
Abstract
Objective
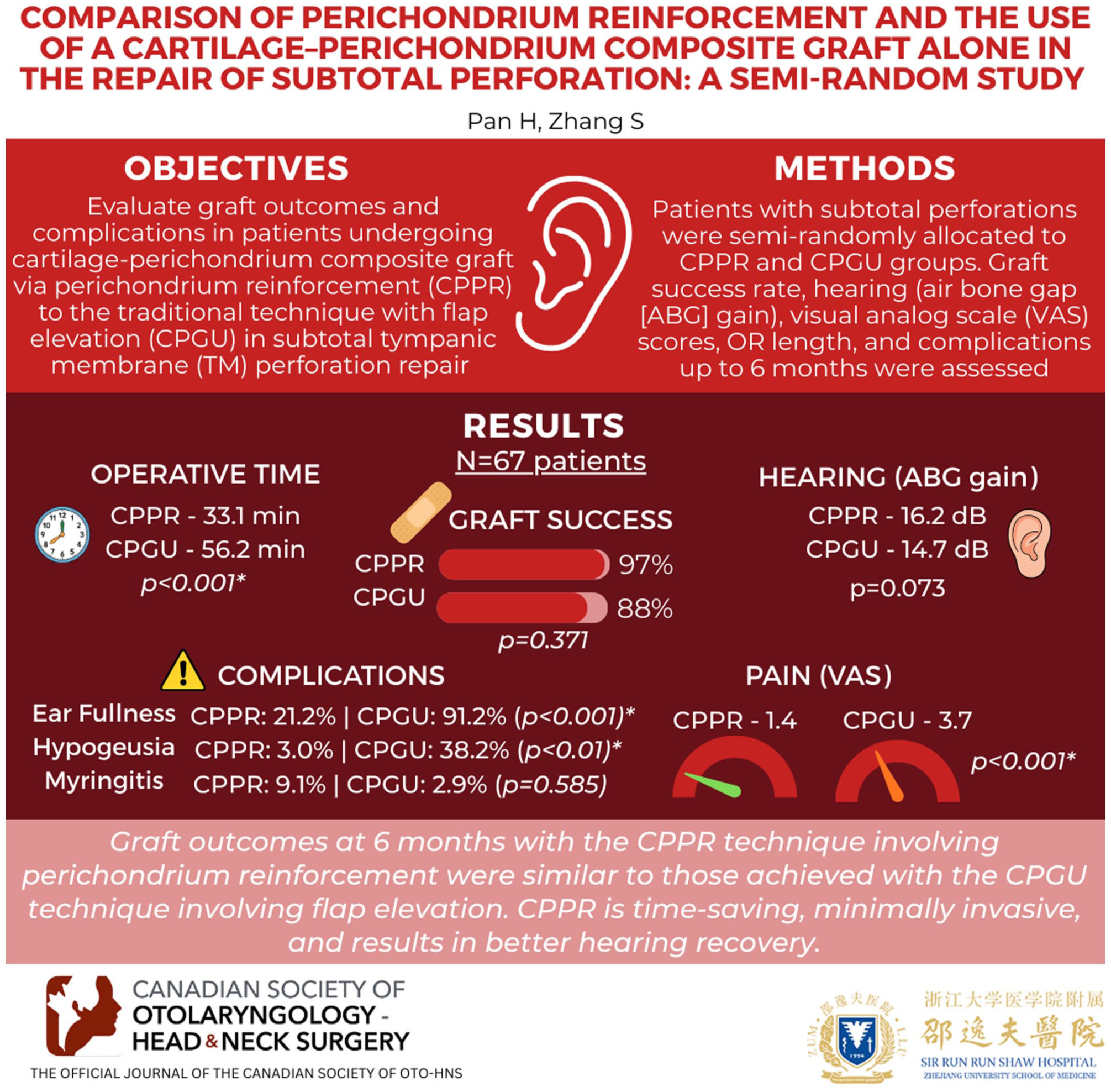
Graft outcomes and complications were compared in patients who received a cartilage–perichondrium composite graft via perichondrium reinforcement (CPPR) and those treated using only a cartilage–perichondrium composite graft underlay (CPGU) technique, including raising a tympanomeatal flap, in the repair of a subtotal perforation.
Materials and Methods
Patients with subtotal perforations were semi-randomly allocated to the CPPR and CPGU groups. The graft success rate, hearing outcomes, operation times, postoperative visual analog scale (VAS) values, and complications were compared for up to 6 months postoperatively.
