
Abstract
A 68-year-old man presented to the Urology Clinic, West China Hospital, Chengdu, with a suspected right adrenal gland mass that had persisted for two months. He had no associated lumbodynia, dizziness or palpitation. Abdominal computed tomography (CT) revealed an uneven density and contrast-enhanced oval-like mass with smooth edges in the right adrenal gland. Laparoscopic right adrenal gland resection followed by histopathology confirmed a diagnosis of metastatic synovial sarcoma. The patient had a history of synovial sarcoma on the right upper leg 3 years previously that was surgically treated, but he had not undergone further treatment. Approximately 1.5 years later, he had undergone surgery for heart and lung metastasis from the synovial sarcoma of the thigh. At 5 months following laparoscopic right adrenal gland resection, abdominal CT showed a significant sign of right adrenal recurrence, and targeted therapy of 12 mg oral anlotinib, daily, was initiated. This relatively rare but alarming case highlights the importance of patient understanding and compliance to treatment.
Keywords
Introduction
Synovial sarcoma is a relatively rare malignant mesenchymal neoplasm that accounts for 5–10% of all soft tissue sarcomas. 1 Predominantly seen in adolescents and the young adult population, the median age for synovial sarcoma is around 35 years. 2 Synovial sarcoma may occur in a multitude of anatomic sites, but mainly affects the lower extremities, with a strong tendency for the para-articular areas. 3 It is a well-defined entity and an aggressive neoplasm that arises from primitive pluripotential mesenchymal cells composed of epithelial and uniform spindle cells, and it has been recognized as a biphasic neoplasm. Synovial sarcoma is driven by the presence of the t (X; 18) (p11.2; q11.2) translocation, which results in the formation of SS18 subunit of BAF chromatin remodelling complex (SS18)-SSX family member (SSX) fusion oncogenes. 4 , 5
Herein, the case of a 68-year-old male patient with classic manifestation and a definite diagnosis of primary synovial sarcoma of the right lower extremity is presented. The patient underwent local resection, but did not undergo further oncology consultation and treatment, and recurrence involving metastasis of the synovial sarcoma to the lung, heart and right adrenal gland occurred within 3 years of primary diagnosis. This case represents a caution to the clinician and patient to carefully consider the implications of the patient failing to undergo recommended assessments and treatment.
The study was approved by the Ethics Committee on Biomedical Research, West China Hospital of Sichuan University, approval No. 2021(183). Verbal informed consent to publish the case report was obtained from the patient.
Case report
A 68-year-old male presented to the Urology Clinic of West China Hospital, Chengdu, China, in January 2019, with a 2-month history of right adrenal gland mass on the abdominal computed tomography (CT) scan. He had no other symptoms or signs, and the systemic review was negative. Blood pressure was measured at 124/78 mmHg, and serum norepinephrine (660 ng/l; reference range, 272–559 ng/l) and epinephrine (84 ng/l; reference range, 54–122 ng/l) were elevated. Enhanced abdominal CT confirmed a 3.4 × 2.1-cm, well-defined oval-shaped mass in the right adrenal gland, with a smooth edge and heterogeneous enhancement (Figure 1). Laparoscopic right adrenal resection was performed, and general observation of the postoperative specimens revealed a 5.0 × 4.0-cm lobulated mass with aggressive margin. Immunohistochemical (IHC) analysis showed that the tumour cells were negative for chromogranin A (CgA), synaptophysin (Syn), activin receptor-like kinase 1 (ALK-1), melanoma‐associated antigen recognized by T cells 1 (MART-1), teratocarcinoma-derived growth factor 1 (CR), inhibin-α, S100 calcium binding protein B (S-100), HMB45 (a marker for premelanosome protein), cytokeratin (CK), epithelial membrane antigen (EMA), CD34 molecule, platelet and endothelial cell adhesion molecule 1 (CD31), desmin, and smooth muscle actin (SMA), but positive for succinate dehydrogenase complex iron sulfur subunit B (SDHB) expression. In-situ hybridization showed that cells were negative for Epstein-Barr virus-encoded RNA 1 and 2 (EBER1/2). The final postoperative pathology-based diagnosis was an infiltrating malignant tumour with necrosis (Figure 2) that was a metastatic sarcoma of the right thigh.
