
Abstract
Introduction
Myringoplasty is currently the gold standard for the treatment of chronic tympanic membrane (TM) perforations. However, challenges remain in repairing large perforations, which have a lower success rate due to poor vascularization, inadequate TM remnants, and poor stabilization. 1 Raising the tympanomeatal flap may improve the graft success rate, but it can result in damage to the chorda tympani, stenosis of the external auditory canal (EAC), iatrogenic cholesteatoma, slow healing, and longer operation times. 2,3 Although the push-through technique without a tympanomeatal flap has gradually gained popularity, 4 –6 it has not been widely used to repair large marginal perforations.
Some scholars have used cartilage-reinforced temporalis fascia or perichondrium to improve the graft success rate. 1,7,8 Kolethekkat et al 7 found that a cartilage rim-augmented fascia group had a higher graft success rate compared with a temporalis fascia alone group (94.7% vs 70%). Similarly, Tek et al 8 found that cartilage reinforcement tympanoplasty had a significantly higher success rate compared with temporalis fascia (100% vs 66%). Additionally, Shakya et al 1 compared single and double perichondrium reinforcement cartilage techniques and found no difference in graft outcomes (95% vs 95%). However, these techniques, similar to the double underlay technique, have their limitations, as the procedure is complicated for beginners. Our previous study showed that perichondrium overlaying the squamous epithelium did not increase the risk of iatrogenic cholesteatoma. 9,10 Furthermore, Kolethekkat et al 7 demonstrated that cartilage rim-augmented fascia tympanoplasty did not affect postoperative hearing improvement if the ossicular chain was not damaged. Based on this, we designed an endoscopic cartilage reinforcement technique to treat large marginal perforations. In this study, we compared the graft success rate and hearing outcomes of endoscopic cartilage reinforcement perichondrium-cartilage composite graft and push-through techniques for the treatment of large marginal perforations.
Material and Methods
Ethical Considerations
The study protocol was reviewed and approved by the Institutional Ethical Review Board of Shanghai Sixth People’s Hospital Affiliated to Shanghai Jiao Tong University School of Medicine. All participants provided written informed consent.
Patient Selection
Subjects were recruited from consecutive adult patients diagnosed with large chronic perforations and dry ears for > 3 months between May 2020 and May 2021. Prior to enrollment, CT scans were performed, and audiograms were recorded for all patients. Exclusion criteria included revision cases, poor pneumatization of the middle ear and mastoid, ossicular chain abnormalities, and fungal otitis externa. The following data were recorded: age, sex, side, duration, myringosclerosis, smoking status, and diabetes. Subjects were assessed using standard pure-tone audiometry at frequencies of 0.5, 1, 2, and 4 kHz, both preoperatively and at 6 months after surgery. We calculated the air-bone gap (ABG) as the average difference between air and bone conduction at each frequency. Ossicular chain disruption was suspected when the preoperative ABG exceeded 40 dB; these subjects were excluded from the study.
Randomization and Blinding
All patients underwent endoscopic cartilage myringoplasty. The graft technique allocation was performed by the principal investigator, with the aid of a registered operating room nurse, using simple random sampling. Specifically, consecutive subjects who met the inclusion criteria and signed the consent form were assigned random numbers generated by the SPSS for Windows software package (ver. 20.0; SPSS, Inc., Chicago, IL, USA) and allocated to the cartilage reinforcement group or push-through group. Neither technique involved tympanomeatal flaps. In the cartilage reinforcement group, small pieces of cartilage were overlaid on the epithelial layer of perforation rims to reinforce the cartilage-perichondrium graft.
Surgical Approach
De-Epithelialization of Perforation Margins
All myringoplasties without raising tympanomeatal flaps were performed endoscopically under general anesthesia by the same surgeon. A single-layer perichondrium-cartilage composite graft was harvested from the ipsilateral tragus. The perforation margins were refreshed, and the epithelium of the manubrium was removed. The graft was supported medially and laterally by biodegradable NasoPore (Stryker Canada, Hamilton, ON, Canada) in both groups.
