
Abstract
Objective
The purpose of this study was to evaluate the diagnosis circumstances, predisposing factors, investigations, and therapeutic management of retropharyngeal and parapharyngeal abscesses.
Methods
A retrospective chart review of patients diagnosed with retropharyngeal or parapharyngeal abscess from 2001 to 2021 was performed. Epidemiological characteristics, clinical signs, investigations, medical treatment, and surgical interventions were analyzed for each patient.
Results
A total of 30 patients with retropharyngeal or parapharyngeal abscess were identified. Computed tomography was performed in all cases, and magnetic resonance imaging was performed in three cases. Twelve patients had a “pure” retropharyngeal abscess, nine patients had a prestyloid abscess, one patient had a prestyloid abscess associated with a peritonsillar abscess, three patients had a retrostyloid abscess, and five patients had a prestyloid abscess associated with a retropharyngeal abscess or a retrostyloid abscess. The median long axis of the abscess was 42 cm. All patients received intravenous antibiotics for a median period of 8 days [4–30]. Seventeen patients required surgical trans-cervical drainage. Other patients underwent transoral or transnasal drainage. The pus culture revealed no growth in six cases, streptococcus (four cases), methicillin-sensitive Staphylococcus aureus (two cases), Klebsiella (two cases), Enterobacter (one case), Fungi (two cases), and Mycobacterium tuberculosis (a twelve-year-old boy). It was not documented in twelve cases. Histological examination revealed caseofollicular tuberculosis in a 53-year-old man. In 25 patients, no adverse events were observed during follow-up. Five patients had an unfavorable outcome.
Conclusion
We have found an increase in the incidence of these infections in recent years. Computed tomography is the best imaging examination for the diagnosis and follow-up of retropharyngeal and parapharyngeal abscess. Early drainage and antimicrobial therapy are essential for rapid recovery and prevention of complications of these abscesses.
Introduction
Peritonsillar, retropharyngeal (RPA), and parapharyngeal abscesses (PPA) are deep neck infections that are usually secondary to contiguous spread from local sites. 1
Proper diagnosis and treatment of these deep neck space abscesses are essential to prevent airway compromise. 2
The protection of the airway and broad-spectrum intravenous antibiotic therapy are recognized cornerstones of treatment. 3
This retrospective study of 30 patients was designed to evaluate the circumstances of diagnosis, predisposing factors, investigations, and therapeutic management of retropharyngeal and parapharyngeal abscesses.
Methods
A retrospective chart review of patients diagnosed with retropharyngeal or parapharyngeal abscess from January 2001 to December 2021 was performed.
The positive diagnosis of these abscesses was made based on clinical symptoms, physical examination, laboratory tests, and results of contrast-enhanced computerized tomography (CT) or magnetic resonance imaging (MRI).
Criteria for determining an abscess were low density, the presence of air or low-attenuation fluid, and enhancement of the rim. In this study, we included only abscesses confirmed by pus drainage by surgery or aspiration.
Epidemiological characteristics, clinical signs, investigations, medical treatment, and surgical interventions were analyzed for each patient.
All variables including baseline characteristics were presented as a number with a percentage for categorical variables, mean ± standard deviation for continuous variables following a normal distribution, and median with extreme values for continuous variables not following a normal distribution. Normal distribution was tested with the Shapiro–Wilk test.
Results
During a 20-year study period, 30 patients, including 20 men and 10 women, with a median age of 28 years [ 3 months, 67 years] were hospitalized in the ENT and Head and Neck Surgery Department for retropharyngeal or parapharyngeal abscess. The incidence of the disease has increased in recent years, reaching a peak frequency in 2014 and 2016 (five cases per year).
Clinical presentation
Summary of clinical symptoms according to the location of the abscess.
