
Abstract
Objective:
We evaluated the graft success rate and hearing outcomes of endoscopic cartilage graft myringoplasty without tympanomeatal flap elevation used to repair posterior marginal perforations.
Study Design:
A prospective case series.
Materials and Methods:
A total of 31 patients with posterior marginal perforations who underwent endoscopic cartilage graft myringoplasty were included. The outcomes were the hearing gain and graft success rate at 6 and 24 months.
Results:
The graft success rate was 96.7% (30/31) at 6 months and 90.3% (28/31) at 24 months; 1 patient exhibited composite graft extrusion and lateralization in the region of the anterior annulus; a residual perforation was apparent. Reperforation occurred in 2 patients. The mean preoperative air-bone gap (ABG; 28.61 ± 3.14 dB) was significantly greater than the mean postoperative ABG (12.15 ± 3.98 dB; P < .05) at 6 months; however, there was no statistically significant difference between the post-6 months and post-24 months with regard to ABG values (P = .871), ABG gain (P = 0.648), or functional success rate (P = .472). No significant graft blunting or atelectasis was noted during follow-up. The free perichondrium became fully integrated with the skin of the external auditory canal; the perichondrium could not be clearly distinguished endoscopically 4 to 8 weeks postoperatively. Computed tomography revealed well-pneumatized middle ear and mastoid cavity at postoperative 24 months.
Conclusion:
Endoscopic cartilage graft myringoplasty without tympanomeatal flap elevation reliably repairs posterior marginal perforations. The short- and long-term graft success rate is high, and the hearing results are satisfactory; the technique is minimally invasive.
Introduction
Underlay or overlay myringoplasty is used to repair perforations associated with mucosal chronic otitis media (COM) and an intact ossicular chain. Generally, the underlay technique is associated with a higher risk of graft failure because the residual native tympanic membrane (TM) does not support marginal perforations.1,2 The overlay technique is technically more difficult and occasionally complicated by graft lateralization, anterior blunting, and epithelial pearl production.1,2 Several surgical techniques have been developed to improve the graft success rate; these include sandwich graft tympanoplasty, 3 over-under tympanoplasty, 4 mediolateral graft tympanoplasty, 5 the “window shade” technique, 6 “hammock” tympanoplasty, 7 and loop underlay tympanoplasty. 1 However, all require the elevation and restoration of differently sized tympanomeatal flaps to strengthen the grafting of marginal perforations. Such flap manipulations prolong the operation time. Although butterfly cartilage myringoplasty does not require tympanomeatal flap elevation, it is not easy to ensure that the cartilage graft groove accurately follows the perforation margins.8-10 Here, we use cartilage–perichondrium composite graft myringoplasty to repair posterior marginal perforations; tympanomeatal flap elevation is unnecessary because the perichondrium graft is placed lateral to the posterior bony annulus and the posterior external auditory canal (EAC). We present our preliminary data on the graft success rate and hearing gain.
Materials and Methods
Ethical Considerations
The study protocol was approved by the institutional ethical review board of Yiwu Central Hospital. Informed consent was obtained from all participants.
Patients and Methods
This prospective case series ran from January 1, 2016, to December 31, 2017. The inclusion criteria included a posterior marginal perforation, COM, an intact ossicular chain without a cholesteatoma, and a need for TM repair. Patients exhibiting ossicular chain disruption and revision cases were excluded. Temporal bone computed tomography/magnetic resonance imaging was performed to exclude a middle ear cholesteatoma. Pure-tone audiometry was performed preoperatively and 6 and 24 months postoperatively at the standard frequencies of 0.5, 1, 2, and 3 kHz. The air-bone gap (ABG) was the average difference between air and bone conduction at 0.5, 1, 2, and 3 kHz. Each TM perforation was classified as small (<50% of the eardrum) or large (≥50%).