Cartilage Reinforcement Group
The lateral perichondrium was elevated circumferentially around the cartilage graft, but the pedicle remained attached to the center of the graft. Cartilage was removed peripherally according to the size of the perforation in an annular fashion, making the cartilage graft at least 1 mm larger than the circumferential perforation margins. A notch was created in the cartilage graft to accommodate the malleus handle, if necessary. Excess pieces of cartilage were retained to reinforce the graft. The perichondrium graft was also trimmed peripherally and should be approximately 2 mm larger than the cartilage graft.
The perichondrium and cartilage graft were placed trans-perforation; the cartilage graft was positioned medial to the remnant TM and the annulus, with a notch in the cartilage accommodating the malleus handle if necessary. The perichondrium graft was placed medial to the remnant TM and the annulus but lateral to the cartilage and malleus handle. If there was a gap between the perichondrium graft and perforation margin, excess free perichondrial grafts were placed therein to create a continuous surface between the graft and TM remnant. Then, small pieces of cartilage were overlaid on the epithelial layer of the margin of the graft and the remnant TM to augment the margins (Figures 1A and 2).
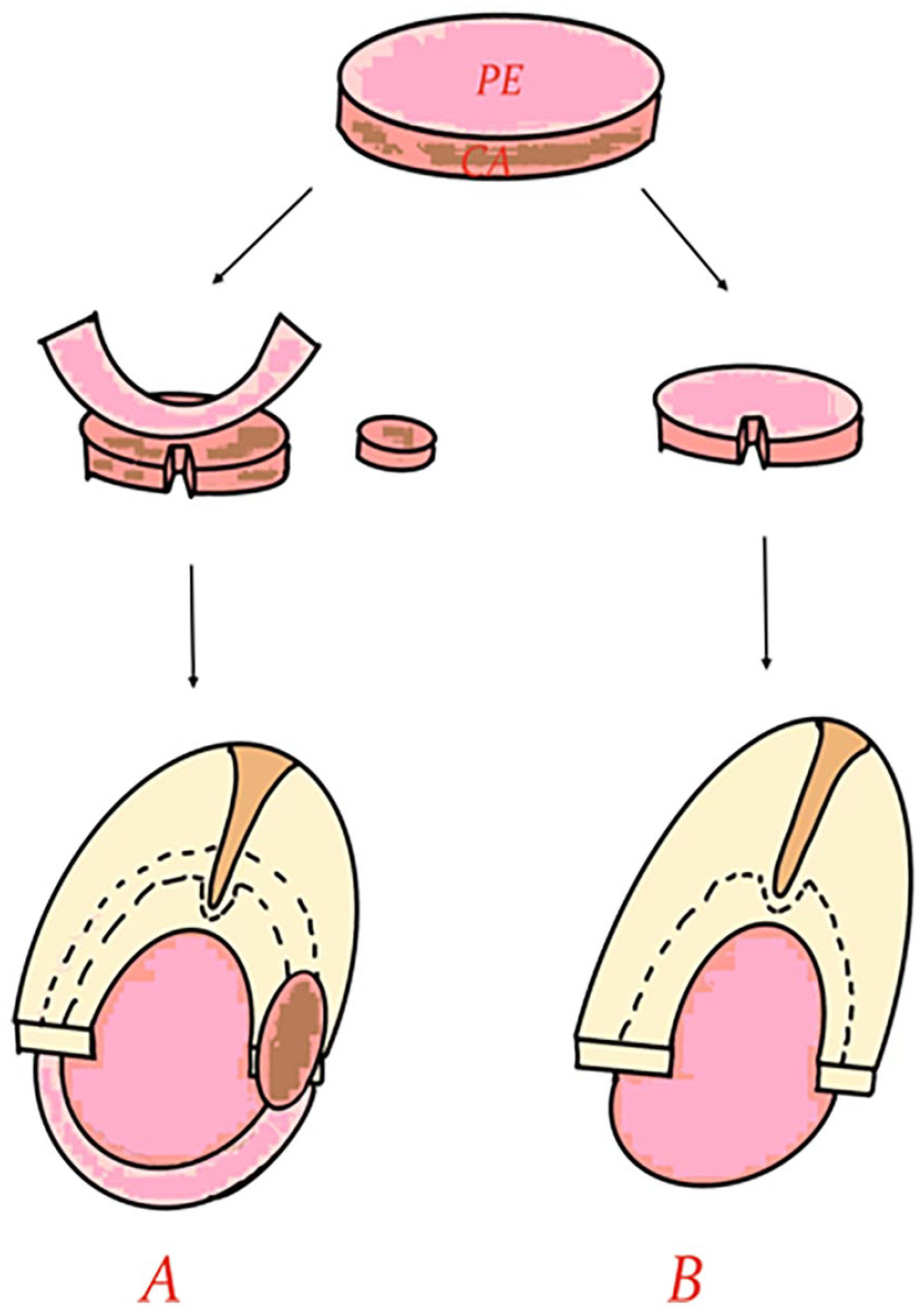
Artist drawing of both techniques. (A) Cartilage reinforcement technique. Harvesting of perichondrium-cartilage composite graft, elevating of lateral perichondrium and a notch of the cartilage graft, and placement of graft and small pieces of cartilage augment. (B) Push-through technique. Harvesting of perichondrium-cartilage composite graft, a notch of the cartilage graft, placement of graft.
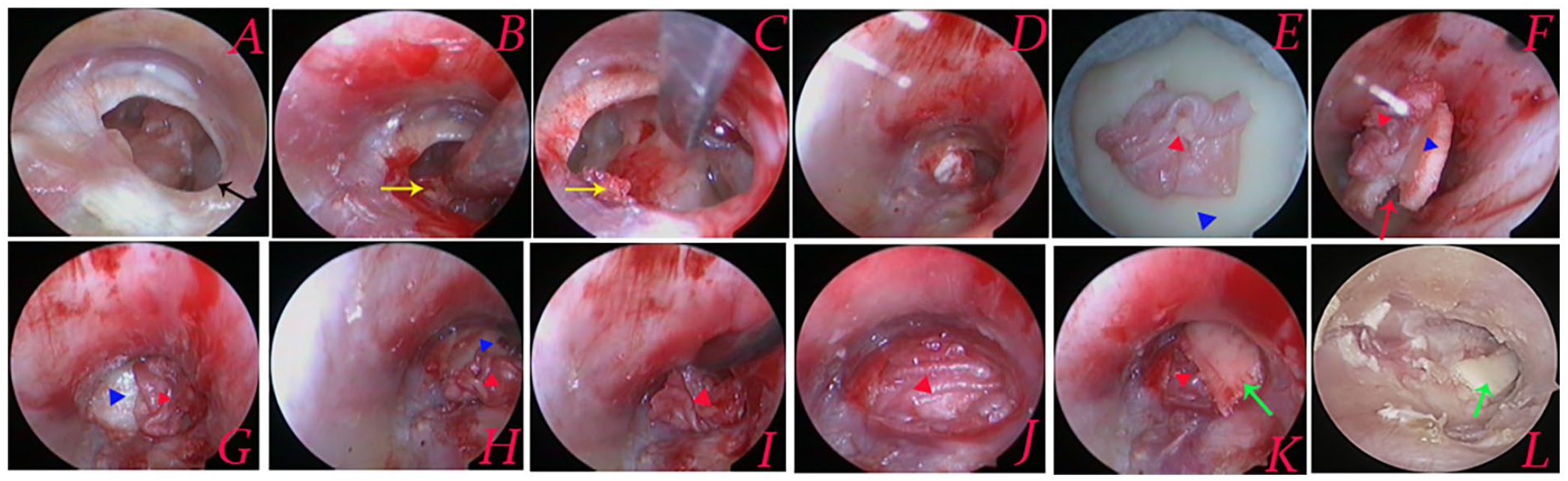
Cartilage reinforcement technique. Preoperative perforation (A), removal of epithelium of the manubrium (B), de-epithelializing of perforation margins (C), middle ear packing (D), graft preparation: elevating lateral perichondrium (E), graft preparation: creating a notch of the malleus handle (F), the cartilage graft medial to the remnant TM and the annulus (G and H), the perichondrium medial to the remnant TM but lateral to the cartilage (I and J), small pieces of cartilage augment the margins (K), postoperative 4 weeks (L). Black arrows indicated the perforation involves the marginal perforation; yellow arrows indicated the manubrium; red arrows indicated a notch of the cartilage graft; green arrows indicated small pieces of cartilage; red triangle indicated the perichondrium graft; blue triangle indicated the cartilage graft.