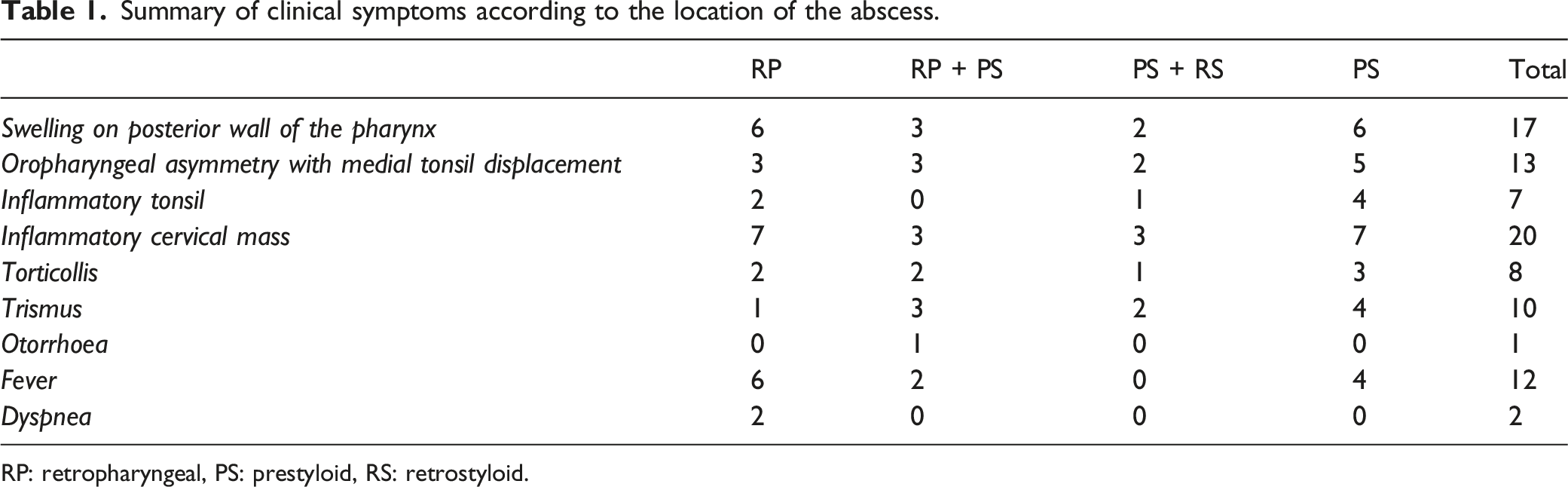
RP: retropharyngeal, PS: prestyloid, RS: retrostyloid.
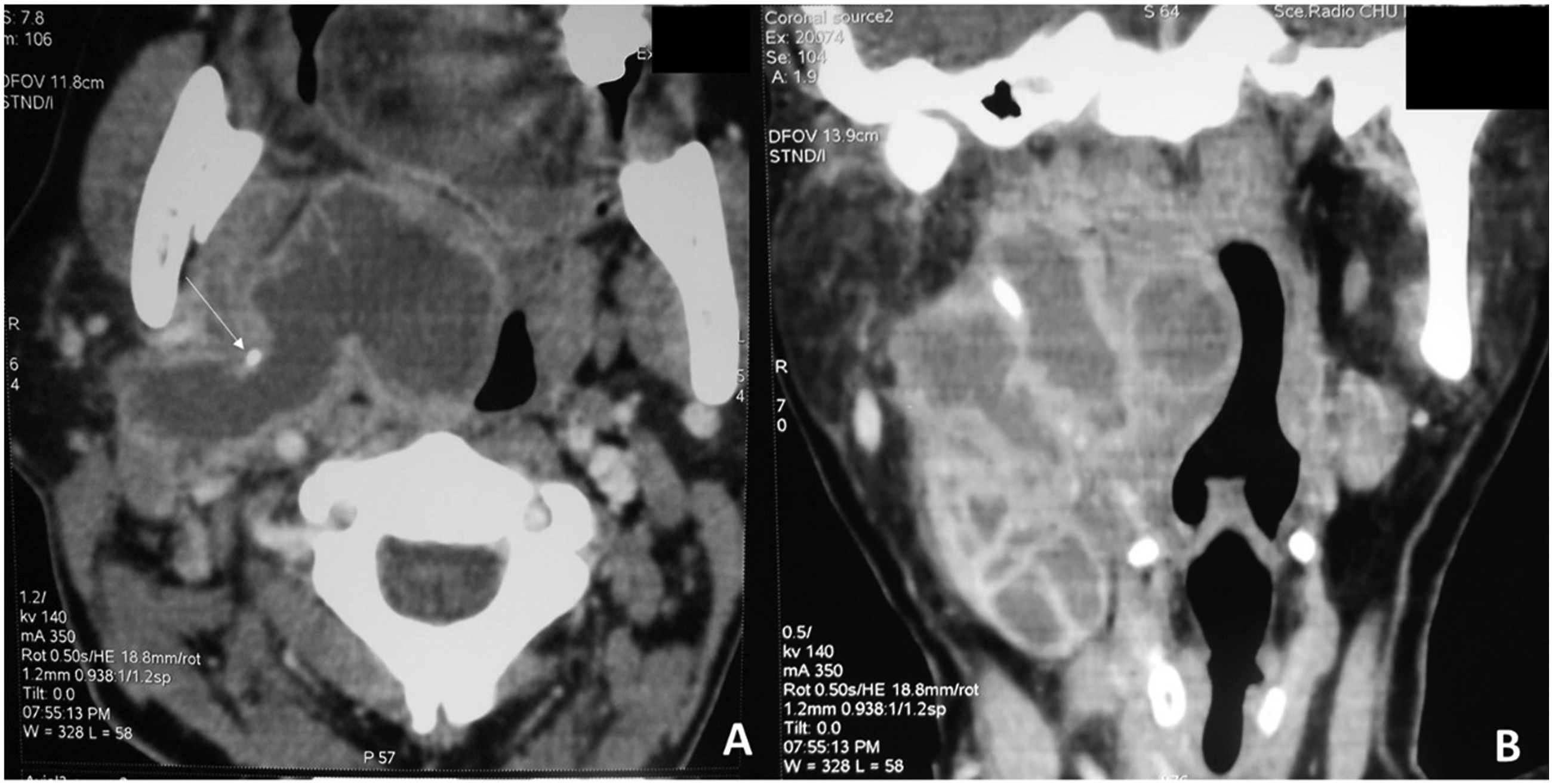
An oropharyngeal asymmetry with medial tonsil displacement was found in 17 patients. A painful lateral cervical mass was found in nineteen patients and one patient presented a 3 cm inflammatory retromandibular swelling (Figure 1A). A 38-year-old