Surgical Procedure
A 0°, 4 mm × 18 cm rigid endoscope and a high-definition monitor were used. The left hand was used to hold the endoscope and the right to perform surgery. The monitor was placed on the side of the patient where the surgeon did not stand. All patients were under general anesthesia. A composite tragal cartilage–perichondrium graft (with the perichondrium stripped from one side) was harvested and a 1 to 1.5 mm skin incision created on the medial side of the ipsilateral tragus. The composite graft was at least 2 mm wider than the diameter of the annulus but was not thinned. The perichondrium on one side of the composite graft was peeled over at least 2 mm to form free perichondrium and uncover cartilage; the perichondrium on the other side remained attached to cartilage. The cartilage lacking perichondrium was partially removed to ensure that the cartilage graft was at least 2 mm wider than the perforation edges. A notch was made in cartilage from which perichondrium had been removed to accommodate the handle of the malleus.
The perforation edges were de-epithelialized using an angled pick. If the perforation involved the malleus, the epithelium was removed from the distal malleus handle. The cartilage–perichondrium graft was pushed through the perforation. Cartilage covered by perichondrium was placed medial to the remnant TM and the anterior annulus in an underlay manner; cartilage lacking perichondrium was placed medial to the posterior bony annulus; the notch in the cartilage graft received the handle of the malleus. The free perichondrium was placed lateral to the handle of the malleus, the posterior bony annulus, and the posterior EAC over a distance of at least 2 mm without elevation of a tympanomeatal flap (Figure 1). Biodegradable NasoPore soaked in antibiotic ointment was used to support the graft medially and laterally. The EAC was packed with gauze soaked in antibiotic ointment up to the tragus incision, which was not sutured.
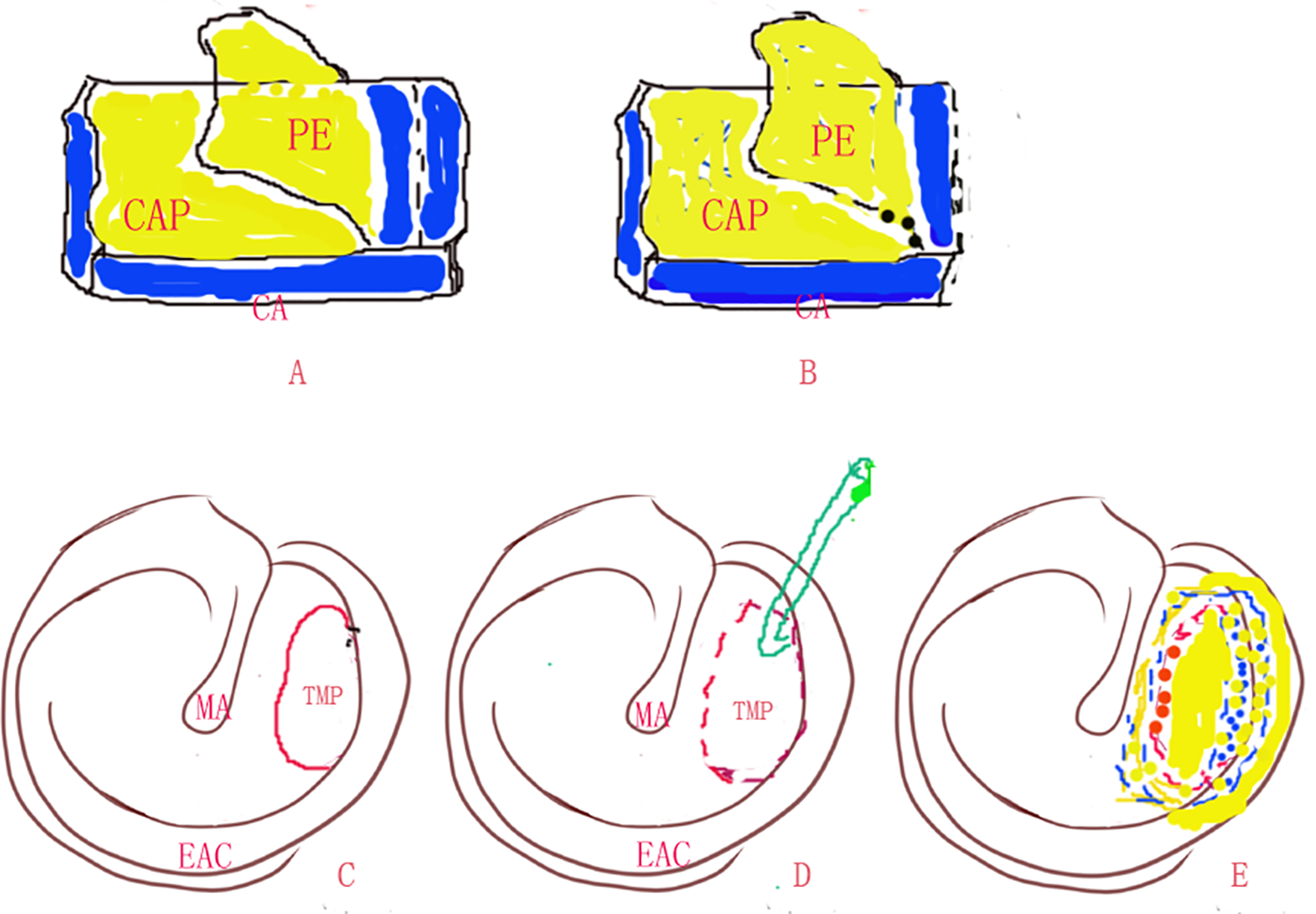
Diagram of surgical procedure. The perichondrium on one side of the composite graft was peeled (A). The cartilage lacking perichondrium was partially removed (B). Preoperative perforation (C). Freshened perforation edges (D). The free perichondrium was placed lateral to the posterior bony annulus and EAC (E). CA, cartilage; CAP, cartilage with single-side perichondrium; EAC, external auditory canal; MA, malleus; PE, perichondrium; TMP, tympanic membrane perforation.