Results
The sample consisted of 67 ears from 67 patients. The mean operation time was 33.1 ± 2.8 min in the CPPR group and 56.2 ± 1.8 min in the CPGU group. At 6 months postoperatively, the VAS scores were 1.4 ± 0.9 and 3.7 ± 1.2, and the graft success rates were 97.0% and 88.2% (P = .371), respectively. There were no significant differences in the mean gain in the air–bone gap (16.2 ± 5.3 vs. 14.7 ± 6.2) between the two groups, but hearing improvement was greater in the CPPR group. Ear fullness was reported by 21.2% patients in the CPPR group and 91.2% of patients in the CPGU group. Temporary hypogeusia developed in 3.0% of patients in the CPPR group and 38.2% of those in the CPGU group. Myringitis was seen in 9.1% patients in the CPPR group and 2.9% in the CPGU group.
Conclusion
In patients undergoing subtotal perforation repair, the 6-month graft outcome in patients treated with the perichondrium reinforcement technique without raising a tympanomeatal flap and external ear canal packing was similar to that of patients who underwent a flap-raising technique. The advantages of the perichondrium reinforcement technique are that it is simple, time-saving, and minimally invasive, with less ear fullness and better hearing recovery.
Keywords
Introduction
Tympanic membrane (TM) reconstruction is mainly performed to fill a defect in the TM using graft material. Perforation closure is achieved by inosculation of the graft and remnant TM, graft neovascularization, and epithelization.1,2 Although cartilage myringoplasty is a well-established procedure, facilitated by the development of endoscopic techniques,1,3 –5 the repair of subtotal perforations remains a challenge. Factors related to closure failure and thus residual perforation include insufficient graft size, graft movement, infection, and unrecognized middle ear mucosal disease.3 –5 Close contact between a graft of sufficient size and the remnant TM is essential to avoid failed graft inosculation. Different techniques have been used in the repair of subtotal perforations, but all of them require raising a tympanomeatal flap via an incision in the external ear canal (EAC).6 –10 If the procedure is not performed by a skilled surgeon, there is a high risk of a torn or misplaced flap, which will not only fail to reinforce the graft but may also result in damage to the chorda tympani, graft lateralization, inclusion cholesteatoma in the EAC, slow healing, pain, and longer operation times.1,3,6,7
In recent years, graft reinforcement has been proposed in cases in which the graft size cannot meet the needs of perforation repair, including through the use of perichondrium cartilage,11,12 temporalis fascia cartilage,13,14 and other cartilage sources.15,16 Studies have reported variable or no effects of the double cartilage graft on the vibration of the repaired TM and thus on hearing improvement.15,16 The acoustic properties of the perichondrium are similar to those of the TM, and any cartilage-related acoustic transfer loss can be reduced by decreasing the thickness of the cartilage.17,18 Moreover, clinical studies have reported greater hearing improvement with a perichondrium graft than with a cartilage graft, particularly in the high-frequency range.19,20 Tragus cartilage is composed of bilateral perichondrium and intermediate cartilage, whereas in the endoscopic cartilage technique, only a composite graft of cartilage and perichondrium on one side is used.1,3 –5,12 To date, the efficacy of perichondrium reinforcement, consisting of a perichondrium–cartilage composite graft, without raising a tympanomeatal flap, has not been investigated. Thus, in this study, we compared the operation times, graft outcomes, and complications following subtotal perforation repair performed using a cartilage–perichondrium composite graft via perichondrium reinforcement (CPPR) versus cartilage–perichondrium composite graft underlay (CPGU) technique alone, with the latter including the raising of a tympanomeatal flap.
Materials and Methods
Ethical Considerations
The study was conducted in accordance with the ethical standards of the Declaration of Helsinki. It was approved by the Medical Ethics Committee of Sir Run Run Shaw Hospital, Zhejiang University School of Medicine. Informed consent was obtained from all participants.
Patient Selection
Study subjects were recruited from consecutive patients diagnosed with chronic subtotal perforation with only a remnant annular edge on at least one side who visited the Department of Otorhinolaryngology, Head and Neck Surgery between January 2020 and October 2023. The inclusion criteria were perforation size 1/2–3/4 of the TM, dry ear for at least 3 months prior to enrollment, air–bone gap (ABG) < 35 dB, and a well-pneumatized mastoid. The exclusion criteria were previous ear surgery, fungal otitis externa, and suspicious ossicular chain abnormalities as seen in high-resolution computed tomography (HRCT) audiograms, or intraoperative findings. HRCT and audiograms were performed in all patients prior to enrollment. The causes of perforation included chronic mucosal otitis media and failed healing of a traumatic perforation for at least 12 months.