woman treated for nasopharyngeal cancer. Contrast-enhanced axial (A) and coronal (B) CT scan shows an upper prestyloid parapharyngeal abscess. The follow-up imaging (C) performed 1 month after the transnasal endoscopic approach shows the residual cavity.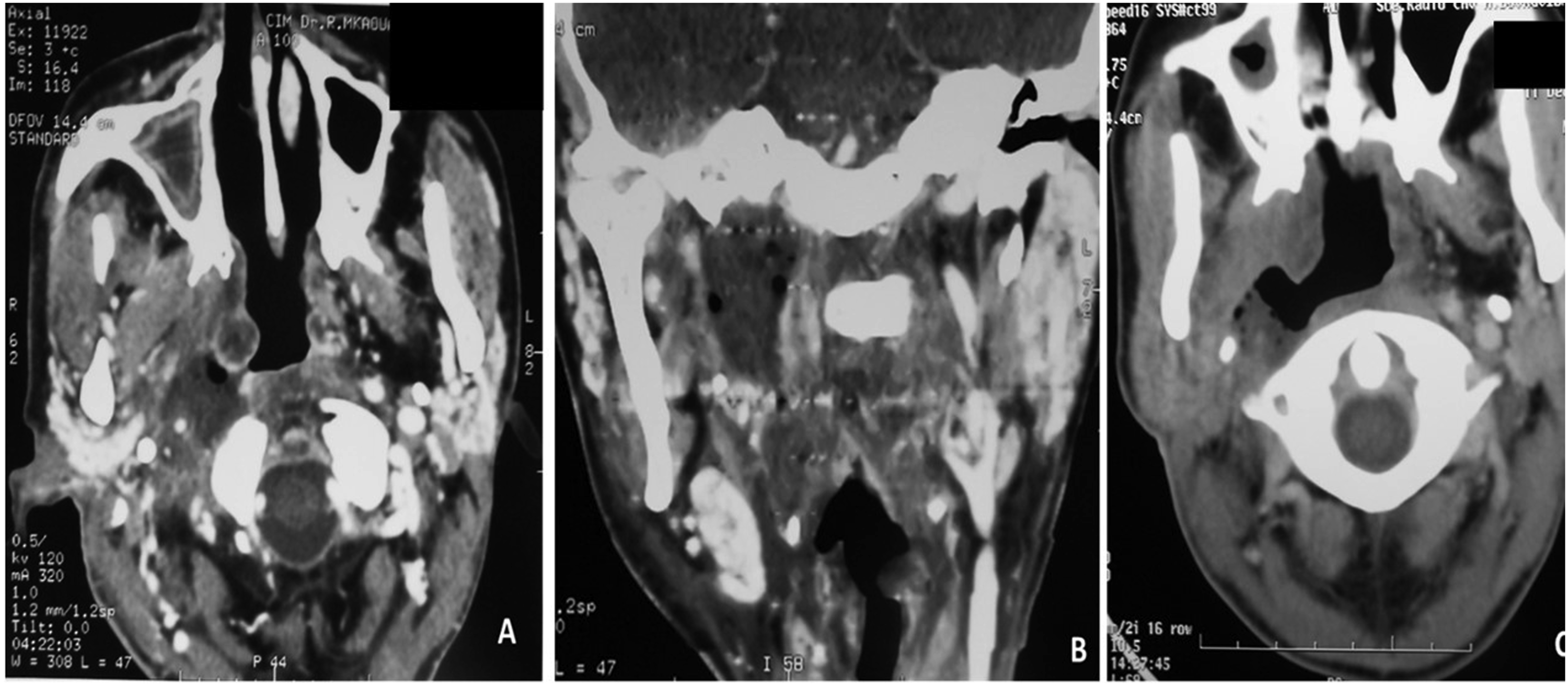
Fever was present in 12 patients and was higher than 39°C with a maximum of 40.5°C.