Postoperative Follow-Up
The packing gauze was removed from the EAC 14 days after surgery and biodegradable NasoPore fragments were aspirated from the EAC 3 to 4 weeks after surgery, then the graft could be visualized. All patients were followed up in the outpatient department at 2 weeks. At 1, 3, 6, and 24 months after surgery, endoscopic otological examinations were performed. At the end of the 6th and 24th postoperative month, graft take-up was evaluated endoscopically and the ABGs were examined audiometrically. Any intra- or postoperative complications were recorded. Functional success was defined as an ABG ≤20 dB, and grafting success was an intact graft lacking perforation, retraction, lateralization, significant blunting, and medialization.
Statistical Analyses
Statistical analyses were performed using SPSS ver. 20 software (IBM Inc). The data are expressed as means (SDs) or percentages (%). We compared the pre- and postoperative ABGs using the Wilcoxon signed-rank test. A P value <.05 was considered to indicate statistical significance.
Results
Patient Demographics
We included 31 patients (31; 12 right and 19 left ears; 22 females and 9 males; average age, 47.3 ± 11.8 years) with unilateral, posterior marginal perforations associated with COM. In all, 25 perforations were large and 6 were small; the average perforation duration was 15.7 ± 8.3 years. The tragal incisions healed by postoperative week 2 in all patients. The mean operative time (from the start of surgery after anesthesia induction to EAC packing) was 42.8 ± 11.6 minutes.
Graft Take Rate and Hearing Gain
All patients had follow-up longer than 24 months, with a mean follow-up of 27.9 months (range: 24.2-36.4 months). The graft success rate was 96.7% (30/31) at 6 months and 90.3% (28/31) at 24 months (Figure 2); 1 patient exhibited composite graft extrusion and lateralization near the anterior annulus and a residual perforation (Figure 3). Two patients developed mild otorrhea, which resolved following application of topical ofloxacin otic solution and oral antibiotics. The reperforation occurred in 2 patients at 24 months.
