
Abstract
Parapharyngeal infection is a well-known disease of otorhinolaryngologists. Rapid onset, short duration, severe symptoms, and manifestations such as sore throat and dysphagia are common characteristics treated primarily by surgical incision and drainage. Traditional surgical approaches encompass endoscopic transoral/nasal, transparotid, transcervical, or a combination thereof. We report a novel technique of nasal endoscopic incision and drainage transnasal retropterygoid approach to an upper parapharyngeal abscess. This report presents a case of a 14-year-old man presented with severe right neck and head pain, who was found to have an upper parapharyngeal abscess during a nasal endoscopic parapharyngeal exploration via a retropterygoid approach. The intraoperative frozen section revealed chronic mucosal inflammation and mild to moderate dysplasia of the squamous epithelium, but no carcinoma.
Introduction
The parapharyngeal is divided into upper, middle, and lower parapharyngeal, in which the lower edge of the lateral pterygoid muscle and the level of the mandibular angle are anatomical demarcations. The parapharyngeal abscess (PPA) site is deep and develops rapidly and can endanger the patient’s life. Early detection and intervention are crucial, with surgical incision and drainage considered the preferred treatment strategy. A novel technique, endoscopic sinus surgery via the retropterygoid approach to the upper parapharyngeal, was used to treat upper parapharyngeal abscesses, which are reported as follows.
Case Report
A 14-year-old male reported to a local hospital, presenting with severe paroxysmal pain in the right side of the neck and head that had persisted for the past 3 days. No fever, nasal obstruction, or hemoptysis were reported. An initial head CT scan at the local hospital revealed irregular thickening and slightly hypodense shadows