treated by incision and drainage of PPA via caliber approach.
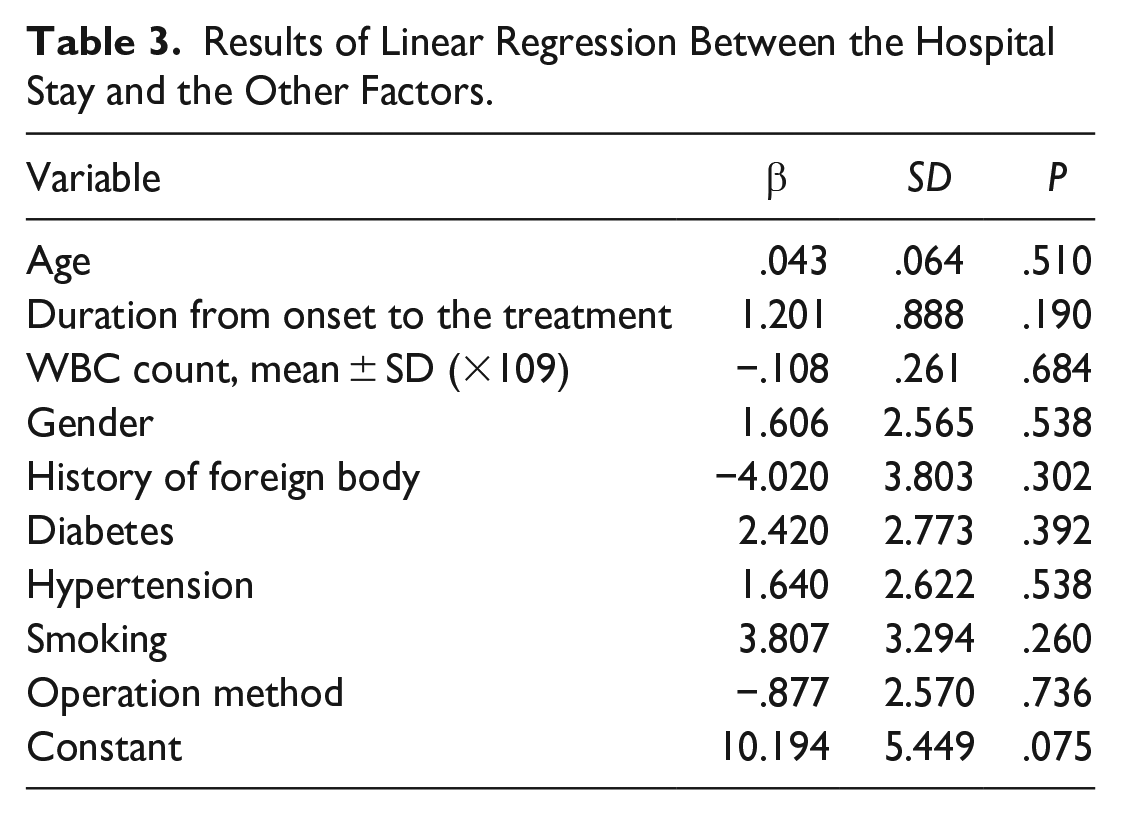
All patients in the 2 groups were cured and experienced no side effects. Furthermore, no significant difference was found in the results of the mean white blood cell count, demographic characteristics, and medical history at the time of presentation (Table 1). Hospital stay ranged from 3 to 30 days. Interestingly, the length of hospital stay was shorter in the antibiotic-only group than in the surgery group (P < 0.05). Furthermore, the duration from onset to treatment in the antibiotic-only group was shorter than in the surgery group (Table 2). No correlation was found between hospital stay with diabetes, history of accidental swallowing, age, and white blood cell count (Table 3). One PPA patient suffered from a mediastinal abscess in the course of treatment. Incision and drainage of the PPA and mediastinal abscess were undertaken. Two patients were excluded due to having a severe mediastinal abscess concurrently, and incision and drainage of the mediastinal abscess were undertaken by a thoracic surgeon. Other severe complications were not found in our study.
Comparison of Baseline Characteristics in 2 Groups.