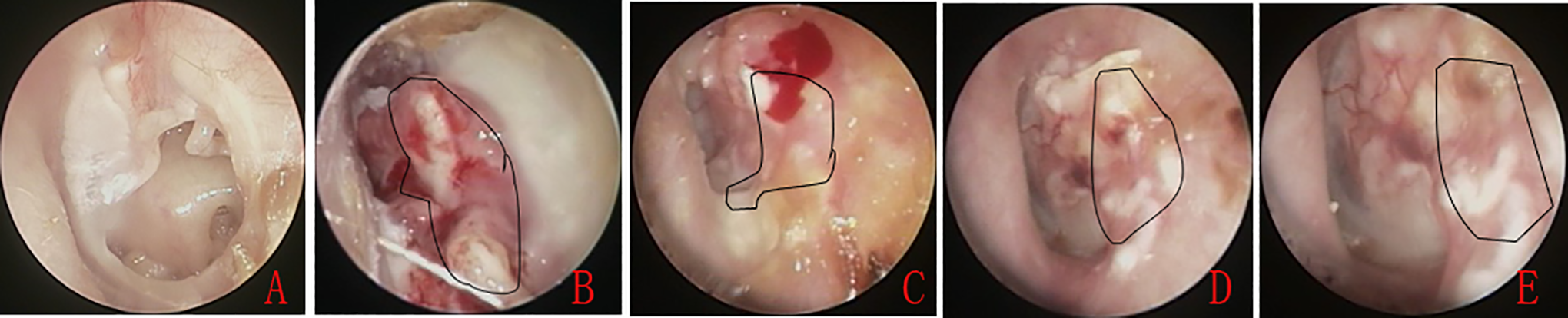
Photographs of the perforation preoperatively (A), at 4 weeks postoperatively (B), at 6 weeks (C), at 7 weeks (D), and at 8 weeks (E). The irregular curve indicates the free perichondrium.
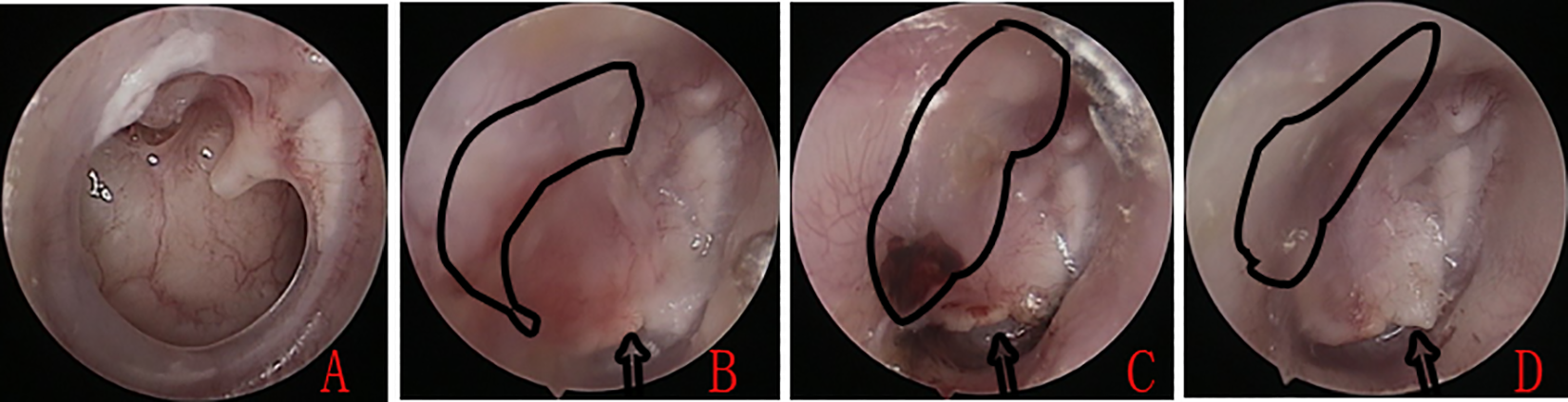
Photographs of the perforation preoperatively (A), at 5 weeks postoperatively (B), at 12 months (C), and at 13 months (D). The irregular curve indicates the free perichondrium. Arrows indicate partial extrusion of the cartilage graft and the residual perforation.