within the right wall of the nasopharynx. No other tests or treatment were performed due to medical level restrictions. Following these findings, the patient was immediately referred to our hospital. Upon physical examination, the patient had a body temperature of 36.5°C, exhibited no neck erythema or swelling, remained active, no tooth decay or inflammation in oral cavity, and intact tympanic membrane. An observable, orange valve-like bulge in the nasopharynx was detected with smooth mucosa, suggestive of adenoid residue (Figure 1). No obvious congestion or inflammatory exudation in oropharynx, no tonsillar enlargement, no obvious bulge in lateral oropharyngeal wall, but congestion was noted in the right external auditory canal. The nasopharyngeal MRI plain scan plus enhanced scan showed a slightly low signal intensity in the right parapharyngeal T1-weighted images (T1WI), while T2-weighted images (T2WI) revealed mixed high signal intensity, Range 23 * 20 mm. The enhanced scan demonstrated heterogeneous enhancement (Figure 2). Multiple bilateral cervical lymphadenopathies, larger than about 8 mm. Blood examination upon admission indicated an elevated white blood cell (WBC) count at 18.27 × 109/L and neutrophil ratio (NEUT) at 81.3%. The preoperative diagnosis was made based on these findings: potential parapharyngeal space lesions (abscess or nasopharyngeal carcinoma with infection) alongside right otitis externa.
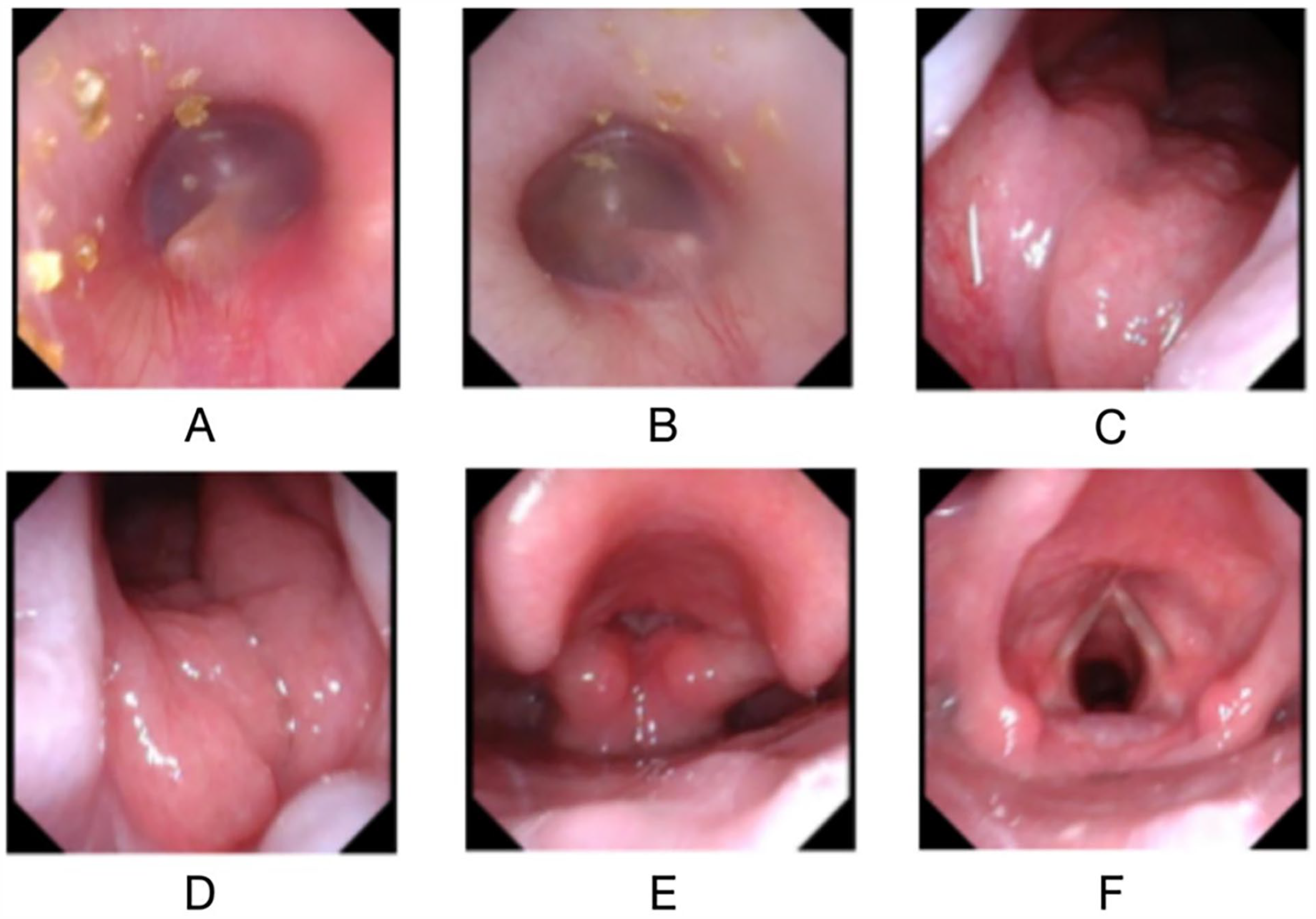
Electronic nasopharyngoscope. Congestion was noted in the right external auditory canal (A). An observable, orange valve-like bulge in the nasopharynx was detected with smooth mucosa, suggestive of adenoid residue (B/C).
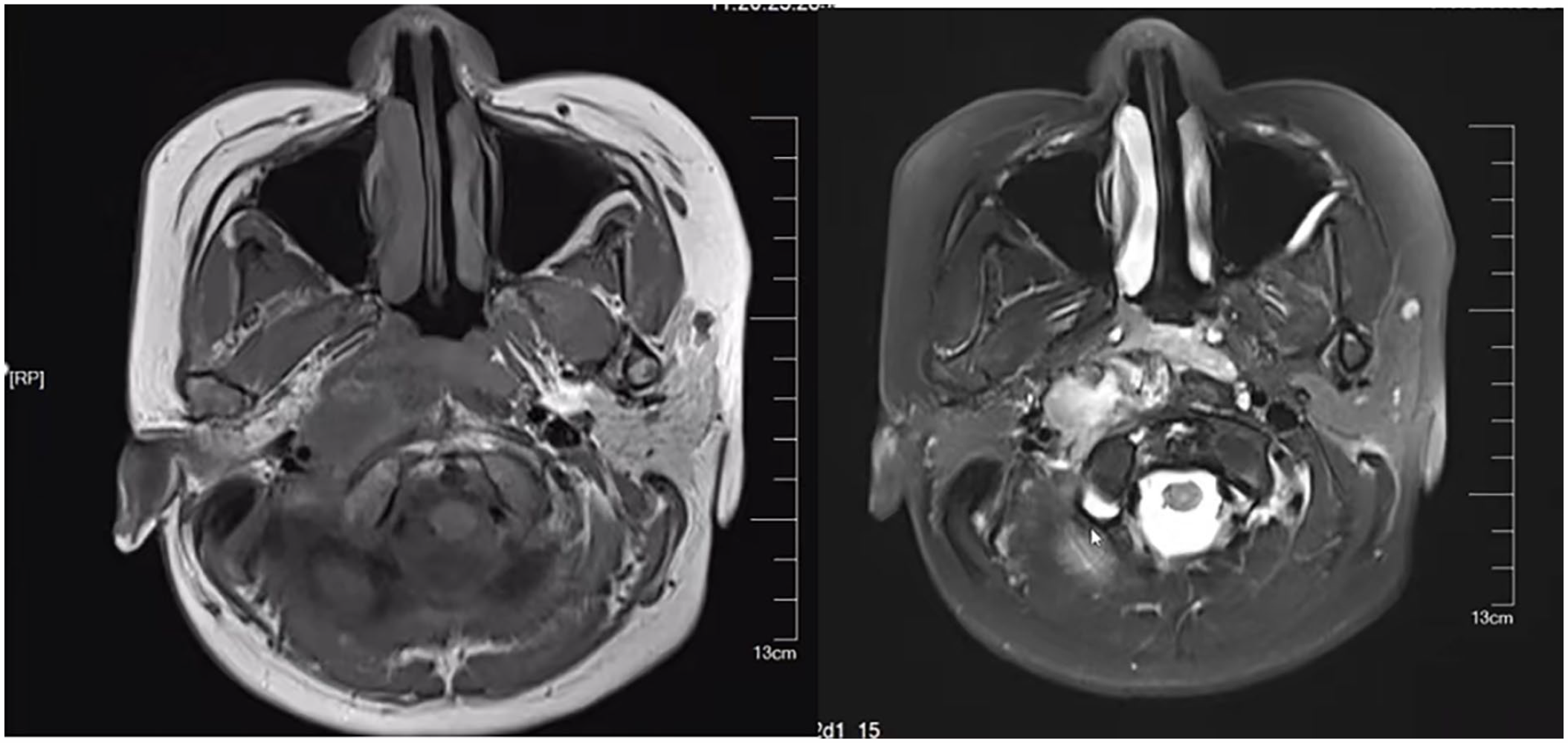
Nasopharyngeal MRI and contrast-enhanced scan. The nasopharyngeal MRI plain scan plus enhanced scan showed a slightly low signal intensity in the right parapharyngeal T1-weighted images (left). The enhanced scan demonstrated heterogeneous enhancement, Range 23 * 20 mm (right).
