
Abstract
Parapharyngeal abscess in an infant is a very rare condition. We present the case of a 4-month-old girl with large masses on the neck’s left side. Computed tomography showed an extensive parapharyngeal abscess. Left tonsillectomy was performed under general anesthesia from a transoral approach, followed by an incision and evacuation of the abscess from the parapharyngeal space. Microbiological analysis identified a massive occurrence of Streptococcus intermedius.
Case Report
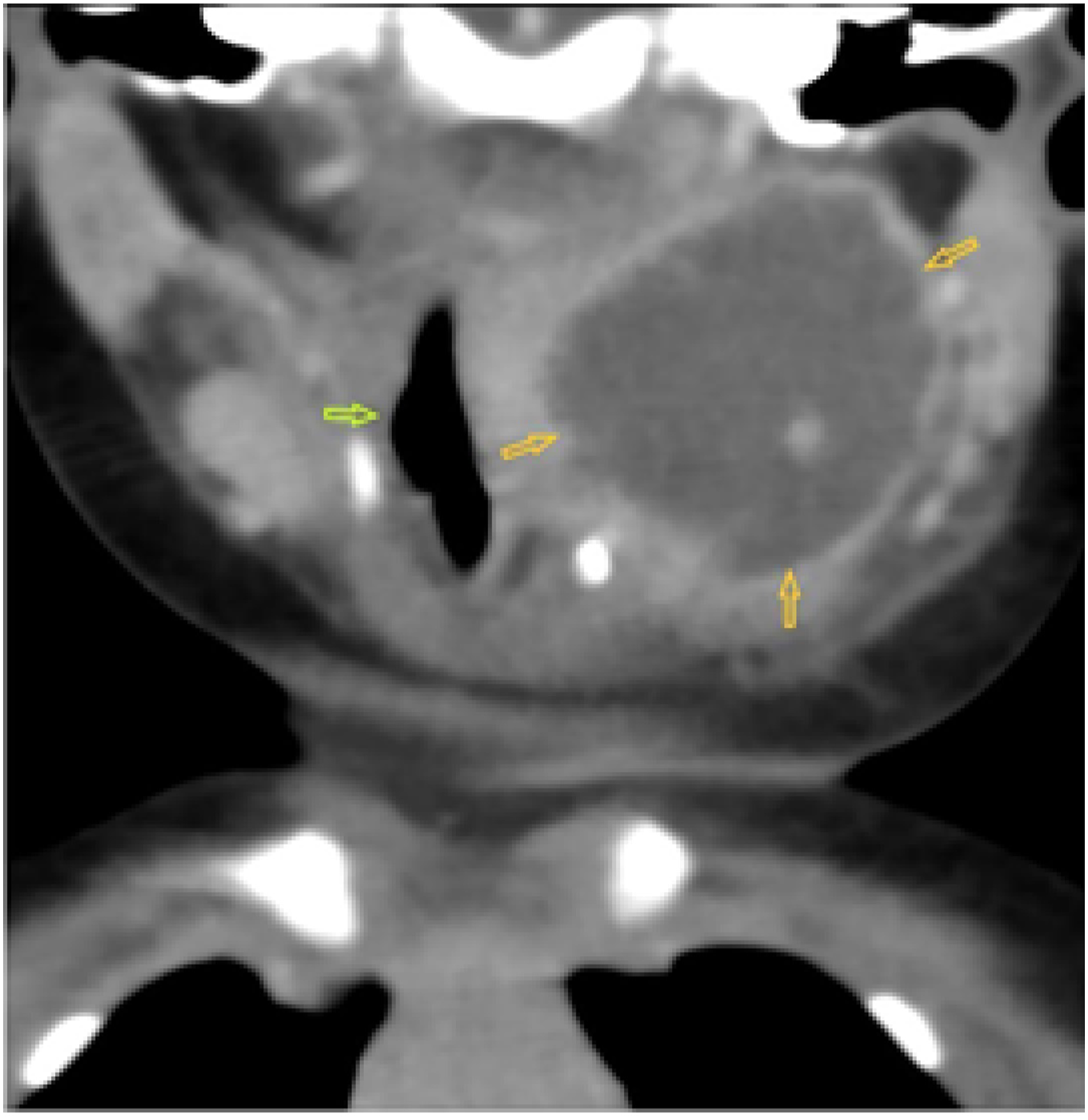
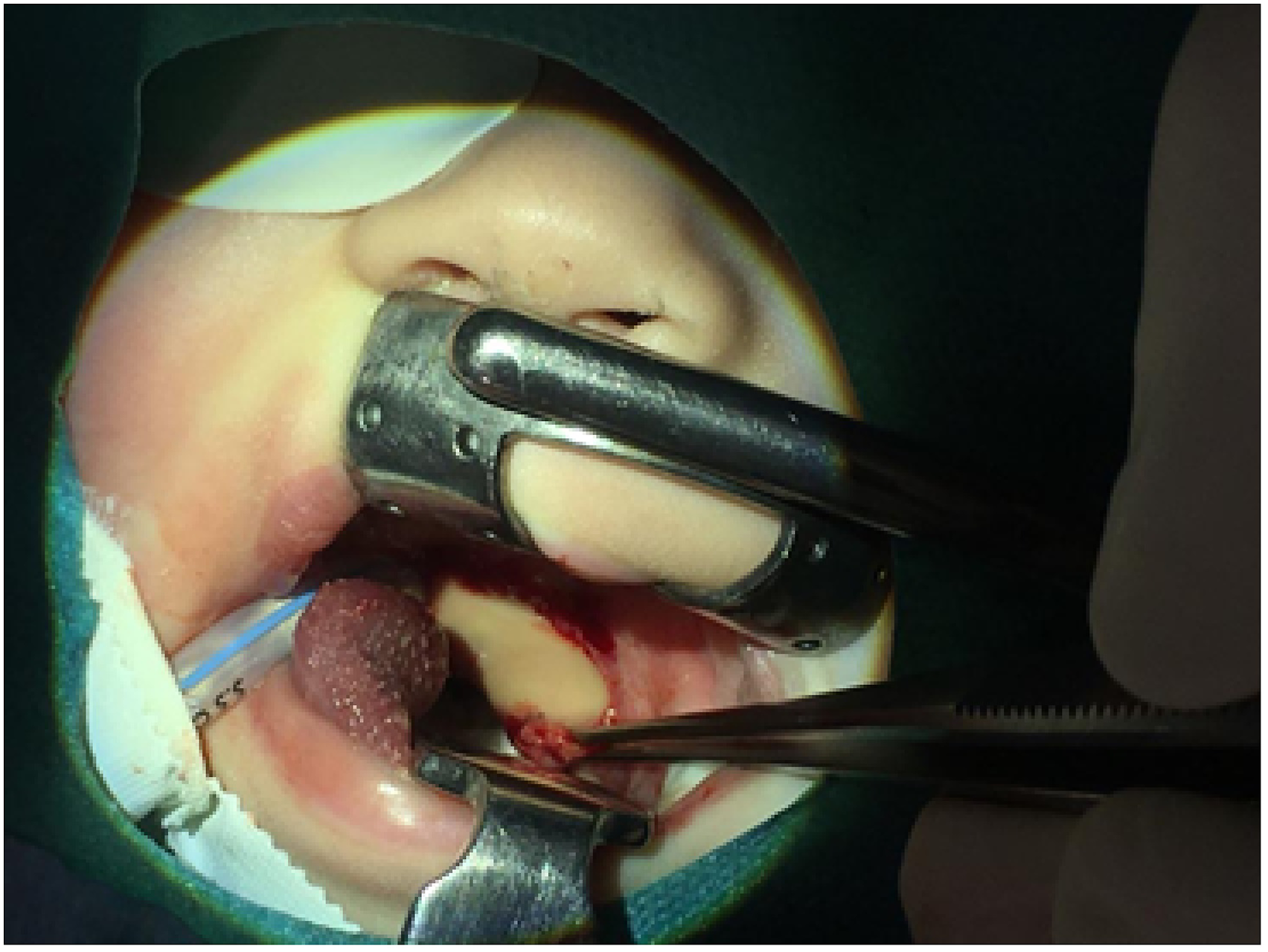
A 4-month-old female infant was referred to the Department of Pediatric Otorhinolaryngology of our tertiary referral hospital for fever, swelling of the neck on the left side, diarrhea, and dysphagia. The child was exhausted and apathetic, her temperature was 37.8°C, and she had ptosis of the left eyelid and hypersalivation. There was mucosal edema of the pharynx, asymmetry of palatal arches, and bulging of the tonsil on the left side. Ultrasonography was performed with suspicion of parapharyngeal abscess. The patient was admitted to the intensive care unit (ICU) and acute computed tomography (CT) of the neck was