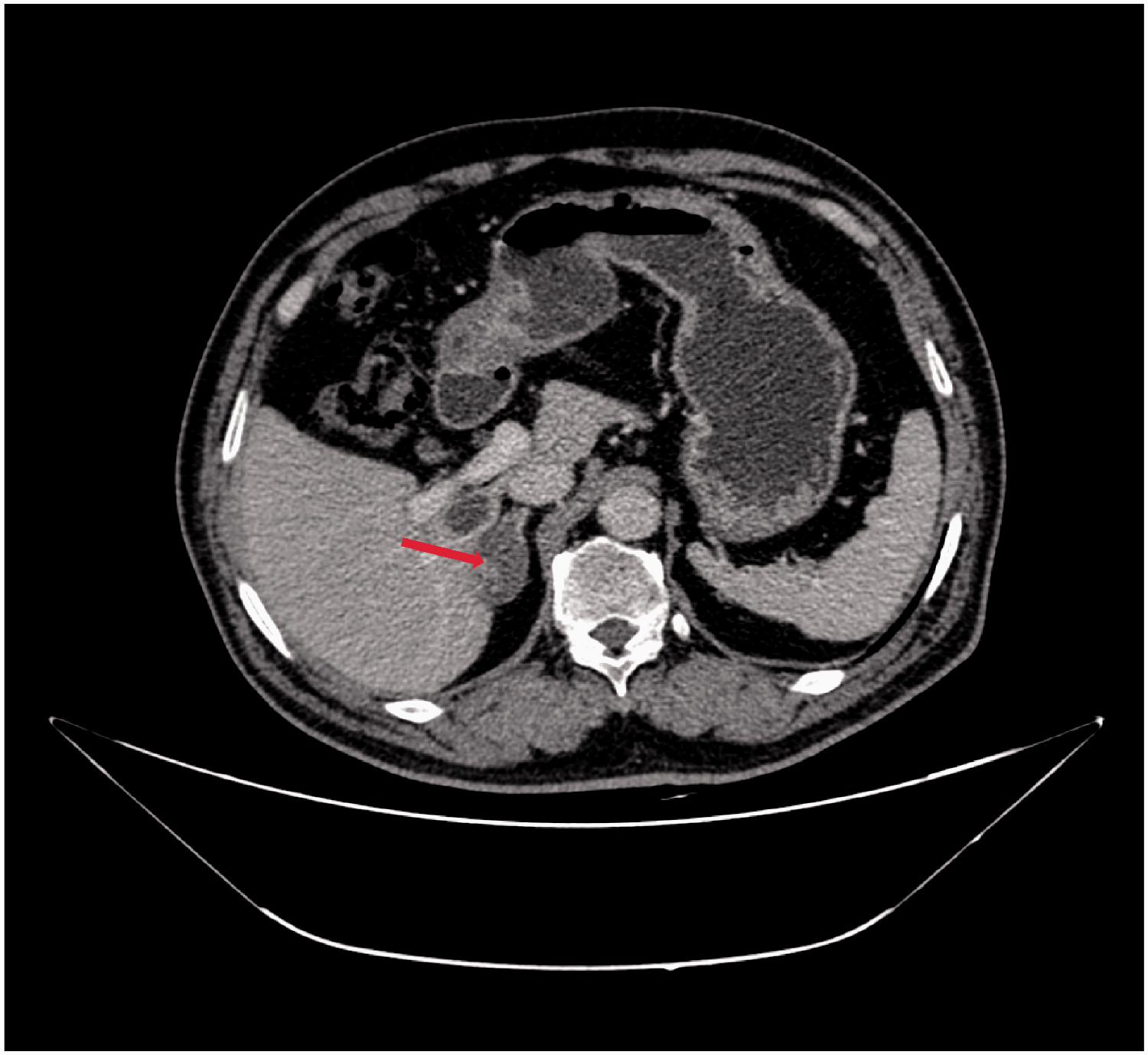
Abdominal enhanced computed tomography scan showing a low-density oval mass in the right adrenal gland with smooth edges, uneven density and contrast enhancement (red arrow).

Haematoxylin and eosin-stained section of the resected right adrenal gland showing infiltrating tumour cells and necrosis (original magnification, × 100).