The nasopharyngeal mucosa was smooth, and pathology results indicated chronic inflammation of the nasopharynx. Puncture not performed due to small lymph nodes. The patient’s MRI, however, suggested the presence of malignant tumors, prompting the decision for a secondary pathological examination under general anesthesia. Exploration of the parapharyngeal via the retropterygoid approach was performed under a nasal endoscope 3 days later. The posterior end of the right inferior turbinate was first removed, followed by a plasma incision to dissect the surface tissue of the medial pterygoid plate and the anterior occipital tissue of the torus tubarius. Adipose tissue was observed in the parapharyngeal and was subsequently excised. The torus tubarius was sutured, and silk thread traction was used to expose the surgical cavity. The upper parapharyngeal was further enlarged by separating the tensor veli palatini from levator veli palatini and approximately 10 ml of yellowish pus was extracted during the operation. The operative area was repeatedly irrigated with iodophor and normal saline (Figure 3). The intraoperative frozen section revealed chronic mucosal inflammation, mild to moderate dysplasia of the squamous epithelium, and absence of carcinoma. Pus sent for culture yielded negative results. Postoperatively, the patient reported relief from neck pain and was diagnosed with a PPA and right otitis externa. The patient was treated with ceftazidime and ornidazole for anti-infection treatment and nasal irrigation. Five days posttreatment, the patient fully recovered from neck and head pain. Blood examination indicated an elevated WBC count at 9.34 × 109/L and NEUT at 71.5%. The patient reported no discomfort during the 6-month follow-up.