performed using an intravenous contrast. The CT scan showed an extensive abscess of dimensions 37 mm × 26 mm × 32 mm in the left parapharyngeal space (Figure 1). The carotid sheath was pressed dorsally (Figure 2). Laboratory findings indicated heightened C-reactive protein (42.7 mg/L), leukocytosis (24.3 × 109/l), and thrombocytosis (677 × 109/l). Immediately after CT examination of the neck, a left tonsillectomy was performed under general anesthesia from a transoral approach. This was followed by an incision and evacuation of the abscess from the parapharyngeal space. After the incision, yellow pus flowed out under pressure (Figure 3). The abscess cavity was dilated and then washed with a disinfectant solution. There was no pathology (edema) of the epiglottis. Microbiological analysis of the pus and histology of the tonsil were made. Parapharyngeal abscess, CT scan, axial projection. Parapharyngeal abscess, CT scan, coronal projection. Evacuation of the pus from parapharyngeal space, transoral approach.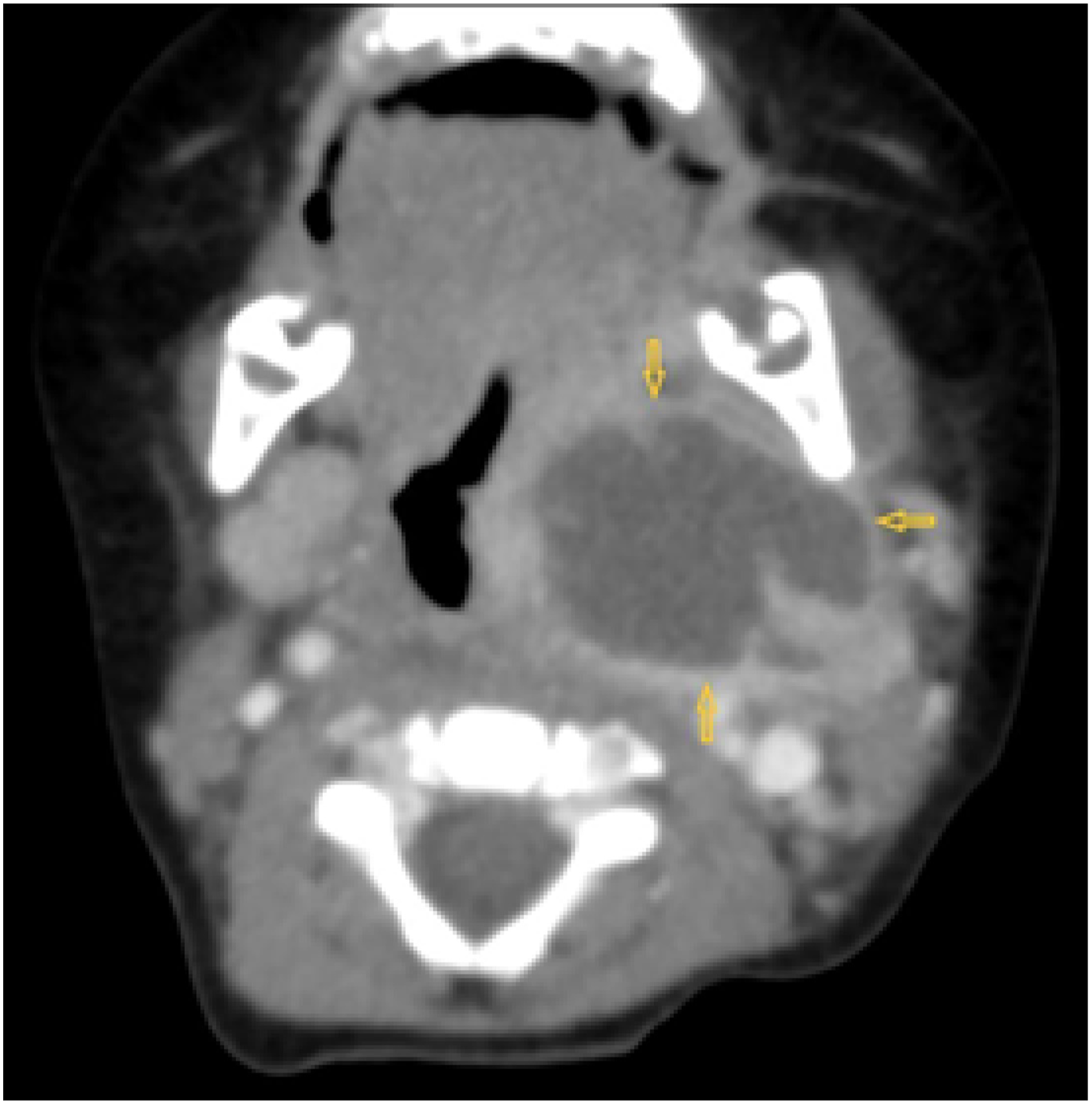