Age, sex, ear side, contralateral ear status, perforation duration and cause, smoking status, diabetes, myringosclerosis, Valsalva maneuver, operation time, and pre- and postoperative hearing levels were recorded. A Valsalva maneuver was performed the day before surgery to preliminarily evaluate Eustachian tube function. Operation time was defined as the time from completing anesthesia induction to tragus incision compression. Pain intensity was measured postoperatively on the day of surgery, when the patient was wide awake. All patients were asked to score their pain on a visual analog scale (VAS) with scores ranging from 1 (no pain) to 10 (severe pain). 1 Only deep ear pain as reported by the patient was scored; pain in the tragus area was not. 1 Audiometric data were assessed preoperatively and at 6 months postoperatively based on the standards of the Hearing Committee of the American Academy of Otolaryngology–Head and Neck Surgery.1,2
Patient Treatment Allocation and Masking
Consecutive patients who met the inclusion criteria were allocated to either the CPGU group or the CPPR group according to the order of submission of written informed consent (thus semi-randomly). The informed consent form was labeled using consecutive natural numbers starting from 1 (1,2,3. . ..). An office nurse uninvolved in surgical procedures performed the allocation. If the terminal digit of the natural number was an uneven number (1,3,5,7,9), the participant was allocated to the CPGU group; if the terminal digit of the natural number was an even number (2,4,6,8,10), the participant was allocated to the CPPR group.
The CPPR technique differs from the CPGU technique in that it does not involve raising a tympanomeatal flap, trimming the perforation margins, or EAC packing; instead, pieces of perichondrium are placed lateral to the cartilage–perichondrium composite graft. The patients and the individual performing the assessment were blinded to treatment allocation.
Surgical Approach
All myringoplasties were performed endoscopically by the same surgeon with the patient under general anesthesia. The middle ear was inspected using 0° and 30° endoscopes.
CPPR Technique
As noted above, this technique does not involve raising a tympanomeatal flap and trimming the perforation margins. The epithelium was removed from the distal malleus handle, but the TM was not elevated off the malleus manubrium.
A cartilage-one-sided perichondrium composite graft was harvested. Simultaneously, the other side of the perichondrium was also obtained to serve as a free perichondrium graft.
The lateral perichondrium was raised circumferentially from the composite graft, with attachment at the center of the cartilage. The cartilage graft was shaped peripherally so that it was slightly larger than the perforation margins, and a notch was created to accommodate the malleus handle in the cartilage graft. The perichondral flap of the composite graft was shaped peripherally to be 1 to 2 mm larger than the cartilage graft.
The tympanic cavity was packed with biodegradable NasoPore (Stryker Canada, Hamilton, ON, Canada). The composite graft was placed transperforationally, medial to the remnant TM and the annulus, with the notch in the cartilage accommodating the malleus handle. The perichondral flap of the composite graft was also placed medial to the remnant TM and the annulus, but lateral to the malleus handle.
This free perichondrium graft was placed lateral to the composite graft and the annulus to reinforce the composite graft (Figure 1 and Video 1). EAC packing was not applied.

CPPR. (A) preoperative perforation. (B) middle ear packing. (C) preparation of the perichondrium–cartilage composite graft. (D) composite graft placement. (E) preparation of the perichondrium. (F) perichondrium placement. The blue triangle indicates the composite graft, and the green triangle is the perichondrium graft.
CPGU Technique
In this group, a raised tympanomeatal flap, trimming of the perforation margins, and removal of the epithelium from the malleus handle were performed. The perforation margins were trimmed, and the epithelium was removed from the malleus handle. The technique was used in previous studies.4,17
A tympanomeatal flap made via EAC incision was elevated, the annulus was identified, and the middle ear was entered. The tympanic cavity was packed with biodegradable NasoPore. Cartilage, together with perichondrium on the parotid side, was harvested as a composite graft. Then the lateral perichondrium was elevated circumferentially around the graft, with the pedicle remaining attached to it. The composite graft was entered into the middle ear via the trans-tympanomeatal flap, with the cartilage placed medial to the TM remnant and annulus, and the notch in the cartilage graft accommodating the malleus handle. The raised perichondral graft was placed lateral to the long process of the malleus and medial to the TM remnant and tympanomeatal flap. The EAC was packed with biodegradable NasoPore.