Medical history
Five patients had diabetes mellitus. None had a history of “tonsillar abscess.” One patient had a history of radiochemotherapy-treated nasopharyngeal carcinoma that ended three months before hospitalization.
Previous history and predisposing factors
RPA and PPA complicated pharyngitis in eighteen patients and dental abscess in one patient. A patient reported swallowing a fish bone six days prior to presentation. Before hospitalization, two patients received corticosteroids and seven patients received non-steroidal anti-inflammatory drugs.
Twenty patients received oral antibiotics before diagnosis.
Biology
Laboratory findings revealed moderate leukocytosis with a mean of 18363+/-8003 cells/microliter and a mean C-reactive protein of 123+/-79 milligrams/l.
Imaging
The computed tomography (CT) scan with contrast was the initial imaging modality for all patients. Three patients had gadolinium-enhanced magnetic resonance imaging. Imaging confirmed the diagnosis of clinically suspected RPA and PPA.
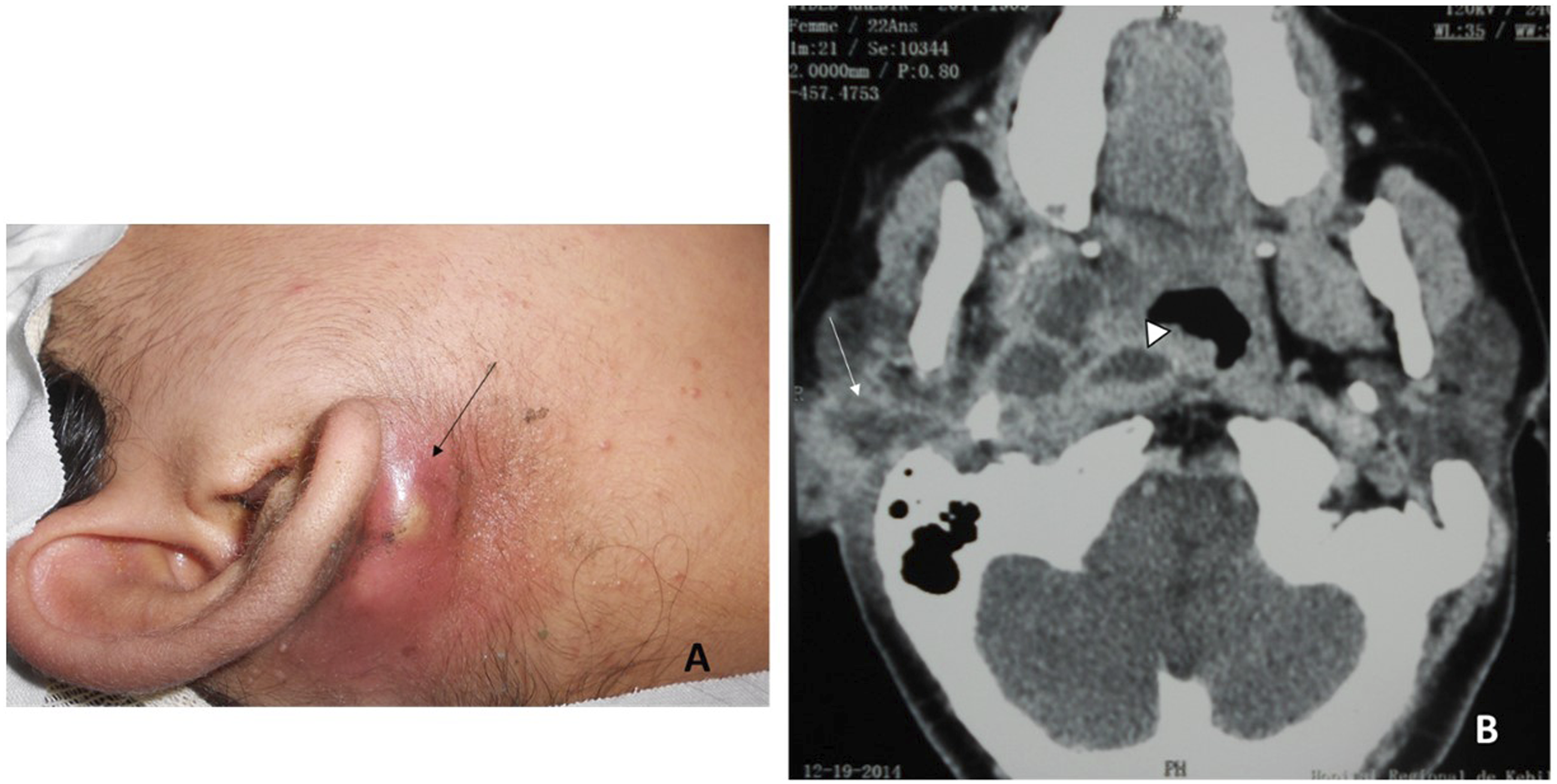
Twelve patients had an isolated retropharyngeal abscess, nine patients had a prestyloid abscess (Figure 1, Figure 2), one patient had a prestyloid abscess associated with a peritonsillar abscess, three patients had a retrostyloid abscess, and five patients had a prestyloid abscess