Cartilage-Perichondrium Push-Through Group
The perichondrium-cartilage composite graft was trimmed to the same size as the perforation but without elevating the lateral perichondrium. The composite graft should be 2 mm larger than the perforation margins. A notch was created in the cartilage graft to accommodate the malleus handle if necessary. The perichondrium-cartilage composite graft was pushed through the perforation and placed medial to the remnant TM and the annulus, with a notch in the cartilage graft accommodating the malleus handle if necessary. 4,6 (Figure 1B)
Postoperative Follow-Up
Postoperative follow-up was scheduled at weeks 2 and 4 and at months 3 and 6. The biodegradable NasoPore fragments were aspirated from the EAC at 2 weeks post-surgery, allowing the graft to be visualized endoscopically.
Outcome Assessment
The postoperative outcome measures included graft success, hearing outcome, and complications. An audiometric evaluation was performed to measure the ABGs at 6 months after surgery. Graft success was defined as the presence of an intact graft with no residual perforation, retraction, lateralization, significant blunting, or medialization, as assessed by otomicroscopy and tympanometry.
Statistical Analyses
Statistical analyses were performed using SPSS (ver. 21.0; IBM Corp., Armonk, NY, USA). Data are expressed as means (with standard deviations) or percentages. The chi-square test was used to compare categorical data. The Wilcoxon and Mann-Whitney U tests were used to compare nonparametric variables, and independent and paired-samples t-tests were used to compare parametric variables. A P-value <.05 was considered to indicate statistical significance.
Results
Demographic Characteristics of the Patients
A total of 57 patients were included in the study (Figure 3). Among the 57 ears (57 patients), there were 29 in the cartilage reinforcement group and 28 in the push-through group. All patients completed 6 months of follow-up. The demographic data for both groups are shown in Table 1. The age, sex, side, duration of perforation, myringosclerosis, smoking status, etc, were matched between the 2 groups (Table 1).
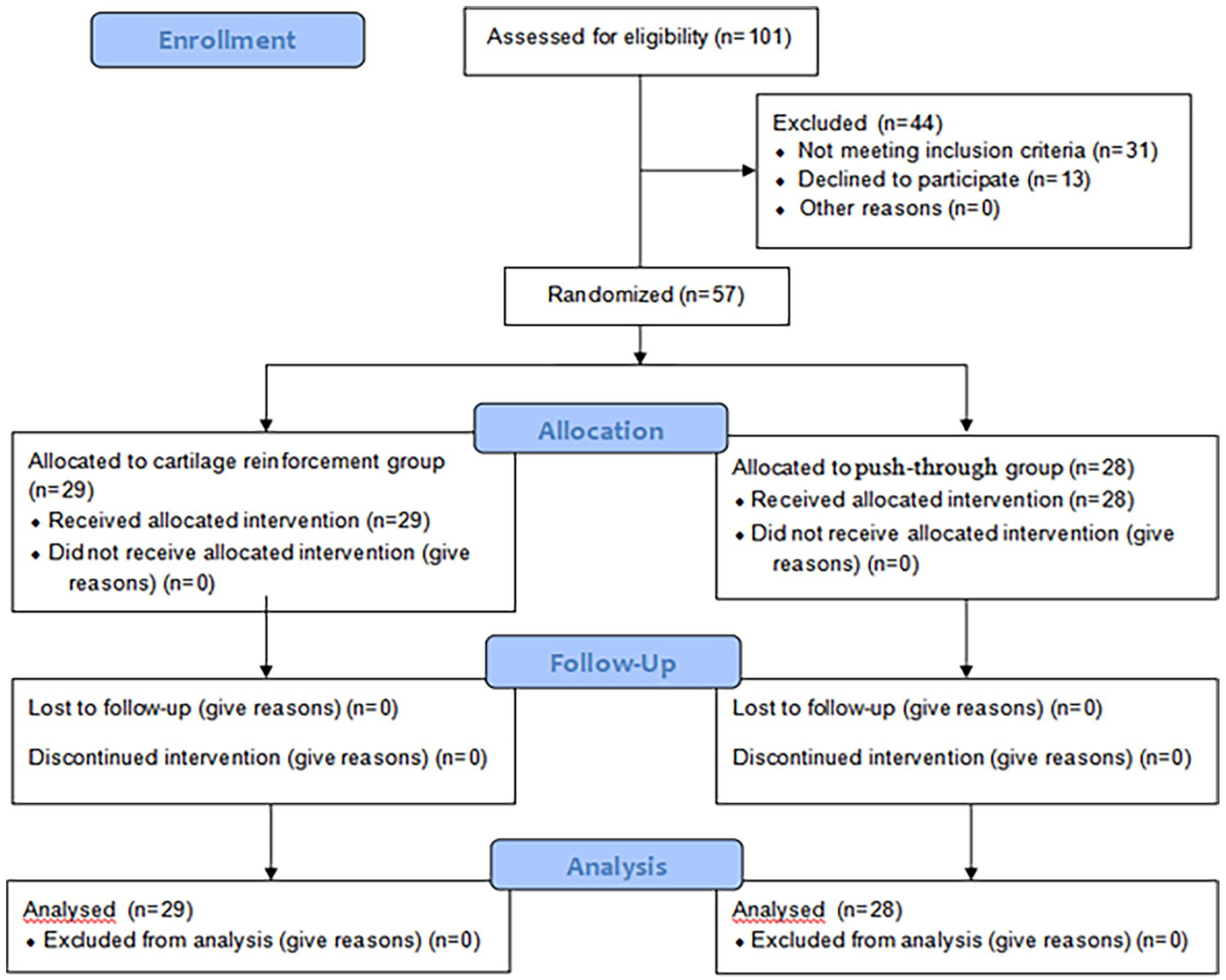