Postoperative Follow-Up and Outcome Assessment
Patients were discharged the day after surgery. Pain intensity was measured and recorded. Postoperative follow-up was scheduled at 2 and 4 weeks and at 3 and 6 months. In the CPGU group, the biodegradable NasoPore fragments were aspirated from the EAC 2 weeks after surgery. The graft was visualized endoscopically and patients were asked about altered taste, vertigo, and tinnitus at each follow-up visit. An audiometric evaluation was performed to measure ABG at 6 months postoperatively. Graft success was defined as the presence of an intact graft with no residual perforation or reperforation, as assessed by endoscopy. Follow-up exams were performed by a surgeon not involved in the initial operation.
Statistical Analyses
The data are presented as the mean ± standard deviation for quantitative variables and as the frequency (percentage) for qualitative variables. Group comparisons were performed using an independent-samples t-test for quantitative variables and a chi-square test for qualitative variables. A paired t-test was used to evaluate differences in ABG thresholds between groups. All statistical analyses were performed using SPSS (version 20; IBM Corp., Armonk, NY, USA). A P-value < .05 was considered to indicate statistical significance.
Results
Demographic Characteristics
The study population consisted of 67 patients, with a total of 67 treated ears, 33 treated with the CPPR technique and 34 with the CPGU technique. The demographic, baseline, and surgical characteristics of the patients are shown in Table 1. Demographic data were matched between the two groups. All patients completed 6 months of follow-up.
Demographic Characteristics of Patients.

Chi-square test.
Independent Samples t-test.
Abnormity: the presence of perforation/or otitis media.
Operation Time and Postoperative Pain Scale
The mean operation time was 33.1 ± 2.8 (range: 29–42) min in the CPPR group and 56.2 ± 1.8 (43–61) min in the CPGU group (P < .001). The postoperative VAS score on the day of surgery was 1.4 ± 0.9 in the CPPR group and 3.7 ± 1.2 in the CPGU group (P < .001) (Table 2).
The Graft Success Rate, Operation Time, VAS Score, and Complications.

Chi-square test.
Independent Samples t-test.
Postoperative Endoscopic Views and Graft Success Rate
Endoscopic inspection showed a graft bulge and the clinical inosculation of all grafts and remnant TM at 1 week postoperatively, the initiation of neovascularization of the perichondral graft surface and graft flattening at 2 weeks, complete graft neovascularization at 3 weeks, complete neovascularization of the cartilage graft at 4 to 5 weeks, and graft epithelization in the CPPR group at the final follow-up exam (Figure 2). The reinforcement second perichondrium was incorporated into the composite graft, with the formation of a vascular covering and without a significant boundary. However, clinical inosculation of the graft and remnant TM and graft neovascularization were also observed in the CPGU group after EAC packing removal at 2 weeks postoperatively.

Same Patient as in Figure 1. (A) preoperative perforation. (B) 1 week postoperatively. (C) 2 weeks. (D) 3 weeks. (E) 5 weeks. (F) 3 months.
An infection occurred postoperatively in one (3.0%) patient in the CPPR group and in three (8.8%) patients in the CPGU group (P = .628). All of the infections were controlled but only one patient in the CPGU group had no residual perforation; the remaining three patients (one patient in the CPPR group and two patients in the CPGU group) had residual perforation. In the patients without infection in both groups, no residual perforation was seen in the 32 patients in the CPPR group, whereas anteroinferior residual perforation occurred in 2 patients in the CPGU group. Overall, one (3.0%) patient in the CPPR group and four (11.8%) in the CPGU group had residual perforation (P = .371). No reperfusion occurred in either group. The graft success rate, as determined 6 months postoperatively, was 97.0% (n = 32) in the CPPR group and 88.2% (n = 30) in the CPGU group (P = .371) (Table 2).
Hearing Outcomes and Complications
The postoperative ABG was significantly better than the preoperative value in both groups. There were no significant differences between the preoperative and postoperative average bone conduction pure-tone average (BC-PTA) in either group (Table 3). The between-group differences in the pre- (P = .741) and postoperative (P = .275) ABG values were also not significant, nor were the pre- (P = .671) and postoperative (P = .710) mean BC-PTA. Although the difference in ABG gain (P = .073) between the two groups was not significant, hearing improvement was better in the CPPR group than in the CPGU group (Table 3).