The Wilcoxon signed-rank test revealed that the mean preoperative ABG (28.61 ± 3.14 dB) was significantly greater than the mean postoperative ABG (12.15 ± 3.98 dB; P < .05). Of the 31 patients, 17 (54.8%) exhibited ABG closures of 0 to 10 dB, 13 (41.9%) had closures of 11 to 20 dB, and 1 (3.2%) had a closure of 21 to 30 dB (Table.1). However, there was no statistically significant difference between the post-6 months and post-24 months with regard to ABG values (P = .871), ABG gain (P = .648), or functional success rate (P = .472; Table 1).
Comparison of Hearing Gains and Success Rates Between the Postoperative 6 and 24 Months.

No complications (iatrogenic sensorineural hearing loss, altered taste, facial nerve palsy, vertigo, or tinnitus) were observed during follow-up. No significant graft blunting or atelectasis was noted. The free perichondrium became fully integrated with the skin of the EAC; the perichondrium could not be clearly distinguished endoscopically by 4 to 8 weeks postoperatively (Figure 2). Computed tomography revealed well-pneumatized middle ear at postoperative 24 months in 31 patients (Figure 4).
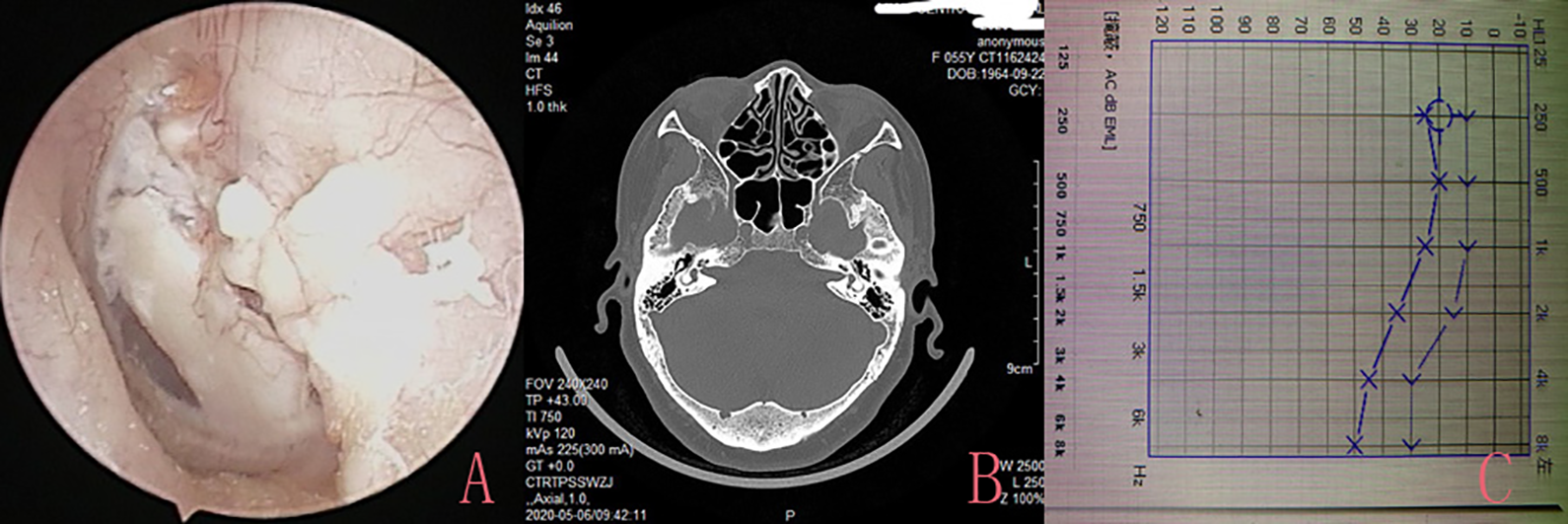
At 36 months postoperatively (A), computed tomography revealed well-pneumatized middle ear (B), pure-tone audiogram at 36 months (C). Please note, this is the same patient as in Figure 2.