associated with a retropharyngeal abscess (Figure 3) or a retrostyloid abscess (Figure 4). The median long axis of the abscess was 42 cm [1.5–100 cm] A 53-year-old man with a prestyloid abscess operated through an external approach. Preoperative MRI examination shows a prestyloid parapharyngeal abscess. Rim enhancement on T1 plane (A) and hyperintense collection on T2 coronal plane (B). Final diagnosis on histological examination: tuberculosis A 22-year-old patient who has a prestyloid space abscess with the involvement of retropharyngeal space (arrowhead). Note the external retro mandibular abscess (arrow). (A) Clinical appearance. (B) CT scan demonstrating collections involving the lateral pharyngeal space, retropharyngeal, and retro mandibular inflammatory collection(arrow). The patient was operated through an external approach. Preoperative axial (A) and coronal (B) CT scans show a voluminous prestyloid abscess extended to the poststyloid compartment (arrow: styloid process).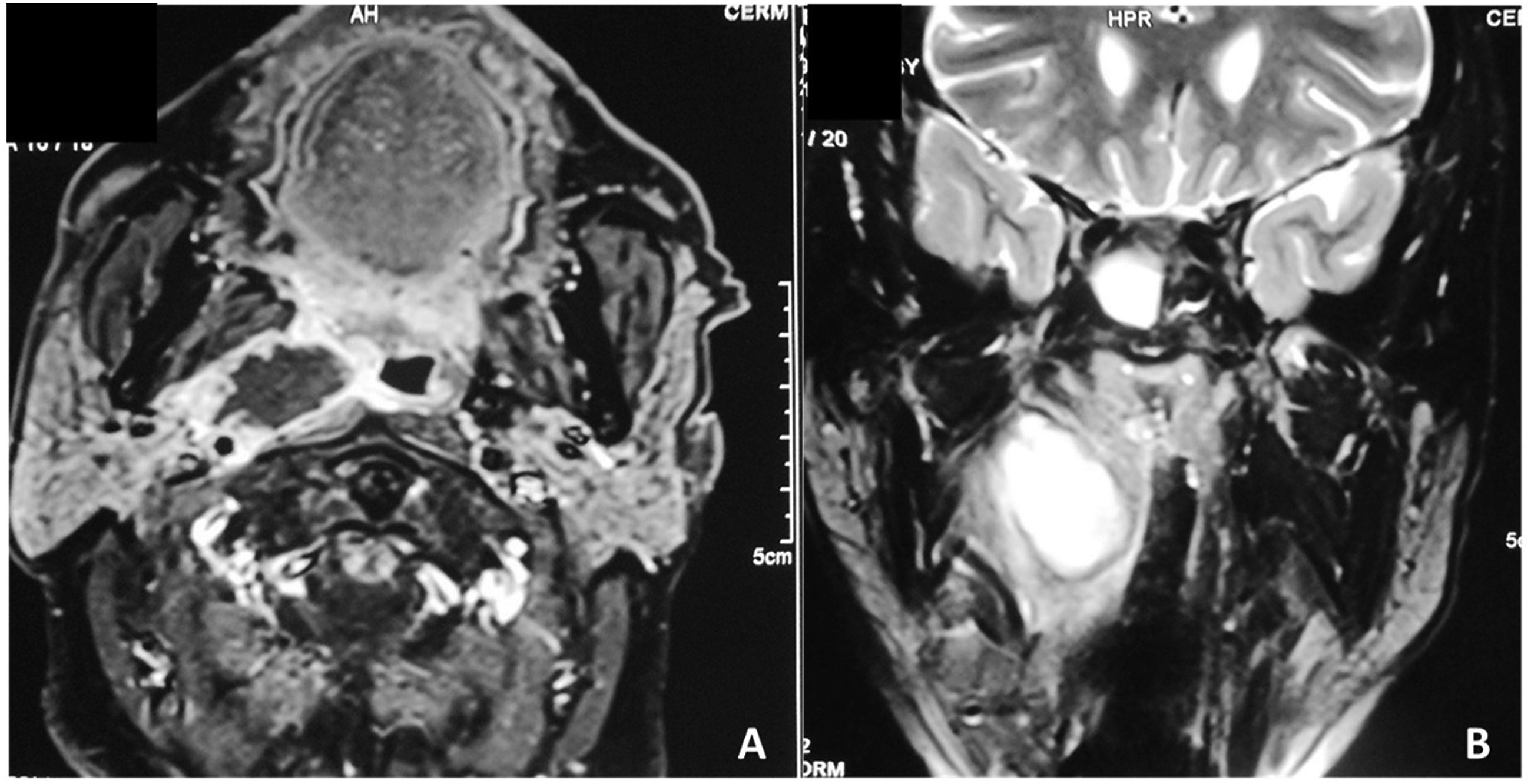
Medical management
All patients received intravenous antibiotics for a median period of 10 days [ 3–30 days]. Ten patients were treated with amoxicillin + clavulanic acid (6 g per day or 150 mg/kg for children under 15 years of age). Other patients received different antibiotics (cefotaxime + imidazole).