Comparison of Hearing Gains, the Air–Bone Gap, and Bone Conduction.

dB, decibel; S.D., Standard deviation; BC, bone conduction; PTA, pure-tone average.
Paired Samples test, Comparison between the same groups in regard to ABG or bone conduction, pre- and postoperatively.
Mann Whitney U test, Comparison between two groups in terms of gain, pre- or postoperatively.
P < .01.
Complications
There were no cases of graft medialization, graft lateralization, or significant blunting. None of the patients reported sensorineural hearing loss, vertigo, or intractable tinnitus. However, 21.2% of the patients in the CPPR group and 91.2% of those in the CPGU group reported ear fullness (P < .001). Temporary hypogeusia was reported by 3.0% patients in the CPPR group and 38.2% of those in the CPGU group (P < .01). Myringitis was seen in 9.1% of patients in the CPPR group and 2.9% of those in the CPGU group (P = .585). EAC scarring/stenosis developed in 5.9% of the patients in the CPGU group.
Discussion
Myringoplasty for the treatment of subtotal perforation has a high graft failure rate due to the lack of residual TM.6 –10,17 Several techniques have been developed to ensure adequate graft contact.6 –10,17 Kawano 6 achieved a graft success rate of 93.6% using an anterior subannular technique. In other studies, the success rate was 95.1% using a circumferential subannular technique, 7 90.3% using a “U” flap technique, 8 89.8% using an anterior tab flap, 9 and 98.0% using an interlay technique. 10 A key to graft success is raising a tympanomeatal flap of adequate size,6 –10 but the drawbacks of these flap-dependent procedures include a prolonged procedure time and EAC complications, such as injury of the chorda tympani, graft lateralization, and inclusion cholesteatoma.1,3,6,7
Graft reinforcement has been recommended to ensure that there are no gaps between the graft and the perforation margin.13 –18 However, most reinforcement techniques rely on cartilage reinforcement using the temporalis fascia,15,16,21,22 which requires two incisions and the raising of a tympanomeatal flap. By contrast, the CPPR technique does not involve raising a tympanomeatal flap, which requires an additional incision or margin trimming and EAC packing. The mean operation time was significantly shorter, and the postoperative VAS score was lower in the CPPR group than in the CPGU group. Previous studies have demonstrated that not trimming the margins does not compromise graft success. 1 Other studies have reported that EAC packing is not necessary for the myringoplasty performed without the raising of a tympanomeatal flap.1,5 However, EAC packing may be necessary for patients treated with a raised tympanomeatal flap, as it supports flap recovery and prevents EAC stenosis.
In our study, there were no significant differences in the graft success rate between the two groups. A high success rate using a cartilage reinforcement fascia technique and tympanomeatal flap raising was reported in 93.4% of patients in Kouhi et al., 15 86.5% in Tek et al., 21 and 98.9% in Mundra et al. 22 The graft success rate in our CPPR group was comparable. Good results have also been obtained using a perichondrium reinforcement cartilage technique. The graft success rates in Shakya et al., 13 Wang et al., 14 and Shakya et al. 23 were 95%, 97.5%, and 87.2%, respectively. Although our rates are similar, the advantage of CPPR is that a flap is not raised, whereas in the cited studies, the perichondrium was used to reinforce the barred cartilage or cartilage palisades. The CPPR technique is similar to the “cartilage reinforcement cartilage graft technique” recently reported in two studies.17,18 That approach also does not include raising a tympanomeatal flap, but the perforation margins are trimmed, and a small piece of cartilage ring is used to reinforce the annulus.17,18 These procedures not only increase the technical difficulty of shaping the ring cartilage, but they may also lead to displacement of the ring cartilage following EAC packing.
The graft success rate was not significantly different between the CPPR and CPGU groups. The total residual perforation rate was 3.0% in the CPPR group and 11.8% in the CPGU group, without a significant difference. There was no residual perforation in the CPPR group except in the one patient with infection, whereas residual perforation occurred in two patients without infection and three with infection in the CPGU group. Postoperative infection is a strong risk factor for graft failure. 1 These results suggest a lower risk of residual perforation in the CPPR group.