Discussion
Recently, some scholars have modified the myringoplastic repair of large marginal perforations; the graft success rates have been low and the complication rates have been high.
Barake et al 1 reported that loop underlay tympanoplasty afforded a closure rate of 99.3%. Panchal et al 2 reported a 95% success rate using over-underlay myringoplasty. Other scholars have reported graft success rates of 95%, 11 90%, 12 and 97.9% 13 using different double-layer graft techniques. Other studies have reported graft take rates of 96.7% 14 and 97.1% 15 after overlay tympanoplasty. 15 However, in these 3 latter studies, although the various techniques indeed enhanced the graft success rate, elevation of posterior EAC skin was mandatory. Our graft success rate was 96.7% (30/31) at 6 months and 90.3% (28/31) at 24 months. In addition, the mean preoperative ABG (28.61 ± 3.14 dB) was significantly greater than the mean postoperative ABG (12.15 ± 3.98 dB; P < .05) at 6 months; 96.7% of patients achieved ABG closures of 0 to 20 dB. However, there was no statistically significant difference between the post-6 months and post-24 months with regard to ABG values, ABG gain, or functional success rate. Thus, our findings are comparable to those of previous studies.
We did not elevate a posterior tympanomeatal flap; free perichondrium was placed lateral to the handle of the malleus, the posterior bony annulus, and the posterior EAC. Although some scholars have developed endoscopic, cartilage tympanoplastic methods employing minimal tympanomeatal flaps,16-18 flap elevation is still required. The absence of tympanomeatal flap elevation reduces the operation time (to a mean of 42.8 ± 11.6 minutes in the present study). We placed the cartilage graft medial to the remnant TM and annulus in an underlay manner; this completely closed the perforation. Free perichondrium that was still attached to the cartilage graft was placed lateral to the posterior EAC. Biodegradable NasoPore packing of the middle ear and EAC supported and strengthened the graft. Theoretically, the EAC perichondrium may tauten the cartilage graft, thus preventing collapse by maintaining intimate contact between the cartilage, the posterior bony annulus, and the remnant TM. We use the largest possible perichondrial flap to cover the EAC. This large flap is in contact with the EAC and the undersurface of the TM and thus nourishes the cartilage graft, enhancing cartilage viability.19,20 Some scholars have reported high graft success rates using butterfly cartilage myringoplasty without tympanomeatal flap elevation. A groove 1 to 2 mm deep created in the cartilage graft is used to anchor the graft to the bony annulus. By contrast, we increased the tension imparted to the free perichondrium of the cartilage graft. Precise creation of the graft groove (which must accurately fit the perforation margins) is time-consuming.
During follow-up, we encountered no complications (further hearing deterioration, a taste change, facial nerve paralysis, vertigo, tinnitus, EAC stenosis, graft medialization, or significant blunting). However, cartilage graft lateralization and extrusion into the anterior annulus were observed in one patient. We may have placed an oversized graft. Our principal concerns were the clinical prognosis and whether the EAC surface perichondrium would develop a cholesteatoma. We in fact found that the perichondrium became fully integrated with the EAC skin to the extent that the “border” was difficult to identify endoscopically. Computed tomography revealed well-pneumatized middle ear and mastoid cavity at postoperative 24 months. We found no cholesteatoma pearls, but further longer-term observation is still needed.
Conclusion
Endoscopic cartilage graft myringoplasty without tympanomeatal flap elevation reliably repairs posterior marginal perforations. The short- and long-term graft success rate is high and the hearing results are satisfactory; the technique is minimally invasive.
Footnotes
Author’s Note
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Science and Technology Agency of Yiwu city, China (Grants#2018-3-76).