Flow diagram comparing the efficacy of cartilage reinforcement and push-through myringoplasty.
Demographic and Preoperative Data of the Cartilage Reinforcement and Push-Through Groups.
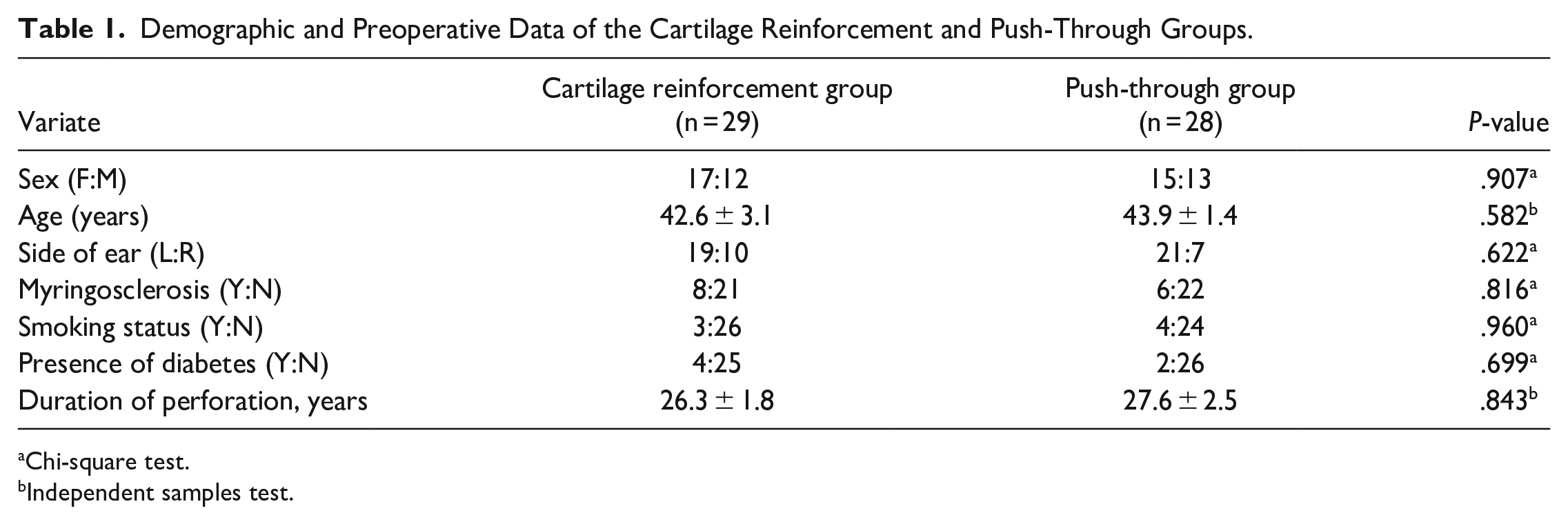
Chi-square test.
Independent samples test.
Graft Success Rates and Postoperative Complications
At 6 months postoperatively, the graft success rate in the cartilage reinforcement group was significantly higher compared to that in the push-through group (100.0% vs 78.6%, P < 0.01) (Table 2). Residual perforation was observed in 5 (17.9%) patients, and re-perforation in 1patient (3.6%), in the push-through group. All residual and re-perforations occurred at the graft margins. No procedure-related complications were found during the follow-up period, including graft medialization, lateralization, significant blunting, sensorineural hearing loss, vertigo, or tinnitus.
Graft Outcomes the Cartilage Reinforcement and Push-Through Groups.
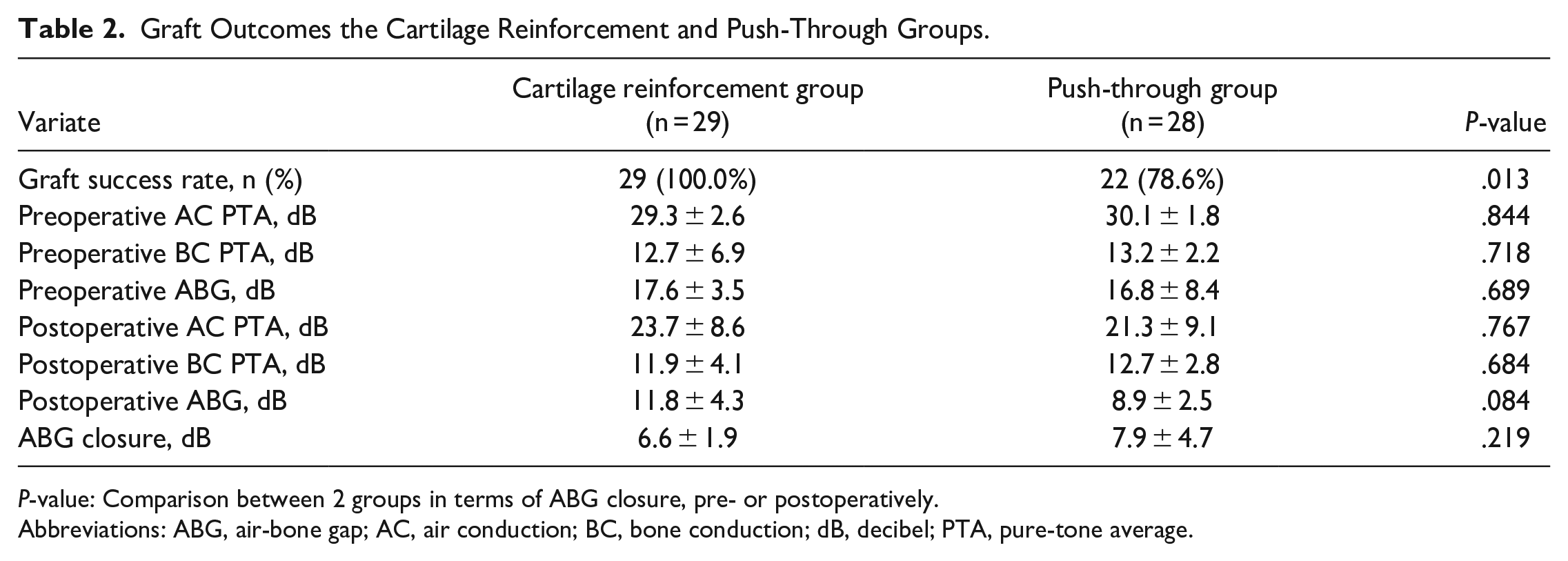
P-value: Comparison between 2 groups in terms of ABG closure, pre- or postoperatively.