A combination of intravenous antibiotics was administered: clindamycin at dose 70 mg, four times daily, and piperacillin/tazobactam at dose 800 mg, three times daily. Dosages were consulted with the antibiotic center. The condition of the patient improved rapidly after surgery. On the second day after surgery, the patient was afebrile, oral fluid intake was restored, and swelling of the neck was significantly reduced. Microbiological analysis identified a massive occurrence of S. intermedius, sensitive to the established antibiotic treatment. The patient was discharged in good condition on the eighth day after surgery.
Discussion
Parapharyngeal abscess (PFA) is a potentially life-threatening deep neck infection, and it is a very rare pathology in infants. To date, only three cases have been described previously in children under 1 year of age.1-4 In children, the most common causes of PFA are pharyngitis and odontogenic infection, as well as sinusitis, otitis, tonsillitis, mastoiditis, parotitis, or external trauma (penetrating injuries of the neck).3,5,6 In older children, the lymph nodes involve around the parapharyngeal space, and this explains the lower incidence of the disease in these children. 7 The most common complications of PFA include airway obstruction, necrotizing fasciitis, mediastinitis, aspiration pneumonia, thrombophlebitis of the internal jugular vein (Lemierre’s syndrome), carotid artery aneurysm, and sepsis.5,6
Diagnosis of PFA in an infant can be difficult because the clinical signs are highly variable and the pathology is usually not so conspicuous as in adults. Moreover, verbal communication with the patient is greatly limited. The main symptoms include fever, dysphagia, odynophagia, sore throat, swelling of the soft tissues of the neck, hypersalivation, restriction of oral intake, torticollis and/or trismus, and dyspnea.1,2,5,7-9
CT scan with contrast is indicated when PFA is suspected. Some authors prefer magnetic resonance imaging, less often ultrasonography.7,9 CT has high sensitivity but low specificity. It is reported to be able to distinguish formed abscess from cellulite in 89% of cases and is currently considered the standard for diagnosis of PFA.10,11 We prefer CT scan with contrast if PFA is suspected. The abscess on the CT scan with contrast is defined as a low-attenuation formation with a rim enhancement. Proven in our patient was a bounded, low-attenuated fluid formation of 37 mm × 26 mm × 32 mm with rim enhancement and having the character of an abscess.