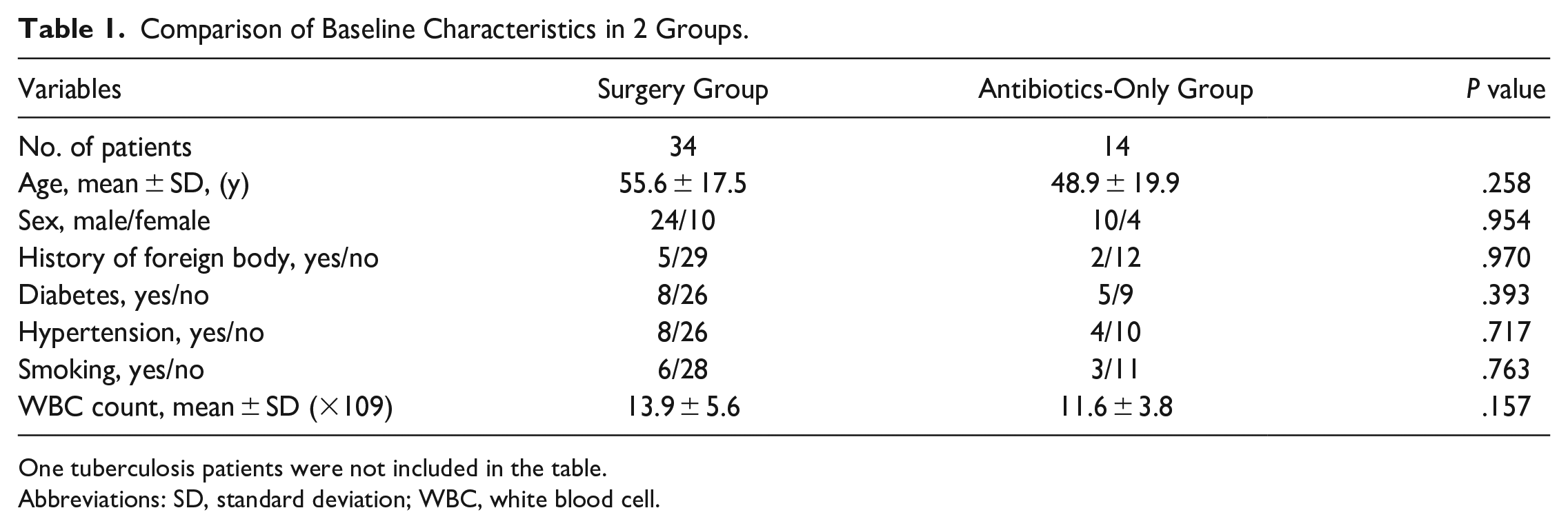
One tuberculosis patients were not included in the table.
Abbreviations: SD, standard deviation; WBC, white blood cell.
Comparison of Hospital Stay and Duration From Onset to the Treatment. a

One tuberculosis patients were not included in the table.
Values are presented as days (mean ± standard deviation).
Results of Linear Regression Between the Hospital Stay and the Other Factors.
Discussion
Peritonsillar abscesses, PPAs, and posterior pharyngeal space abscesses are the most common types of abscesses in the head and neck. Peritonsillar abscesses are easily found and treated by peritonsillar abscess puncture or drainage. Posterior pharyngeal space abscesses are usually caused by tuberculosis. Parapharyngeal abscess is the second most common deep neck abscess after peritonsillar abscess. However, parapharyngeal space abscesses are difficult to diagnose and treat.
The parapharyngeal space is an inverted cone-shaped potential space that has the following boundaries: superiorly, the skull base; interiorly, the hyoid; medially, the buccopharyngeal fascia; laterally, the pterygoid muscles and mandible; anteriorly, the submandibular space; and posteriorly, the retropharyngeal space. This anatomical feature makes PPA near neither the lateral neck nor the lateral pharyngeal wall, which makes the operation more difficult.
In previous research, PPA was regarded as an affliction of younger persons, particularly those under 30, and less likely to occur in older people.3,11 In our study, the 49 PPA patients ranged in age from 6 to 84, and their mean age was 53.5 ± 18.1 years, differing from previous studies.3,8 However, a difference in age was not found between the 2 groups, and age was not correlated with hospital stay. The results were similar to those of a previous study on deep neck space infections. 4 This could imply that age is not a factor affecting morbidity and prognosis.