Review of the patient’s past medical history revealed that he had undergone a mass en-bloc resection in the right lower extremity in February 2016, approximately 3 years earlier (Figure 3), with no evidence of metastatic disease before the surgery. The primary pathology diagnosis was strongly considered to be synovial sarcoma, French National Federation of Cancer Control Centres (FNCLCC) grade 3. IHC analysis at that time showed that the primary tumour was negative for CD34, desmin, pan-CK, and EMA, and moderately positive for murine double minute 2 (MDM2), cyclin dependent kinase inhibitor 2A (P16), TLE family member 1, transcriptional corepressor (TLE-1), and SMA, with a Ki-67 index of 40% (Figure 4). Fluorescence in situ hybridization (FISH) was suggested to detect MDM2 and the SS18 gene to further confirm the diagnosis and therapeutic considerations, however, the patient declined further tests and treatment. At 1.5 years following the primary tumour resection, he presented to the Cardiac Surgery Clinic of West China Hospital with a 2-week history of bilateral lower limb oedema. Positron emission tomography (PET)/CT showed right pulmonary nodules, observed in the right superior pulmonary vein and some of its branches, and a high possibility of left atrial thrombosis (Figure 5). Combined evidence indicated likely synovial sarcoma metastasis. Echocardiography further confirmed a left atrial mass and mitral obstruction, however, left ventricular systolic function was normal. The patient was classified as New York Heart Association functional class III. He received right superior and middle lobectomy, and open-heart surgery with left atrial tumour resection and patent foramen ovale repair. IHC analysis of the left atrial tumour cells revealed moderate positivity for EMA, MDM2, SMA, and TLE-1, and negative results for desmin, S-100, CR and CD34 (Figure 6). Morphology and IHC results supported the diagnosis of synovial sarcoma, FNCLCC grade 3, but this required further confirmation using FISH to detect MDM2 and the SS18 gene. Postoperative pathology confirmed that the right lung tumour was the metastasised sarcoma, however, the patient remained objective to chemotherapy. At the time of writing, the patient had not undergone genetic testing to further confirm the diagnosis, but based on morphological and immunostaining analyses, medical history and clinical manifestation, he was given a primary diagnosis of synovial sarcoma. During the previous 4 years, the patient experienced right medial thigh synovial sarcoma with consecutive lung, heart and right adrenal gland metastasis, which is quite rare. At 5 months following laparoscopic right adrenal resection, an abdominal CT scan showed signs of significant right adrenal recurrence, resulting in the initiation of targeted therapy with 12 mg oral anlotinib, daily. The reporting of this study conforms to CARE guidelines. 6

Magnetic resonance image showing a T2-weighted hyperintense solid mass involving the right lower thigh (red arrow).

Representative immunohistochemistry images of primary thigh tumour tissue sections showing moderate positivity for: (a) cyclin dependent kinase inhibitor 2A (P16); (b) murine double minute 2 (MDM2); and (c) smooth muscle actin (SMA); and (d) Ki-67 index of 40% (original magnification, × 100).