The therapy involves intravenous administration of broad-spectrum antibiotics and drainage of the abscess.1,5 Antibiotics are initially administered empirically to cover the largest possible spectrum of bacteria, including anaerobes, and we adjust the treatment according to the results from microbiological examination of the pus.
Amoxicillin/clavulanate, clindamycin, or the combination penicillin + metronidazole is recommended for PFAs with origin in the oral cavity. Consultation with an antibiotic center regarding suitable choice of antibiotic and its dose is recommended. 8 In our case, we decided to use clindamycin and piperacillin + tazobactam after consultation with the antibiotic center. We chose this combination of antibiotics due to concern for the possibility of nosocomial infection.
If an inflammatory phlegmon is present and the patient is stable, it is possible to proceed conservatively (antibiotics) and perform a control CT scan within 48 h.5,12,13 The main indications for surgery are airway obstruction, development of other complications, no improvement of clinical state within 48 h after intravenous antibiotic therapy, abscess size >2 cm, age <4 years, and hospitalization in the ICU.12,13 In our case, we decided on acute surgical treatment due to the extent of the finding, symptoms, age, and general state.
The surgical approach is external or transoral. The external approach poses a greater risk of injury to the nerve-vascular bundle. The transoral approach is less risky and less invasive, reducing the length of hospitalization and associated costs of treatment. In some cases, such as severe trismus or abscess located laterally to large vessels, the external approach remains the method of choice. A combined approach can also be chosen in case of massive abscess.9,10,13 The transoral approach worked well in our case.
Microbiological analysis will usually detect a mixed flora, most often Streptococcus pyogenes, S. Aureus, and/or S. viridans.10,14 S. intermedius was detected in our patient. Although this is a flora commonly occurring in the oral cavity and urogenital tract,12,15 S. intermedius can be a potential cause of severe infections, especially in cases of brain and liver abscesses or empyema of the chest. 15
Due to this unusual finding in the patient, we considered the possible presence of inborn error of immunity. 16 We planned to investigate at least basic immune parameters, such as immunoglobulin levels and functional immunoassays, and to examine T-cell receptor excision circles (TRECs) and kappa-deleting recombination excision circles (KRECs), despite that interpretation of these tests could be questionable at this age. The parents did not want further investigation, however, and still do not. The patient is currently 11 months old and doing well. We have recorded no repeated, prolonged, or atypical course of infections. We accordingly conclude that the immune parameters are normal in this patient, but we cannot wholly rule out a potential presence of inborn error of immunity of some type.
Conclusion
Parapharyngeal abscess in children under 1 year of age is an extremely rare and life-threatening pathology. The diagnosis can be difficult because the symptoms are usually nonspecific. Imaging plays an important role in diagnosis, and CT scan using intravenous contrast is preferred. Early surgical intervention with evacuation of pus and drainage of the abscess cavity is indicated. PFAs are most commonly mixed-flora infections, so intravenous broad-spectrum antibiotics constitute an important part of treatment.
Footnotes
Author Contributions
All authors declare that they participated in the preparation of this study. Supervision: MU; design: BP; resources: BP; materials: MU and MB; data collection and/or processing: BP and EK; analysis and/or interpretation: BP, MU, and PJ; literature search: BP and EK; writing manuscript: BP and MU; and critical review: MU, JJ, SŠ, and PJ.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Health, Czech Republic, Conceptual Development of Research Organization (FNBr, 65269705) and by project of Masaryk University Brno MUNI/A/1118/2020.
Ethical approval
The study was approved by Ethical Committee of University Hospital in Brno, number of protocol: 12-1402121/EK.