Abscess drainage
Seventeen patients underwent trans-cervical drainage with a histological sample from the margin of the abscess: via an exclusive cervical incision for fourteen patients and via a combined cervical and transoral approach for three patients.
Twelve patients underwent transoral needle aspiration drainage or an intraoral surgical approach (RP abscesses). Four patients underwent immediate tonsillectomy and drainage of the abscess through the tonsil.
One patient (nasopharyngeal abscess) also had nasal endoscopic drainage.
No patient required a tracheostomy.
Bacteriology
Blood culture was performed on 12 patients and was negative.
Pus culture revealed no growth in six cases, streptococcus in four cases, methicillin-sensitive Staphylococcus aureus in two cases, Klebsiella pneumoniae in two cases, Enterobacter in one case, Candida albicans in two cases, Mycobacterium tuberculosis in one case (a twelve-year-old boy), and polymicrobial growth in twelve cases.
Histological examination revealed caseofollicular tuberculosis in a 53-year-old man.
Patients with tuberculosis did not have tuberculous involvement of the cervical spine.
Outcomes and complications
In 25 patients, no recurrence or complication was observed during follow-up. The mean total duration of antibiotic therapy (parenteral and oral) was 24 days (range: 11–60 days). The median duration of oral antibiotics was 14 days (7–30 days).
Two patients with tuberculous abscess received a six-month antituberculosis treatment regimen and did not have a recurrence.
Five of the thirty treated patients had an unfavorable outcome: − A three-month-old baby presented a recurrence of a retropharyngeal abscess 7 months after the initial treatment. − A woman with a recurrent abscess requiring repeated punctures followed by external drainage died from generalized sepsis during hospitalization. − A woman treated for nasopharyngeal cancer presented, 2 months after drainage, and had massive epistaxis followed by immediate death. − A 45-year-old man died in the intensive care department after cervical drainage of a retropharyngeal abscess complicated by spinal compression and quadriplegia. − A 66-year-old diabetic man presented mediastinitis 9 days after surgical drainage of a retropharyngeal abscess, secondarily complicated by pulmonary embolism during his stay in the intensive care unit.
Discussion
Spaces
The parapharyngeal space is an inverted cone-shaped potential space that extends from the skull base to the hyoid bone. 3 Its lateral boundaries are the medial pterygoid muscle, the medial face of the ramus of the mandible, the deep lobe of the parotid gland, and the posterior belly of the digastric muscle. Its medial borders are the buccopharyngeal and alar fascia, while the posterior boundary is the posterior layer of the carotid. 4
The styloid process and its attached structures divide the lateral pharyngeal space into two compartments: anterior or prestyloid and posterior or poststyloid. The anterior compartment contains fat and connective tissue, whereas the posterior compartment contains cranial nerves IX, X, XII, the cervical sympathetic chain, the internal jugular vein, and the carotid artery. 3
The alar fascia separates the parapharyngeal space from the retropharyngeal space, which extends from the skull base to the mediastinum. 4
The retropharyngeal space extends longitudinally downward from the base of the skull to the posterior mediastinum. The posterior border is the prevertebral fascia, and the anterior boundary is the posterior portion of the pretracheal fascia. 4 Retropharyngeal space infections are the most dangerous deep neck infections. This is due to the rapidity of the potential spread to the mediastinum and the resultant morbidity. 2
Microbiology
Most oropharyngeal abscesses are polymicrobial infections and reflect oropharyngeal flora; the average number of isolates is 5 (range: 1–10).5,6
In the pre-antibiotic era, the most common organism associated with deep neck infections was Staphylococcus aureus. 3
The predominant anaerobic organisms isolated in parapharyngeal abscesses are Fusobacterium, Prevotella, Peptostreptococcus spp, and Porphyromonas; aerobic organisms are streptococcus of group A (Streptococcus pyogenes), Staphylococcus aureus, and Haemophilus influenza.4,5,7
Anaerobic bacteria can be isolated from most abscesses when appropriate techniques for their cultivation have been used.5,7
Brook studied 14 children with retropharyngeal abscesses; all produced bacterial growth. Anaerobes were isolated in all patients; they were the only isolates in two patients (14%) and mixed with aerobes in twelve (86%), with alpha and gamma hemolytic streptococci, S. aureus, Haemophilus influenza, and hemolytic streptococci of group A being the predominant aerobes. 8
According to data published by Hoffman et al., polymicrobial cultures were found in 3 out of the 35 positive cultures, whereas no bacterial growth was observed in 22 cases. 9 On the other hand, in a study led by Klug, pus cultures were polymicrobial in 93% of the cases and no negative cultures were reported. 10 In the present study, no bacterial growth was observed in 6 out of 30 patients. This is probably due to the use of high-dose antimicrobials early at the beginning of the disease.