Enhanced thoracic computed tomography scan showing the mitral orifice obstructed by a left atrium solid mass with uniform density (red arrow).
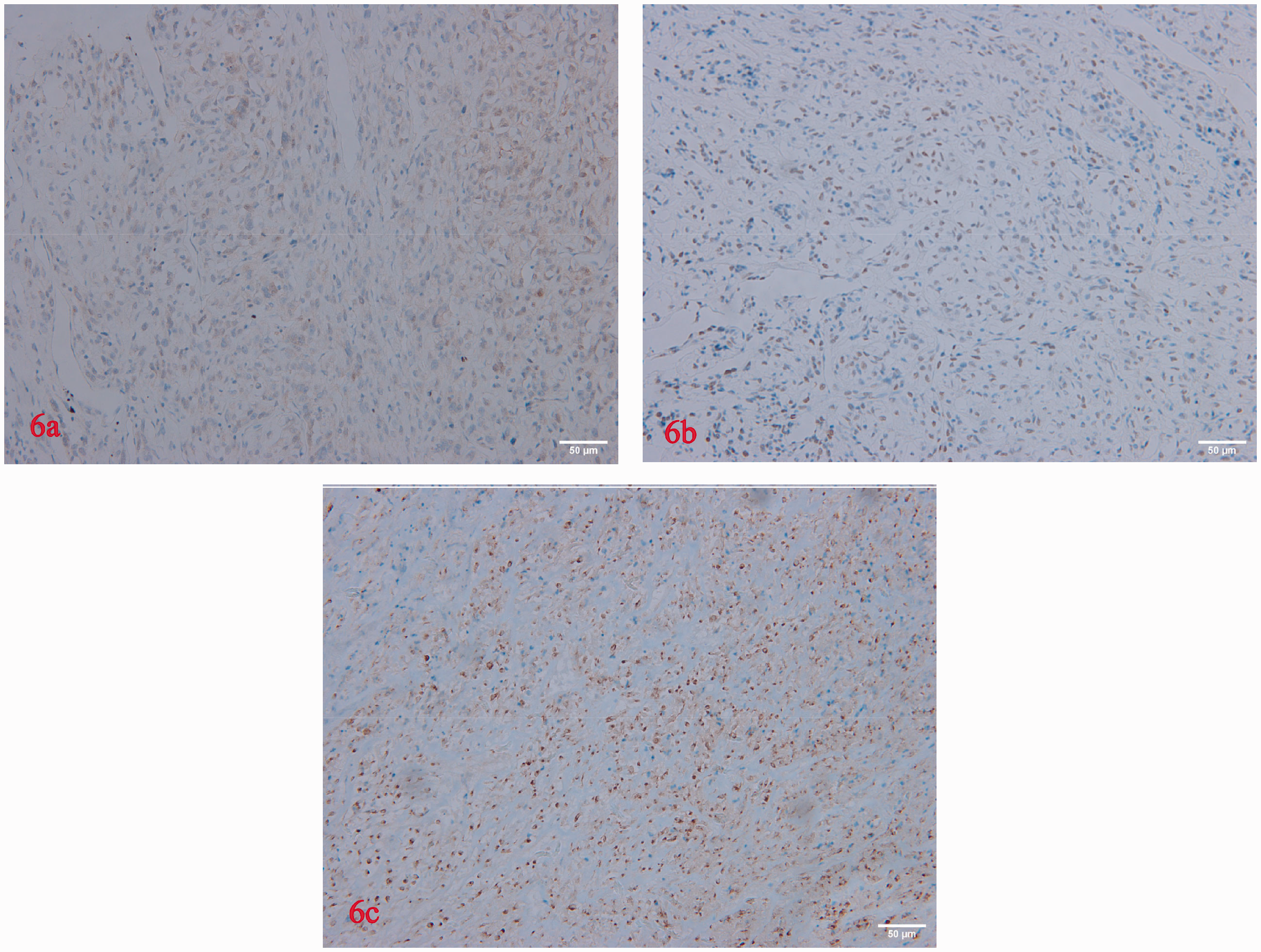
Representative immunohistochemistry images of left atrial tumour tissue sections showing moderate positivity for: (a) murine double minute 2 (MDM2); (b) TLE family member 1, transcriptional corepressor (TLE-1); and (c) epithelial membrane antigen (EMA) (original magnification, × 200).
Discussion
Synovial sarcoma may occur at almost any anatomic site, 5 including the lungs, kidneys, cerebellum, parapharyngeal region, and heart. Cases of intraprostatic synovial sarcoma have also been reported in the literature.7–10 The overall prognosis of primary metastatic synovial sarcoma remains poor, with a metastases rate of 25%, and a 48% rate of recurrence. 11 , 12 The standard approach to treating synovial sarcoma is wide surgical excision combined with radiotherapy, with or without (neo)adjuvant chemotherapy, as appropriate. However, (neo)adjuvant chemotherapy in such cases remains controversial. Advanced stage synovial sarcoma has been reported to have a better response to systemic chemotherapy than other soft tissue sarcoma subtypes.13–15
The present case is relatively complicated, as the differential diagnosis was difficult to achieve with pathology and depended on FISH results to inform the patient's further treatment and potential outcome. The patient was advised by pathologists to undergo FISH assessment on more than two occasions, but he declined. The disease course and outcome has been poor for this patient, despite a localized disease when he was first admitted to hospital. This rare tumour type requires more study in terms of clinical and pathological diagnosis. The present case is complicated by the fact that first, during the course of disease, the patient presented with a malignant tumour manifestation with multiple distant metastases, but did not visit subsequent clinics nor the oncology clinic for further treatment. Secondly, the patient had three surgeries in different surgical departments. Doctors need to pay more attention to doctor-patient communication and health education to improve patients' health consciousness, and encourage patients to proactively seek comprehensive treatment. Lastly, in such situations, difficult and time-consuming pathological diagnoses should be solved promptly.
The present case is a caution for both patients and clinicians. Noncompliance may be the leading cause of this patient’s adverse disease course. Medical professionals should apply more patience and consideration in educating patients, so that patients fully understand the implications of accepting or rejecting recommended assessments and treatments.
Footnotes
Acknowledgements
We are thankful for the efforts of the Urology Department of Sichuan University West China Hospital, and we greatly appreciate the assistance of Dr Cui Chi, Department of Vascular Surgery, the Third People's Hospital of Chengdu, Sichuan, China.
Author contributions
Lisha Jiang and Qingxin Ma drafted the manuscript. Lisha Jiang, Guonian Zhu, Xiaoqin Lai and Qian Liu acquired the clinical data. Hongsheng Ma and Ming Shi designed and revised this work. All authors approved the final version of the manuscript for publication.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.