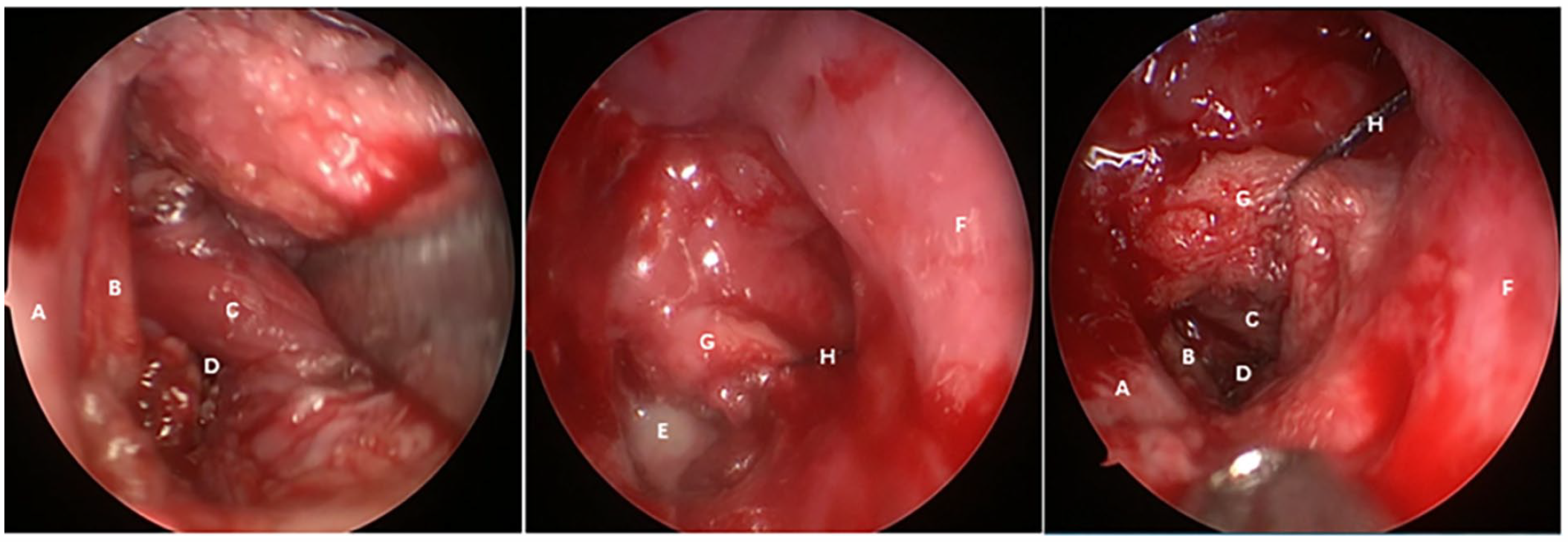
Intraoperative images followed by a plasma incision to dissect the surface tissue of the inner pterygoid plate and the anterior occipital tissue of the torus tubarius. We can see upper parapharyngeal (left). Pus filling upper parapharyngeal (middle). Upper parapharyngeal and surrounding tissues (right).
Discussion
PPA, resultant from suppurative inflammation in the parapharyngeal, are categorized into 2 types: acute and chronic. Failure to promptly manage PPA can result in severe complications such as retropharyngeal abscess, mediastinal abscess, thrombophlebitis, sepsis, and carotid sheath infection. 1 PPA, as demonstrated on CT scans, present as soft tissue swelling, lateral or posterior pharyngeal wall thickening, unclear boundaries with adjacent muscle groups, localized narrowing of the pharyngeal cavity, and relatively hypodense round or fusiform areas within the thickened soft tissue, often accompanied by ring enhancement or septation-like enhancement post-contrast. Sagittal MRI images typically depict a thickening of the posterior pharyngeal wall, and in the presence of an abscess, the pus exhibits high signal intensity on T2WI, with significant peripheral enhancement. 2 Conventional treatment for PPA in adults is antibiotic therapy plus surgical drainage, while in children the role of surgical drainage versus conservative treatment remains controversial. 3 A retrospective survey of the PPA in children showed an age cutoff of 4.2 years for conservative treatment and 23 mm 4 for abscess size for conservative treatment. In this case, the patient was 14 years old, the size of the abscess was about 23 mm, and the patient was difficult to diagnose. Surgical exploration was also an indication. The anatomy of the parapharyngeal is special and adjacent to many important tissues and organs. It is shaped like an inverted pyramid with its skull base and its apex pointing down to the large corner of the hyoid bone. The parapharyngeal is limited anteriorly by the pterygomandibular raphe and pterygoid fascia and posteriorly by the cervical spine and prevertebral muscles. The medial border of the parapharyngeal is the pharynx, and the lateral border includes the mandibular branches, the medial pterygoid muscle, and the parapharyngeal of the deep lobe of the parotid gland. The parapharyngeal is divided into upper, middle, and lower parapharyngeal, in which the lower edge of the lateral pterygoid muscle and the level of the mandibular angle are anatomical demarcations. Timely incision, drainage, and the selection of an appropriate surgical approach are pivotal in reducing postoperative complications and ensuring surgical success. For lesions located in the lower parapharyngeal, oral and/or transmandibular incisions, cervical submandibular approaches, and transparotid approaches can be an option.5 -7 At present, the surgical treatment of lesions in the upper parapharyngeal (hard palate plane) is still a great challenge, and the treatment of lesions in this site through the external approach through the parotid approach requires dissection of the facial nerve and removal of the styloid process. But the exposure of the surgical area is still unsatisfactory, and there are many postoperative complications. Notably, the surgical management of PPAs has been sparsely documented in medical literature.8 -10 Modern endoscopic techniques are becoming more and more mature, and endoscopic transpterygoid approaches have been reported to manage lesions in the upper parapharyngeal space.11,12 The transpterygoid approach requires prior resection of the pterygoid