The antibiotic spectrum should cover both Gram-positive and Gram-negative, and aerobic and anaerobic pathogens.2,11
Yang found that 10 of the 174 isolates from 89 deep neck abscesses were β-lactamase-producing strains producing-lactamase (5.8%). These strains were staphylococcus aureus, staphylococcus coagulase negative, and Fusobacterium nucleatum. 12
The production of β-lactamase would protect not only the β-lactamase producing bacteria but also the β-lactamase nonproducing bacteria from β-lactam antibiotics.
A tuberculous retropharyngeal abscess is rare and is generally secondary to tuberculous involvement of the cervical spine. In rare cases, the abscess may be due to hematogenous spread from pulmonary tuberculosis. 13 The patients presenting tuberculosis were not having tuberculous involvement of the cervical spine.
Clinical diagnosis
Retropharyngeal infection occurs most frequently in children younger than 5 years of age. It has been postulated that young children are more likely to develop infections in this area due to the presence of lymph nodes (Rouviere nodes) that run in a paramedian chain in the retropharyngeal space and spontaneously regress after 5 years. 1
Yang et al. found an annual incidence rate of PPA and RPA of 2.43–3.17 per 100,000 adult people during 2007–2016, which was higher than similar population-based studies. 14 The difference in the incidence of this infection may be due to age groups, geographic regions, ethnicities, and/or lifestyles. We have found an increase in the incidence of these infections in recent years. A larger multicenter study is needed to evaluate the incidence of this infection.
Predisposing factors such as dental problems, dental interventions, upper respiratory infections, recent surgery, or trauma need to be evaluated.2,7
In a study that included 64 patients with deep neck abscesses performed by Sethi et al., the cause of infection remained unknown in 39% of cases, was caused by a dental infection in 31% of cases, and by foreign bodies in 27% of cases. 15
The primary symptoms of these deep neck collections are fever, sore throat, dysphagia, swelling, and trismus.2,7 Sànchez reported odynophagia in 69% of the cases, fever in 60%, pharyngeal wall bulging in 54%, palpable lymphadenopathy in 15%, and trismus in 12%. Other signs mentioned in his study were halitosis, torticollis, and dyspnea. 7
Parapharyngeal and retropharyngeal abscesses are important causes of morbidity and mortality due to potential complications, including laryngeal obstruction with acute respiratory distress, internal jugular vein thrombophlebitis with septicemia (Lemierre syndrome), and spread of infection to the mediastinum. 16
Medical imaging
When a deep neck infection is suspected, contrast-enhanced CT or magnetic resonance imaging is recommended to accurately assess the extent of the injury and differentiate an abscess from cellulitis.17,18 Contrast-enhanced CT is preferred because it is generally available, less expensive, and allows rapid acquisition of diagnostic images. 18
Although CT helps determine both the presence and location of neck infections in children, it is less helpful in differentiating abscesses from lymphadenitis, cellulitis, and some complex cervical masses. 18 The abscess appears as a low-attenuation fluid collection that distends the deep space of the neck with peripheral enhancement.