Abbreviations: ABG, air-bone gap; AC, air conduction; BC, bone conduction; dB, decibel; PTA, pure-tone average.
Hearing Outcomes
The postoperative ABG showed significant improvement compared to preoperation (Table 2). The preoperative ABG was 17.6 ± 3.5 dB in the cartilage reinforcement group and 16.8 ± 8.4 dB in the push-through group (P > .05). Postoperatively, the ABG significantly improved to 11.8 ± 4.3 dB (P < .01) in the cartilage reinforcement group and 8.9 ± 2.5 dB (P < .01) in the push-through group. No significant difference was found in ABG closure between the 2 groups (6.6 ± 1.9 vs 7.9 ± 4.7 dB, P > .05).
Discussion
Previous studies have shown that the underlay technique had poor surgical outcomes for the treatment of large perforations due to reduced vascular supply, limited margin, and inadequate graft stabilization. 1,7 –10 However, the overlay and underlay-overlay techniques require the removal of the superficial layer and raising of the tympanomeatal flap. Although various techniques have been recommended to repair large perforations, raising the tympanomeatal flap has been a key operation, and its complications have been reported. 2,3 In recent years, the push-through technique has been recommended and serves as a simple and time-saving method. This technique is essentially the cartilage underlay technique; it is mainly used to repair small-medium perforations but rarely also for large perforations. 4 –6 Gu 4 reported that the success rate of the push-through technique was inversely proportional to the perforation size. The key to graft success is adequate support of the remnant TM for the graft; otherwise, the tension of the cartilage is high, which can cause graft extrusion, TM laceration, and cartilage graft slippage, resulting in residual or re-perforation. 5,11
This study applied the cartilage reinforcement technique to repair large perforations, and the graft success rate was significantly higher compared with the push-through technique (100.0% vs 78.6%, P < .01). Other authors reported a success rate of 86.7% to 91.8% using the push-through technique for repairing small-medium perforations and 82.7% for large perforations. 4 –6 The success rate of our cartilage reinforcement technique was comparable to other techniques for repairing large perforations. Choi et al 12 reported a success rate of 95.1% using lateral underlay, compared with 94.1% using butterfly-inlay by Gülşen et al, 5 95.5% using inlay myringoplasty by Eren et al, 13 and 93.8% using the transmeatal technique by de Savornin Lohman. 14 Kawano 15 applied the anterior subannular grafting technique for the treatment of subtotal perforations and achieved a success rate of 98.3%. Nevertheless, these techniques required the raising of a tympanomeatal flap.
Although our cartilage reinforcement technique is similar to the underlay and push-through techniques, it differs in that the size of the perichondrium is significantly larger than the size of the cartilage in our reinforcement technique. In this respect, it is more similar to the double underlay technique, where the wide perichondrium may offset the insufficient cartilage size and misfitting perforation margins. However, the size of the perichondrium and cartilage is the same in the push-through technique. In addition, some scholars believe that excess free perichondrial grafts can be used to fill the gap between the graft and perforation edge to improve the success rate. 16,17 Our cartilage reinforcement technique was also similar to butterfly cartilage myringoplasty. Alain et al 18 applied the butterfly technique to repair large perforations and achieved an 88% success rate.