process, and the transnasal retropterygoid approach through the nasal endoscope into the upper parapharyngeal is a novel technique, which can preserve the pterygoid process with less injury. The transnasal retropterygoid approaches the parapharyngeal by removing the mucosa medial to the pterygoid plate and the mucosa below the pharyngeal orifice of the eustachian tube. This approach is closer, less workload, less damage to normal tissue, can obtain a clear view, reduce intraoperative bleeding, has a lower probability of postoperative infection, and does not affect the patient’s eating after surgery. However, there are extremely few reports of this procedure, with only 3 cases. Fudan University’s Juan Liu et al. have reported 3 cases, involving biopsies of benign chondroma, nerve sheath tumor, and nasopharyngeal carcinoma in the parapharyngeal space. 13 Our case marks the first application of this procedure for incision and drainage of a PPA, which led to the patient’s successful recovery. This innovative approach presents a novel clinical perspective for treating parapharyngeal diseases.
This procedure is generally deemed appropriate for diseases confined within specific anatomical boundaries: anterior to the pterygoid process, posterior to the prevertebral muscles and carotid sheath, superior to the eustachian tube, inferior to the level of the palatum durum, medially to the level of the nasopharyngeal cavity, and laterally to the level of the lateral pterygoid process. 13
In this particular case, the abscess was situated medial to the internal carotid artery. To circumvent cervical scarring and internal carotid artery injury, an oral or nasal approach was initially considered, given the patient’s inconspicuous parapharyngeal bulge. However, intraoral incisions pose a risk of contamination by oral secretions and necessitate a nasogastric feeding tube diet. Given the patient’s lesion aligned with the aforementioned spatial boundaries, an endoscopic transnasal retropterygoid approach to the upper parapharyngeal space was deemed suitable.
Selecting an appropriate surgical approach is crucial due to the parapharyngeal space’s deep and challenging exposure. Both CT and MRI scans effectively illustrate the location, size, extent, and nature of the lesion, along with its relationship to the surrounding critical structures, thereby providing essential reference points for treatment planning.
Conclusion
This article delineates the application of an innovative surgical technique, the transnasal endoscopic transpterygoid approach, in the management of a PPA. Literature on this specific surgical method is scant, underscoring the novelty of its implementation in this context.
Footnotes
Author Contributions
Huan Li compiled the patient’s data, reviewed the literature, and wrote the article; Yibin Liu was the patient’s surgeon and provided the patient’s information; Long-Gui You helped perform the analysis with constructive discussions; Xin-Tao Wang was responsible for the review and revision of the article; and Fu-Hua Wang and Hui-huang Liao helped perform the data collection. All authors have given final approval of the submitted version of the article.
Availability of Data and Materials
The data presented in this study are available on request from the corresponding author.
Consent for Publication
A written informed consent was obtained from Guardian of the patient to publish this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
The study was reviewed and approved by the Ethics Committee of Ganzhou People’s Hospital. Guardian of the patient gave their informed consent to participate.