The CT scan provides details of the size, location, and relationships of the abscess with large vessels, and other deep spaces of the neck. 7
In the evaluation of deep neck infections, false-positive computed tomography scans emphasize the importance of correlating radiological interpretation with clinical examination before surgical intervention. In fact, in a comparative study led by Eissa, the precision in identifying a drainable collection of physical examination alone and CT scan alone were, respectively, 63% and 77%, the sensitivities were 55% and 95%, and the specificities were 73% and 53%. When physical examination and CT scan findings were associated, the precision in identifying a drainable collection reached 89%, the sensitivity 95%, and the specificity 80%. 18
Imaging is also useful for assessing potential complications such as inferior extension into the mediastinum; compromised airway, internal jugular vein thrombosis, and pseudoaneurysm formation. 18
MRI is superior in imaging soft tissue masses compared to CT and is strongly recommended today in children to diminish radiation.17,18
CT-guided percutaneous aspiration is both a diagnostic modality that confirms abscess formation of an inflammatory lesion of the retropharyngeal space and a therapeutic tool, sometimes avoiding the need for surgical drainage. 19
The CT-guided aspiration of the retropharyngeal abscess is performed using a retromandibular approach. A twelve-gauge needle is inserted through the mastoid-mandibular angle, flush with the outer cortex of the mandible, then passes through the retrostyloid space, anteriorly to the carotid artery, to reach the retropharyngeal space. 19
Duque and Guerra described the use of ultrasound to guide percutaneous aspiration or identify collection during surgical exploration of parapharyngeal space abscesses in children. 20
Medical therapy
Treatment should be started within the first 24 to 48 hours after the onset of pain, when the infection is in the cellulitis stage. 1
Yang and Lee studied five different combinations of empiric antibiotics for deep neck infection, namely, regimen 1: penicillin G and clindamycin and gentamicin, regimen 2: ceftriaxone and clindamycin, regimen 3: ceftriaxone and metronidazole, regimen 4: cefuroxime and clindamycin, and regimen 5: penicillin and metronidazole. 12 The authors compared these regimens using the antimicrobial susceptibility of 89 patients. They found that the coverage rates for regimens 1, 2, 3, 4, and 5 were 67.4%, 76.4%, 70.8%, 61.8%, and 16.9%, respectively. Recently, Huang suggested amoxicillin clavulanic acid alone, or third-generation cephalosporins, alone or in combination with metronidazole, as first-line treatment. 11
When it is decided to treat the patient with antibiotics alone, follow-up imaging should be performed in the absence of improvement 24 to 48 hours after starting antibiotics. 19
The 2008 guidelines of the French Society of ENT (SFORL) recommend first-line drug treatment of retropharyngeal abscess, except in the presence of complications or when the abscess is larger than 1.5 cm in diameter. 21
Elden found that increased surgical drainage in children under 15 months of age (p = 0.002) and for abscesses >2.2 cm (p = 0.0001). 22
Abscess drainage
Several approaches are available, and their use depends on the site and the extension of the infection.7,9 In our series, all patients were treated with emergency surgical drainage or repeated aspirations. The surgical approach is not standardized.2,3
An intraoral approach to the parapharyngeal space could be discouraged due to the presence of the carotid sheath within the space. 23 Thus, abscess drainage is generally performed externally. 3
For Sakr, posterior abscesses are drained externally through the submaxillary fossa, whereas anterior abscesses can often be drained through an intraoral incision. 16 Therefore, due to functional and aesthetic considerations, other authors prefer intraoral drainage with immediate tonsillectomy for anterior PPA. 23
The drainage of the retropharyngeal space can be accomplished by an intraoral or external approach. 3 Intraoral approach has now been established as the preferred route, and cervicotomy is reserved for abscesses that extend laterally to the great vessels or inferiorly to the mediastinum. 9
Nocolai reported the use of a transnasal endoscopic approach in two patients with retropharyngeal abscesses located in the cranial portion of the retropharyngeal space. 24 This approach is associated with low morbidity and requires a short hospitalization time. In our series, we adopted this approach for a patient with a superior parapharyngeal abscess.
Surgical drainage carries its inherent risks and potential complications. Therefore, percutaneous imaging-guided aspiration (under US or CT guidance) has been suggested as an alternative to conventional surgery. 16
The use of imaging-guided aspiration is an alternative to external drainage of deep neck abscesses essentially in elderly and debilitated patients. Yeow et al. described 15 patients with deep neck abscesses treated successfully with US-guided aspiration and catheter placement. There were no complications in their study. 25
Airway management is the initial and ongoing clinical imperative. Therefore, equipment for intubation cricothyroidotomy or tracheotomy should be available.2,5,7
The limitations of this study include its retrospective and uncontrolled design and the lack of standardized documentation relating to the physical findings. Therefore, some data from physical examinations were missing. However, there were no standard criteria for documenting CT scan interpretations or a standard protocol. We restricted our study to patients who had RPA or PPA confirmed by pus drainage through surgery or aspiration. We presented rare cases of large abscesses extended to more than one space and two acute presentations of tuberculous PPA and RPA.
Conclusion
Retropharyngeal and parapharyngeal abscesses present a challenge in diagnosis and management. We have found an increase in the incidence of these infections in recent years. The CT scan is the best imaging examination for the diagnosis and follow-up of retropharyngeal and parapharyngeal abscesses. Furthermore, early surgical drainage and antimicrobial therapy are essential for rapid recovery and prevention of complications of these abscesses.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest concerning the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Ethics Committee of the University Hospital (number: 7/2022).
Informed Consent
Written informed consent for the publication of data and images was obtained from the patients or the legally authorized representatives.
Data availability statements
All data generated or analyzed during this study are included in this article. Further inquiries can be directed to the corresponding author.