The bacteria in the deep neck space infections were usually found to produce extensive-spectrum β-lactamases. 12 Therefore, third-generation cephalosporins, piperacillin, and quinolones can be recommended as empiric antibiotics to treat patients with a deep neck space abscess.5,12 In our study, ceftriaxone or ceftazidime combined with ornidazole was used as the empiric antibiotic to treat PPA. According to the bacterial culture and drug sensitivity results, antibiotic treatment should be de-escalated to the narrowest effective agent once pathogen identification and sensitivities are established and/or adequate clinical improvement is noted. The cultures of the pus of the abscess from all 20 patients in the surgery group failed to yield bacteria, which was probably due to antibiotic treatments before the surgery, after admission.
In the 48 patients with bacterial infection, only 25 (52.1%) PPAs were isolated abscesses without other deep neck abscesses, 17 (35.4%) patients had complications with other deep neck abscess, and 6 (12.5%) patients had complications with a peritonsillar abscess. This indicates that PPAs probably occur with other neck abscesses. Neck abscesses should be treated when PPAs are treated. A previous study 13 showed that PPAs were frequently associated with concomitant peritonsillar abscesses; however, PPAs usually occurred with other deep neck abscesses in our study.
In the traditional view, open surgical drainage should be performed immediately after the abscess was found. 7 However, for the PPA which was localized to the parapharyngeal space, conservatively empiric antibiotics were only used.8,9 Our treatment protocol for PPA was to administer antibiotics immediately after diagnosing with PPA and admission. Only if the drug treatment was ineffective, the abscess was large, or the disease continued to progress, and surgical treatment was adopted. Therefore, according to the treatment protocol, the PPAs in the antibiotic-only group were milder than those in the surgery group. However, the duration from onset to treatment in the antibiotic-only group was shorter than in the surgery group. This result showed that the antibiotic-only method was also recommended for the PPA which was effective for the empiric antibiotics and localized. After all, the procedure carries a risk of major hemorrhage from a vein or artery in the parapharyngeal space (internal carotid artery, external carotid artery, common carotid artery, and internal jugular vein), a risk of nerve injury (cranial nerves IX-XII), and a risk of dyspnea with hemorrhage. In our study, 14/48 patients with bacterial PPA were cured with antibiotics alone. This also suggests that the early diagnosis and treatment of PPA might ultimately reduce the severity of PPA. Early identification of PPA is often challenging. Contrast-enhanced CT plays a critical role in diagnosis and localization of abscesses. 14
The incidence of diabetes mellitus in PPA was significantly higher than that of the general population, which could imply that it was one of the risk factors causing PPA. However, it had no correlation with hospital stay; this might be because many factors affect the treatment of PPA, such as bacterial virulence, surgical method, and the time at which treatment of disease begins. 15
The incidence of PPA complications has diminished greatly since the pre-antibiotic period. Many severe complications, such as internal jugular vein thrombosis, carotid artery rupture, and meningitis, were not found in our study. Only 1 patient in our study suffered from mediastinal abscess. Two patients were excluded from our study and referred to the department of thoracic surgery. However, we must remain vigilant to diagnose and treat these complications in the treatment of PPA.16-21
This study had several limitations. First, we observed a low positivity rate in bacterial cultures, which might because of the usage of antibiotics before surgery. Second, the time of bacterial culture was long, and empiric antibiotics were usually used for a long time without the support of this bacteriological evidence.
Conclusions
PPAs continue to occur despite the wide use of antibiotics. The emergence of antibiotic-resistant strains might explain the occurrence of PPAs. This result showed that the antibiotic-only method was also recommended for the PPA which was effective for the empiric antibiotics and localized, on the basis of careful observation of the changes in PPA. Early diagnosis and treatment of PPA could ultimately reduce the severity of PPA.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Science and Technology Commission of Shanghai Municipality (CN) (grant number: 18411965600).
Ethical Statement
The research ethics board of our hospital approved the study and waived the requirement for informed consent due to its retrospective nature.
Data Availability Statement
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.