More importantly, cartilage reinforcement of the margins ensures intimate contact of the graft and remnant TM in this technique. In the push-through technique, our findings and those of previous scholars have shown that residual or re-perforation mainly occurs at the graft margins. 5,11 This issue is addressed by our reinforcement technology. Other scholars have reported using cartilage-reinforced temporalis fascia or perichondrium to repair anterior or marginal perforations and achieved success rates of 94.7% to 100%. 1,7,8 Tek et al 8 found that the cartilage reinforcement technique had a significantly higher success rate compared with temporalis fascia (100% vs 66%). However, our reinforcement technique differs from those reported by these scholars. In their techniques, all the cartilage reinforcement and temporalis fascia or perichondrium were placed medial to the remnant TM, while in our technique, the cartilage reinforcement is placed lateral to the remnant TM to ensure intimate contact of the graft and remnant TM without leaving a gap. Thus, in this study, the use of perichondrial flaps and meticulous placement of the graft and closure of any gaps with cartilage or perichondrium accounted for the improvement of graft success achieved with the cartilage reinforcement technique.
This study showed that there was no statistical difference in hearing outcomes between the 2 techniques. Our technique is similar to the cartilage butterfly technique, in which one “wing” of the cartilage is placed at least 1–2 mm lateral to the surface of the TM. 5,18,19 However, previous studies showed no significant difference in hearing improvement between the butterfly technique and other methods. 5,19 Alain et al 18 reported that the ABG improved from 29.7 to 11.3 dB for large marginal perforations following butterfly cartilage myringoplasty, and the hearing improvement remained stable over the long term. Additionally, we believe that the concern about iatrogenic cholesteatoma is unfounded when placing cartilage on the remnant TM, as no iatrogenic cholesteatoma was found after butterfly cartilage myringoplasty. 5,18,19 We also did not find any iatrogenic cholesteatoma in the perichondrium overlaying the squamous epithelium when using our technique in recent studies. 9,10 Regarding ventilation tube insertion for the treatment of chronic otitis media with effusion, few studies have reported middle ear cholesteatoma (1.1% of operated ears). 20,21 In contrast, Olarieta Soto et al 22 reported a rate of 4% of epithelial pearls when using double fascia graft after excision of the epithelial layer. The surgical indications for endoscopic cartilage reinforcement include anterior perforation, marginal perforation, total perforation, and inadequate graft size in the underlay technique. The limitations of this study were the small sample size and short follow-up, which rendered the re-perforation rate and long-term complications unclear. Future studies should include larger sample sizes and longer follow-ups.
Conclusion
Cartilage reinforcement myringoplasty is a simpler and useful technique for achieving graft success compared with cartilage-perichondrium push-through in the treatment of large marginal perforations and does not affect hearing levels.
Footnotes
Authors’ Note
Author Contributions
Z.L.: Interpretation of data for the work, design of the work, analysis of data for the work, drafting the work, agreement to be accountable for all aspects of the work; final approval of the version to be published. Z.L., J.W., B.Z., and Y.H.: Interpretation of data for the work, analysis of data for the work, drafting the work and technical the diagram, agreement to be accountable for all aspects of the work; final approval of the version to be published. Z.C.: Interpretation of data for the work, design of the work; final approval of the version to be published.
Data Availability Statement
All data generated or analyzed during this study are included in the published article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Health Commission of Zhejiang Province, China (Grant#2021KY1186), Shanghai Medical Innovation Project, China (Grant#22Y11902100), and Technology Agency of Jinhua City, China (Grant#2022-3-042).
Ethical/Consent Statement
The study protocol was reviewed and approved by the Institutional Ethical Review Board of Shanghai Sixth People’s Hospital Affiliated to Shanghai Jiao Tong University School of Medicine. All participants provided written informed consent.