In this study, a large free perichondrium graft was placed lateral to the perichondral flap and the annulus to reinforce the composite graft and prevent gaps between the graft and the perforation margins. In addition, in the CPPR group, there was no trimming of the perforation margins, which ensured their sufficiency, or EAC packing, which avoided displacement due to external pressure. Postoperative endoscopy confirmed clinical inosculation of the grafts and remnant TM, followed by graft neovascularization, in all patients. These observations support the conclusion that not trimming the perforation margins and the absence of EAC packing do not affect either the graft success rate or graft neovascularization following myringoplasty.1,5
Although there were no significant differences in hearing improvement between the two groups, the CPPR group had better hearing recovery, perhaps because, in the CPGU group, raising a tympanomeatal flap and trimming the margins may cause slight mechanical damage to the ossicular chain. 24 This result contrasts with other studies of the cartilage ring reinforcement technique. In two studies, the group without cartilage ring reinforcement had better hearing recovery.18,25 This suggests that the cartilage rings covering the residual TM increase the weight and pressure on the new TM and ossicular chain, thereby affecting the vibration and conduction of the TM. Another advantage of the absence of flap raising and EAC packing was the lower rates of ear fullness and temporary hypogeusia, as demonstrated in the CPPR group. However, myringitis developed in 9.1% patients of the CPPR group but only 2.9% of those in the CPGU group.
Inclusion cholesteatoma is among the possible complications of CPPR. In clinical studies, there were no cases of inclusion cholesteatoma involving the epithelium of the remnant TM and the graft.26,27 However, a similar study reported an incidence rate for inclusion cholesteatoma of 4.8% during 3 to 5 years of follow-up. 28 In our study, 5.9% patients in the CPGU group developed EAC scarring/stenosis. Although the TM was not elevated off the malleus manubrium and the perichondral flap of the composite graft was placed lateral to the malleus handle in this study, previous authors reported that perichondrium graft covering the epithelium of the TM had a minimum incidence rate of inclusion cholesteatoma. 28 The failure to detect inclusion cholesteatoma in our patients may have been due to the relatively short follow-up time in either group. However, the possibility of iatrogenic cholesteatoma cannot be completely ruled out in the future. Given the use of cartilage-based grafts, it would be important to confirm the absence (or presence) of epithelial entrapment or retraction pockets that may predispose to cholesteatoma formation over time. Nevertheless, inclusion cholesteatoma appears to be independent of graft placement. In the series of Nejadkazem et al., 29 0.8% of 1,121 ears developed inclusion cholesteatoma after treatment with the underlay technique. In other studies, the cholesteatoma incidence rate following cartilaginous underlay myringoplasty was 6 to 6.7%.30,31 Fortunately, inclusion cholesteatoma may be successfully removed in the clinician’s office using an endoscope.29 –31
The strength of this study is that no patient was lost to follow-up, such that our results are strongly supported. In addition, the absence of EAC packing in the CPPR group facilitated endoscopic observation of the changes in the graft. The primary weaknesses of our study were the small sample size, short follow-up time, and its non-randomized, single-center design. Short-term follow-up is problematic, CPPR group may cause the risks of delayed complications such as late graft failures, reperforation, and inclusion cholesteatoma. Thus, long-term follow-up should be performed in the future. Another limitation is that the surgeries were completed by a single experienced surgeon in this study; the outcomes may differ when performed by less-experienced surgeons.
Conclusion
Although the perichondrium reinforcement technique does not require the raising of a tympanomeatal flap or EAC packing, graft outcomes at 6 months in patients undergoing the repair of a subtotal perforation were similar to those achieved with the flap-raising technique. However, the perichondrium reinforcement technique is simpler, time-saving, and minimally invasive, resulting in less ear fullness and better hearing recovery.
Footnotes
Acknowledgements
None.
Abbreviations
Tympanic membrane: TM
External auditory canal: EAC
High-resolution computed tomography: HRCT
Cartilage–perichondrium composite graft by perichondrium reinforcement: CPPR
Cartilage–perichondrium composite graft: CPGU
Visual analog scale: VAS
Air–bone gap: ABG
Bone conduction: BC
Authors’ Contributions
Hong Pan: data interpretation, study design, data analysis, drafting the manuscript. Shoude Zhang: data interpretation, data analysis. Both agree to be accountable for all aspects of the work and give final approval of the version to be published.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
The study was conducted in accordance with the ethical standards of the Declaration of Helsinki. The study was approved by the Medical Ethics Committee of Sir Run Run Shaw Hospital, Zhejiang University School of Medicine.
Consent to Participate
Informed consent was obtained from all participants.
Consent for Publication
Informed patient consent was obtained in writing.
Data Availability Statement
The datasets supporting the conclusions of this article are included within the article.
Supplemental Material
Additional supporting information is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.